Harkins S, Marteney JL, Cueva O, Cueva L. Application of soft occlusal splints in patients suffering from clicking temporomandibular joints. Cranio. 1988; 6:71-76
Stapelmann H, Türp JC. The NTI-tss device for the therapy of bruxism, temporomandibular disorders, and headache – Where do we stand? A qualitative systematic review of the literature. BMC Oral Health. 2008; 8
Moufti MA, Lilico JT, Wassell RW. How to make a well-fitting stabilisation splint. Dent Update. 2007; 34:398-408
Longridge NN, Milosevic A. The bilaminar (dual-laminate) protective night guard. Dent Update. 2017; 44:648-654
Davies SJ, Gray RJ. The pattern of splint usage in the management of two common temporomandibular disorders. Part I: The anterior repositioning splint in the treatment of disc displacement with reduction. Br Dent J. 1997; 183:199-203
Kai S, Kai H, Tabata O, Tashiro H. The significance of posterior open bite after anterior repositioning splint therapy for anteriorly displaced disk of the temporomandibular joint. Cranio. 1993; 1:146-152
Lobbezoo F, Ahlberg J, Glaros AG Bruxism defined and graded: an international consensus. J Oral Rehabil. 2013; 40:2-4
International Classification of Sleep Disorders, 3rd edn. Darien, IL: American Academy of Sleep Medicine; 2014
Manfredini D, Ahlberg J, Winocur E, Lobbezoo F. Management of sleep bruxism in adults: a qualitative systematic literature review. J Oral Rehabil. 2015; 42:862-874
Dubé C, Rompré PH, Manzini C, Guitard F, de Grandmont P, Lavigne GJ. Quantitative polygraphic controlled study on efficacy and safety of oral splint devices in tooth-grinding subjects. J Dent Res. 2004; 83:398-403
Harada T, Ichiki R, Tsukiyama Y, Koyano K. The effect of oral splint devices on sleep bruxism: A 6-week observation with an ambulatory electromyographic recording device. J Oral Rehabil. 2006; 33:482-488
Nascimento LL, Amorim CF, Giannasi LC Occlusal splint for sleep bruxism: an electromyographic associated to Helkimo Index evaluation. Sleep Breath. 2008; 12:275-280
Van der Zaag J, Lobbezoo F, Wicks DJ, Visscher CM, Hamburger HL, Naeije M. Controlled assessment of the efficacy of occlusal stabilization splints on sleep bruxism. J Orofac Pain. 2005; 19:151-158
Okeson JP. The effects of hard and soft occlusal splints on nocturnal bruxism. J Am Dent Assoc. 1987; 114:788-791
Baad-Hansen L, Jadidi F, Castrillon E, Thomsen PB, Svensson P. Effect of a nociceptive trigeminal inhibitory splint on electromyographic activity in jaw closing muscles during sleep. J Oral Rehabil. 2007; 34:105-111
Peck CC, Goulet JP, Lobbezoo F Expanding the taxonomy of the diagnostic criteria for temporomandibular disorders. J Oral Rehabil. 2014; 41:2-23
Al-Ani MZ, Gray RJ, Davies SJ, Sloan P, Glenny AM. Stabilization splint therapy for the treatment of temporomandibular myofascial pain: a systematic review. J Dent Educ. 2005; 69:1242-1250
Dao TT, Lavigne GJ. Oral splints: the crutches for temporomandibular disorders and bruxism?. Crit Rev Oral Biol Med. 1998; 9:345-361
Türp JC, Komine F, Hugger A. Efficacy of stabilization splints for the management of patients with masticatory muscle pain: a qualitative systematic review. Clin Oral Investig. 2004; 8:179-195
Fricton J, Look JO, Wright E Systematic review and meta-analysis of randomized controlled trials evaluating intraoral orthopaedic appliances for temporomandibular disorders. J Orofac Pain. 2010; 24:237-254
Klasser GD, Greene CS. Oral appliances in the management of temporomandibular disorders. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009; 107:212-223
Durham J. Summary of Royal College of Surgeons (England) clinical guidelines on management of temporomandibular disorders in primary care. Br Dent J. 2015; 218:355-356
Greene CS. Managing the care of patients with temporomandibular disorders: a new guideline for care. J Am Dent Assoc. 2010; 141:1086-1088
Occlusal splints are classified in this article into three groups according to the way that opposing teeth contact the splint: 1) partial occlusal contact; 2) full occlusal contact in retruded arc of closure; and 3) full occlusal contact in protrusion. Each type of splint has relative advantages and disadvantages. Splints do not reliably or predictably reduce bruxism and there are differences between individuals in their response to the wearing of splints. When treating temporomandibular disorders, splints should be provided as part of a package of conservative physiotherapy type measures. There is no evidence that any one type of splint is most effective. Long-term wearing of designs that may lead to permanent occlusal changes should be avoided or the patient should be carefully monitored for occlusal changes.
CPD/Clinical Relevance: The article describes the effect of splints on bruxism. Advice is provided on best practice in respect of the use of splints in the management of temporomandibular disorders.
Article
Occlusal splints
Occlusal splints are interocclusal appliances commonly used in dental practice to manage bruxism and temporomandibular disorders (TMD). There are many articles and studies on the effectiveness of occlusal splints. Many of the articles provide only opinions and many of the studies are not well designed and include different types of patients followed over different periods of time with different assessment and outcome criteria. There is also a large amount of web-based information regarding treatment of TMD with splints, much of which is inaccurate and misleading. This, unsurprisingly, has led to confusion about the value of dental occlusal splints.
The purpose of this article is to describe the different types of occlusal splints and to examine the evidence relating to their effectiveness in managing bruxism and TMD.
Types of occlusal splints
Many types of occlusal splints have been described. They may be classified according to the material from which they are made or by whether they cover some or all the teeth in the dental arch. More usefully, they can be classified into three general groups according to the way that opposing teeth contact the splint:
Full occlusal contact in retruded arc of closure (often termed ‘stabilizing’ splint);
Anterior repositioning splint.
Table 1 shows the three groups of splints and gives examples of each type. Examples in each group are discussed below.
Partial Occlusal Contact (Relaxation Splints)
Full Occlusal Contact in Retruded (Stabilizing Splints)
Full Occlusal Contact in Protrusion (Anterior Repositioning Splints)
Soft splint
Michigan splint
Maxillary
SCi
Tanner appliance
Anterior bite plane
Hard thermoformed splint
Mandibular
Gelb splint (posterior bite plane)
Laminate thermoformed splint
Partial occlusal contact (relaxation) splints
Partial occlusal contact splints cover some or all teeth in one arch. When the mouth closes, limited tooth contacts are made in any mandibular position, including retruded contact position. Prolonged use of this type of splint can result in changes in the dental occlusion.1
Soft splint
All teeth are covered by the splint, which can be made on the maxillary or mandibular arch (Figure 1). Soft splints are made by thermoforming a blank polyvinylacetate-polyethylene sheet (3 mm or 4 mm) onto a dental cast. No occlusal adjustment is made. As a result of the hinge arc of closure of the mandible, initial tooth contact will be on the posterior part of the splint.
Figure 1. Soft splint.
Advantages of this type of splint are that it has reasonable acceptance and is relatively cheap and easy to make. Disadvantages are that it is relatively bulky, it may need frequent replacement due to deterioration, particularly in a patient with sleep bruxism, and it has the potential for producing a posterior open bite.1
Anterior bite plane
An anterior bite plane is a soft or hard splint covering anterior teeth only (Figure 2). Contacts are made by at least four opposing incisor teeth to prevent overloading teeth. An anterior open bite may develop due to over-eruption of posterior teeth.
Figure 2. Anterior bite plane.
SCi (Sleep Clench inhibitor)
This appliance was previously called the Nociceptive Trigeminal Inhibition Tension Suppression System (NTI-tss). This is a small commercially produced anterior bite plane (modified by the dentist at the chairside) that covers the incisor teeth (usually in the maxilla) only (Figure 3). It is said to stimulate the periodontal ligament to activate feedback in order to reduce the contraction intensity of the muscles of mastication. Occlusal changes have been noted.2 Due to the size, it is susceptible to being swallowed or inhaled.
Figure 3. SCi type splint.
Full occlusal contact (stabilizing) splints
The stabilizing splint aims to provide a stable occlusion where retruded contact position is the same as intercuspal contact position. It is constructed on an articulated dental cast and adjusted so that there are equal bilateral contacts in the retruded contact position. The conventional stabilizing splint has a flat occlusal surface and has balanced contacts in lateral excursions. The stabilizing splint is more robust than the soft splint and will not produce occlusal changes. It is, however, more time-consuming and technique sensitive and is therefore more expensive to produce.
Michigan splint
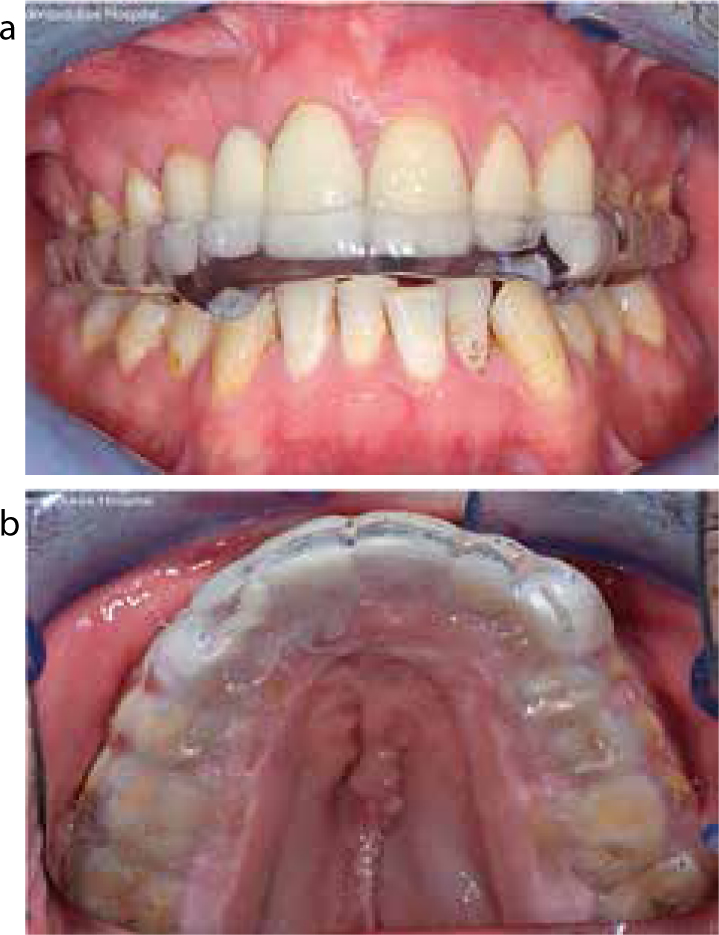
This type of splint is constructed from acrylic resin on the upper arch. It produces what may be considered an ideal occlusion. Ramping is created on the splint to give canine protection in lateral excursions and equal bilateral incisal contacts, giving posterior disclusion in protrusion. There are no non-working side occlusal contacts (Figure 4). Construction and use of this form of splint has been described in detail by Moufti et al.3
Figure 4. Michigan splint: (a) in occlusion retruded contact; (b) occlusal view. (Courtesy of Dr Andrew Barber).
Tanner appliance
This has very similar features to the Michigan splint but is constructed for the mandibular arch.
Thermoformed splint
This type of splint is less widely used. It is made of a hard material (eg Erkodur, EM Natt, London, UK) or from a hard and soft laminate disc (eg Erkoloc-Pro, EM Natt, London, UK). The thermoformed splints are relatively easy to construct and fit. A laminate splint may be more comfortable for patients to wear than a hard splint. Laminate splints, however, are less durable and are liable to split posteriorly.
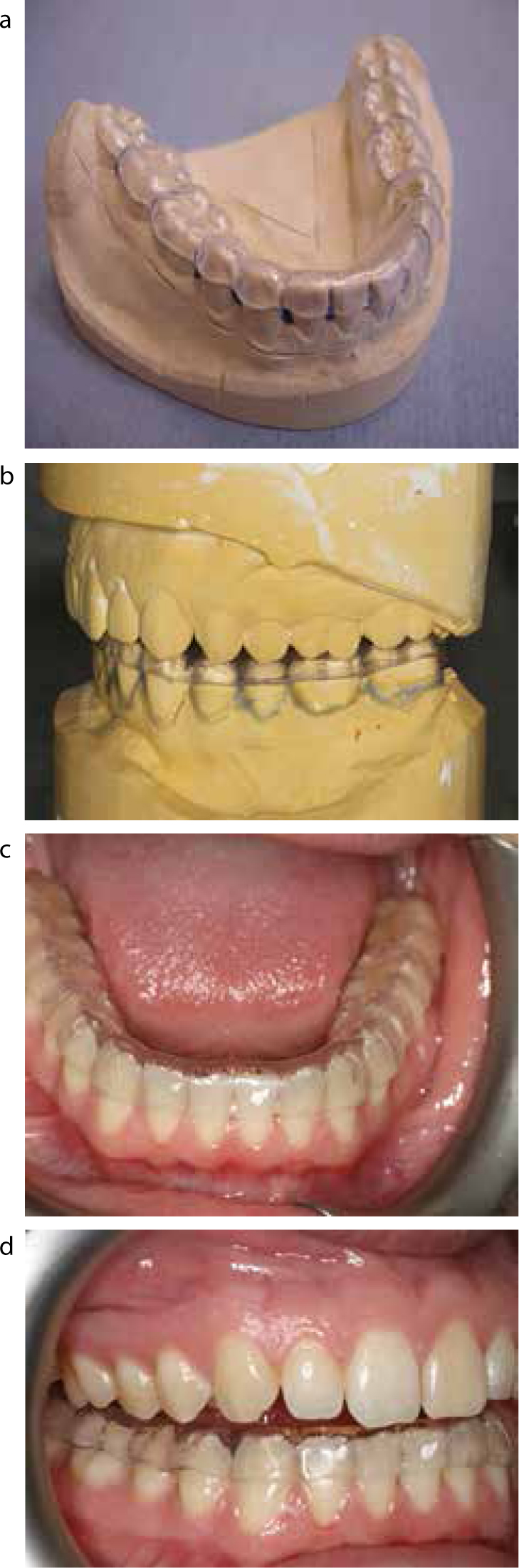
The construction of the laminate splint and its use in the management of tooth wear has been described by Longridge and Milosevic.4 The hard thermoformed splint is made in a similar way. Thermoformed splints are adjusted in the laboratory and/or in the clinic to ensure that maximum bilateral contacts are made in retruded contact (Figure 5).
Figure 5. Thermoformed splint: (a) trimmed on the cast; (b) occlusal adjustment on the articulator; (c) in the mouth (occlusal view); (d) in the mouth.
The occlusal surface of certain thermoformed materials, eg Erkolok Pro, EM Natt, London, UK, can be modified by the technician in the laboratory or at the chairside by the clinician by adding autopolymerizing acrylic resin to provide features of a Michigan splint, including anterior ramping that will provide canine guidance in lateral excursions and posterior disclusion in protrusion.
Anterior repositioning splints
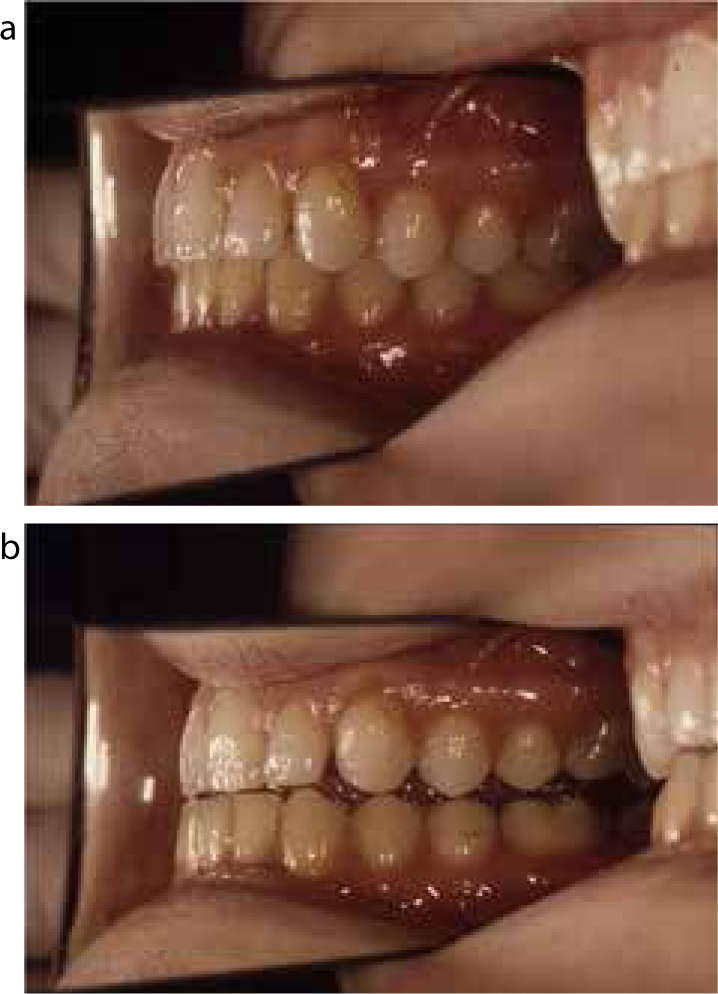
This type of splint is sometimes called a protrusion splint. As in the case of the stabilizing splint, even contact of all opposing teeth can be made with the splint. The splint, however, holds the lower jaw forward to give maximum contact in a protrusive position (Figure 6). The aim of the splint is to re-capture an anteriorly displaced disc preventing further disc displacement and pain and clicking of the temporomandibular joint. It is usually constructed on the upper arch with ramping to slide the mandibular teeth to the more anterior position. It must be worn full time for an extended period. Anterior repositioning splints have been described by Davies and Gray.5 They have the potential for occlusal change, particularly a posterior open bite.6 They are used specifically for painful disc displacements. They are not commonly used and will not be discussed in more detail in this article.
Figure 6. Anterior repositioning splint: (a) intercuspal occlusion; (b) maximum intercuspation in protrusion on the splint. (Courtesy of Mr Stephen Davies).
The effects of splints on bruxism
Bruxism is the repetitive, sustained habitual clenching and/or grinding of the teeth and/or bracing or thrusting the mandible.7 It is classified into primary and secondary bruxism.
Primary bruxism can occur as awake bruxism (AB) or sleep bruxism (SB). AB is considered to be a concentration or stress-related activity or parafunction. Sleep bruxism is a sleep movement disorder.8 Some individuals may exhibit both AB and SB. Secondary bruxism is associated with medical conditions including cerebral palsy and learning difficulties, or it can be a side-effect of various medications and illicit drugs.
Bruxism is associated with a wide range of detrimental effects such as tooth wear, damage to restorations and TMD. It can also cause tooth contact noises that can be unpleasant for partners of those who have SB.
Available evidence is that occlusal splints do not reliably or predictably prevent or reduce SB. A finding of a systematic review of the literature was that evidence-based recommendations on management of SB at the individual level are not available.9
Studies on SB have given contradictory results. Two studies showed a reduction in SB with stabilizing type splints.10,11 In both these studies, however, a similar reduction was obtained with comparison appliances that covered only the palate.
In two other studies, neither occlusal nor palatal splints were found to influence the SB outcome variable.12,13 One of the studies,13 however, noted that variable SB outcomes were found in individual cases. Some patients had a decrease in masticatory muscle activity, while others showed no change or an increase.
A variable individual effect was also shown by Okeson.14 He investigated the effects of both hard and soft occlusal splints on night-time muscle activity in 10 subjects. Soft polyvinyl splints were found to increase masseter and temporalis muscle activity in many subjects, reducing muscle activity in only one participant while causing a statistically significant increase in muscle activity in five of the ten participants. The hard (full contact stabilizing type) occlusal splint significantly reduced muscle activity in eight of the ten participants.
There is little information about the effect of anterior bite planes on bruxism. One study, however, indicated a strong inhibitory effect on muscle activity in jaw closing muscles during sleep of the SCi part-coverage type splint compared with a stabilizing type splint.15 It may be concluded therefore that splints do not reliably or predictably reduce SB and that there are probably individual differences in response to the wearing of a splint.
The effects of splints on temporomandibular disorders (TMD)
Temporomandibular disorders (TMD) are a range of conditions that affect the TMJ and/or the muscles of mastication. The commonly occurring TMD are myalgia, arthralgia and disc derangements.16 These presentations have been known by a wide variety of names including TMJ dysfunction and myofascial pain. Whilst mild symptoms are common, TMD is said to affect 5–12% of the population.17
There have been a number of scientific reviews of articles relating to splint treatment for TMDs18,19,20, 21 and the findings of these can be summarized as follows.
Splints are an effective treatment method for TMDs. Splints have not been shown to be more effective than other forms of treatment including, for example, stress management, jaw exercises and acupuncture.
The mechanism(s) for the benefits that splints provide is not clear. It is not certain that improvement of pain symptoms after incorporation of the intra-oral appliance is caused by a specific effect of the appliance, such as changes in occlusal contacts or occlusal vertical dimension.
It is also important to note that the effect of a splint on bruxism does not necessarily correlate with reduction of TMD associated pain. Nascimento et al found that, although there was no significant decrease in mean masticatory muscle activity of SB subjects using stabilizing type splints, a significant decrease in TMD signs and symptoms was observed after 60 days of use.12
Similarly, in the study of Baad-Hansen et al15 reduction in masticatory muscle activity with the SCi splint compared to the stabilizing splint was not directly related to pain reduction.
There is no evidence that any specific type of splint is most effective. A stabilization type splint does not appear to be more effective than a soft splint, an anterior bite plane type splint, or even a non-occluding palatal splint. As previously mentioned, several studies have reported occlusal changes associated with the use of partial occlusal contact splints and with the anterior repositioning splints. A clinical observation by the authors is that soft splints can exacerbate pain and locking in some patients, but that it is very unusual for that to happen with stabilizing type splints. It has been recommended that soft splints can be useful for short-term treatment, whilst stabilizing splints are more appropriate for long-term use because of their relative robustness and low risk for occlusal change.22
Contemporary guidelines for management of TMD state that local conservative physiotherapy type measures are used as a first line of management, which includes resting the TMJ and muscles (by avoiding chewing hard foods, etc), jaw exercises and heat application.23,24-25 Splint therapy is recommended as a measure that can be used to supplement these local measures.
Full-time wear or long-term wear of specific designs that lead to permanent occlusal changes should be avoided. If partial contact splints, such as soft splints, are worn long-term, the dental occlusion should be carefully monitored. The worst case outcome with use of splints should be nothing more than a failure to relieve symptoms.22
Good practice dictates that clinical records are kept, including diagnosis, discussion of treatment options and informed consent.
Records should be made of follow-up appointments, including review of symptoms and examination of the mouth, to ensure that there are no adverse effects, and an assessment of the condition of the splint.
Summary
This article has classified splints into partial occlusal contact splints, full occlusal contact splints in retruded position and full occlusal contact in protrusion (anterior repositioning splint), according to the way teeth in the opposing arch make contact. Of these, the anterior repositioning splints are not widely used.
The effects of splints on bruxism are not well understood. There is no evidence that splints reliably prevent either awake or sleep bruxism.
When used to manage TMD, splints should be used as part of a ‘package’ of physiotherapy type measures. There is little evidence that one type of splint is more effective than another.
Soft splints are widely used as they are inexpensive and easy to make but are also relatively susceptible to perforation by bruxing. They may exacerbate TMD symptoms and, like other partial occlusal contact splints and anterior repositioning splints, they may produce occlusal changes.