Postlethwaite KR, Hamilton M. Multiple idiopathic external root resorption. Oral Surg Oral Med Oral Pathol. 1989; 68:640-643
Rivera EM, Walton RE. Extensive idiopathic apical root resorption. A case report. Oral Surg Oral Med Oral Pathol. 1994; 78:673-677
Bakland LK. Root resorption. Dent Clin North Am. 1992; 36:491-507
Fuss Z, Tsesis I, Lin S. Root resorption – diagnosis, classification and treatment choices based on stimulation factors. Dent Traumatol. 2003; 19:175-182
Benenati FW. Root resorption: types and treatment. Gen Dent. 1997; 45:42-45
Ne RF, Witherspoon DE, Gutmann JL. Tooth resorption. Quintessence Int. 1999; 30:9-25
Tronstad L. Root resorption-etiology, terminology and clinical manifestations. Endod Dent Traumatol. 1988; 4:241-252
Trope M. Root resorption of dental and traumatic origin: classification based on etiology. Pract Periodont Aesthet Dent. 1998; 10:515-522
Andreasen JO, Hjorting-Hansen E. Replantation of teeth. Part I. Radiographic and clinical study of 110 human teeth replanted after accidental loss. Acta Odontol Scand. 1966; 24:263-286
Heithersay GS. Invasive cervical resorption. Endod Topics. 2004; 7:73-92
Brezniak N, Wasserstein A. Orthodontically induced inflammatory root resorption. Part I: The basic science aspects. Angle Orthod. 2002; 72:175-179
Löe H, Waerhaug J. Experimental replantation of teeth in dogs and monkeys. Arch Oral Biol. 1961; 3:176-184
Kerr DA, Courtney RM, Burkes EJ. Multiple idiopathic root resorption. Oral Surg. 1970; 29:552-565
Soni NN, La Velle WE. Idiopathic root resorption. Oral Surg Oral Med Oral Pathol. 1970; 29:387-389
Di Domizio P, Orsini G, Scarano A, Piattelli A. Idiopathic root resorption: report of a case. J Endod. 2000; 26:299-300
Schätzle M, Tanner SD, Bosshardt DD. Progressive, generalized, apical idiopathic root resorption and hypercementosis. J Periodontol. 2005; 76:2002-2011
Cholia SS, Wilson PH, Makdissi J. Multiple idiopathic external apical root resorption: report of four cases. Dentomaxillofac Radiol. 2005; 34:240-246
Moazami F, Karami B. Multiple idiopathic apical root resorption: a case report. Int Endod J. 2007; 40:573-578
Liang H, Burkes EJ, Frederiksen NL. Multiple idiopathic cervical root resorption: systematic review and report of four cases. Dentomaxillofac Radiol. 2003; 32:150-155
Pinska E, Jarzynka W. Spontaneous resorption of the roots of all permanent teeth as a familial disease. Czas Stomatol. 1966; 19:161-165
Newman WG. Possible etiologic factors in external root resorption. Am J Orthod. 1975; 67:522-539
Polder BJ, Van't Hof MA, Van der Linden FP, Kuijpers-Jagtman AM. A meta-analysis of the prevalence of dental agenesis of permanent teeth. Community Dent Oral Epidemiol. 2004; 32:217-226
Jarvinen S, Vaataja P. Congenitally missing maxillary permanent cuspids. Report of a case. Proc Finn Dent Soc. 1979; 75:11-12
Hunstadbraten K. Hypodontia in the permanent dentition. J Dent Child. 1973; 40:115-117
Créton MA, Cune MS, Verhoeven W, Meijer GJ. Patterns of missing teeth in a population of oligodontia patients. Int J Prosthodont. 2007; 20:409-413
Marx RE, Garg AK. Bone structure, metabolism, and physiology: its impact on dental implantology. Implant Dent. 1998; 7:267-276
Trope M. Clinical management of the avulsed tooth. Dent Clin North Am. 1995; 39:93-112
Multiple idiopathic external root resorption is an unusual condition that may present in a cervical or an apical form. In this paper, we review the published literature relating to root resorption and multiple idiopathic external apical root resorption (MIEARR). The article considers the types, classification and aetiology of root resorption and discusses the restorative options and management. An example of a patient suffering with multiple idiopathic apical external apical root resorption affecting UR2, UR1, UL1, UL2 and hypodontia affecting the maxillary canines is described.
Clinical Relevance: This paper offers clinical advice to practitioners to understand the classification of root resorption and appropriate and timely referral to be made to secondary care for optimum restorative treatment when multiple teeth are involved with no known cause established.
Article
History, types and classification
Root resorption in deciduous teeth is a normal physiological response, resulting in exfoliation of the deciduous teeth with replacement by the permanent dentition. In contrast, the process of root resorption in the permanent dentition has a pathological basis. The resorption of permanent teeth was first described by Bates in 1856, who considered the cause to be trauma to the periodontal membrane.1 Root resorption is classified as external and internal, the former being reported more often.2 Root resorption of permanent teeth has been attributed to a wide variety of causes, such as trauma, inflammation, tooth re-implantation, tumours, cysts, occlusal stress, impacted teeth,3 orthodontic movement,4 periodontitis and dietary habits.5,6 Resorption of the roots can also be related to endocrine disturbances and systemic conditions, such as hyperparathyroidism, hypoparathyroidism, hypophosphataemia, hyperphosphataemia, Gaucher's disease, Paget's disease of bone, Goltz syndrome, Papillon-Lefèvre syndrome and Turner syndrome.7 However, Henry and Weinmann highlighted that minimal apical resorption may be present in all permanent teeth.8 It is not uncommon that resorption of unknown aetiology is encountered.9
Idiopathic external root resorption is the term used when the condition exists without a known aetiology.10 Mueller and Rony first reported the condition in 1930.11 It is a rare condition that has been reported in single and multiple teeth. Two types have been observed: apical and cervical.12,13 The majority of reports involve the apical part of several teeth in young individuals. In apical idiopathic root resorption, the resorption starts apically and progresses coronally causing a gradual shortening and rounding of the roots, whereas the cervical type starts in the cervical region and approaches the pulp.14,15 Various classification systems of root resorption have been proposed.3,16,17,18,19,20 These systems have used different terms and categories to describe dental root resorption. There is considerable confusion and disagreement in the literature regarding the manner of considering and thus classifying root resorption. Bakland described a simple classification system (Table 1) based on site, type and aetiology.16
Site
Type
Aetiology
Internal
TraumaInfection
External
SurfaceInflammatory
TraumaTraumaInfection
Replacement (Ankylosis)
Avulsion and re-implantationLuxationTransplantation
Aetiology of different types of root resorption requires two phases: mechanical or chemical injury to the protective tissues and stimulation by infection or pressure.21,22 Injury can be similar in various types of root resorption. The selection of proper treatment is related to the stimulation factors. Intrapulpal inflammation due to pulp disease as a consequence of the injury is the stimulation factor in internal root resorption and external periradicular inflammatory root resorption.23 Adequate root canal treatment controls intrapulpal bacteria and arrests the resorption process.23 In cervical root resorption, infection originates from the periodontal sulcus and stimulates the pathological process.17,24 As adequate infection control in the sulcus is unlikely, removal of granulation tissue from the resorption lacuna and sealing are necessary for repair.17 Removal of the stimulation factor, ie pressure, is the treatment of choice in root resorption related to pressure during orthodontic treatment, or an impacted tooth or tumour.17 In ankylotic root resorption, there is no known stimulation factor; thus, no predictable treatment can be suggested.17 Therefore, various types of root resorptions can be classified according to the stimulation factors:
Pulpal infection resorption;
Periodontal infection resorption;
Orthodontic, impacted tooth or tumour pressure resorption; and
The process of root resorption involves a complex interaction of inflammatory cells, resorbing cells, hard tissue, cytokines and enzymes such as collagenase, matrix metalloproteinase and cysteine proteinase.20 The periodontal ligament is a specialized connective tissue that acts as a barrier between the alveolar bone and cementum.25 Localized damage or loss of periodontal ligament renders the denuded cementum surface chemotactic to osteoclasts.20,21 This can result in root resorption. In cases where multiple teeth are involved, Löe and Waerhaug have suggested that the dental tissues become part of the osseous system and thus subject to remodelling.26
Multiple idiopathic apical root resorption is a specific entity that must be differentiated from all other resorptive processes. Kerr described the phenomenon of multiple teeth affected with resorption with no known aetiological pathogenesis, such as trauma, previous history of orthodontic treatment or any systemic condition identified.27 Only 14 clearly identified cases of multiple idiopathic apical root resorption have been reported in the literature (Table 2), all of which were in relatively young individuals aged from 14 to 39 years, and the majority of the affected individuals in these studies were males. This paper describes an adult female with multiple idiopathic apical root resorption of maxillary incisor teeth, as well as congenitally missing maxillary canines, and discusses restorative options and subsequent management.
A 35-year–old female suffering with root resorption of maxillary anterior teeth was referred to the Department of Restorative Dentistry at Birmingham Dental Hospital by her general dental practitioner. The patient had no family history of such anomaly. There was no previous history of orthodontic treatment, dental extraction, trauma to teeth or any specific infection in relation to her maxillary anterior teeth. The patient also reported discoloration of her upper left central incisor tooth and general drifting of her maxillary incisor teeth.
The physical appearance of the patient was normal, with a skeletal Class I dental base relationship, and no notable asymmetry of face was noted. Clinical examination revealed missing maxillary canines and a discoloured maxillary left central incisor (UR1). The maxillary lateral incisor teeth were atypical in shape and were diminutive. Generalized spacing and drifting of anterior incisors was noted. The maxillary incisor teeth were not tender to percussion. These teeth were not mobile, with normal probing depths. The teeth also showed positive but delayed response to sensitivity testing with ethyl chloride (Dr Georg Friedrich Henning Chemische Fabrik Walldorf GmbH, Walldorf, Germany) and Electronic Pulp Tester (Analytic Endodontics, Redmond, WA, USA).
Radiographic examination revealed substantial apical root resorption on UR2, UR1, UL1 and UL2. These teeth had short and malformed root morphologies. The UL2 and the adjacent UL4 were significantly rotated (Figure 1a, b).
Figure 1.
(a) OPG demonstrating missing maxillary canines and apical root resorption affecting UR2, UR1, UL1 and UL2. (b) Periapical radiographs pretreatment showing extensive root resorption of maxillary incisors.
Following an initial assessment, it was clear that the patient's aesthetic concerns mainly involved the maxillary arch and, as the mandibular dentition was largely unaffected, the treatment options considered were:
Orthodontic alignment of maxillary incisors +/- aesthetic restoration of teeth;
Elective root canal treatment of maxillary incisors +/- aesthetic restoration of teeth;
Combination of above;
Construction of maxillary partial overdenture using strategic use of the patient's electively root-treated natural incisors as abutments;
Extraction of maxillary incisor teeth and provision of a partial denture or implant-retained fixed or removable restorations.
Following discussions with the patient, and in light of the patient's age and expectations, it was decided that any treatment that involved a removable option would not be acceptable. Elective root canal treatment of already compromised teeth, and using them as abutments for prosthesis retention or restoring them with conventional crowns, would be an aggressive option with unpredictable life span. Orthodontic alignment of the affected teeth was also ruled out because of the compromised nature of the teeth, the unpredictable outcome and its unacceptability to the patient. The initial definitive treatment plan was:
The construction of a maxillary immediate partial denture following the loss of maxillary incisor teeth with extractions;
Replacement of the maxillary incisors and canines with dental implants with early placement protocol with partial bone (12–16 weeks) healing and subsequent fixed restorations.
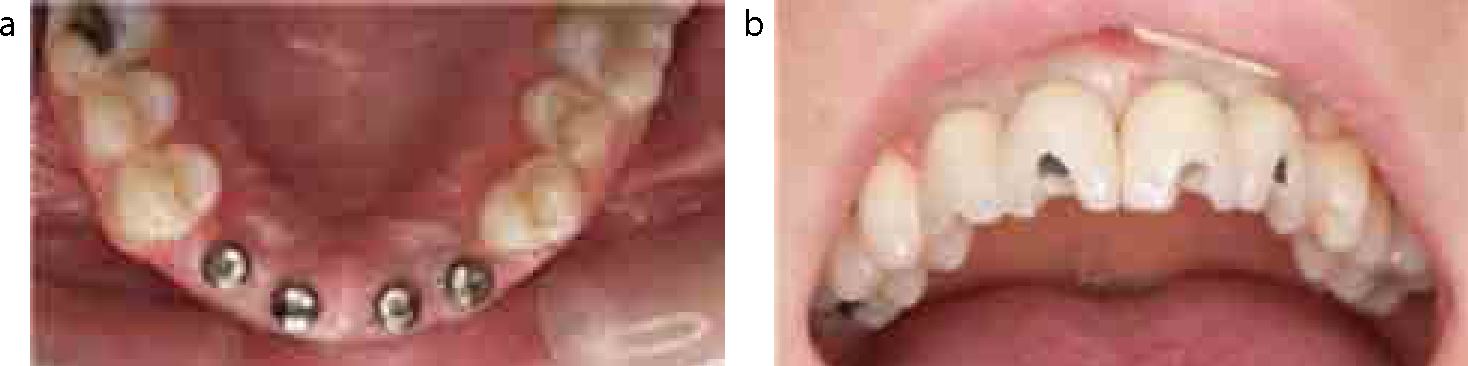
The anterior maxillary teeth were extracted under local anaesthetic and an immediate partial prosthesis inserted (Figure 2a, b). The teeth on the denture had ovate-shaped pontics to retain ridge shape. The patient was then reviewed regularly and the denture relined to compensate for the alveolar bone changes within the initial phase of socket healing (modelling). The hygienic design of the immediate partial denture and pontic shape maintained a scalloped profile of the alveolar tissue at the missing space (Figure 3).
Figure 2.
(a, b) Maxillary immediate partial denture in situ following extractions of incisor teeth.Figure 3. Clinical view of scalloped alveolar ridge profile to maintain interdental papilla height.
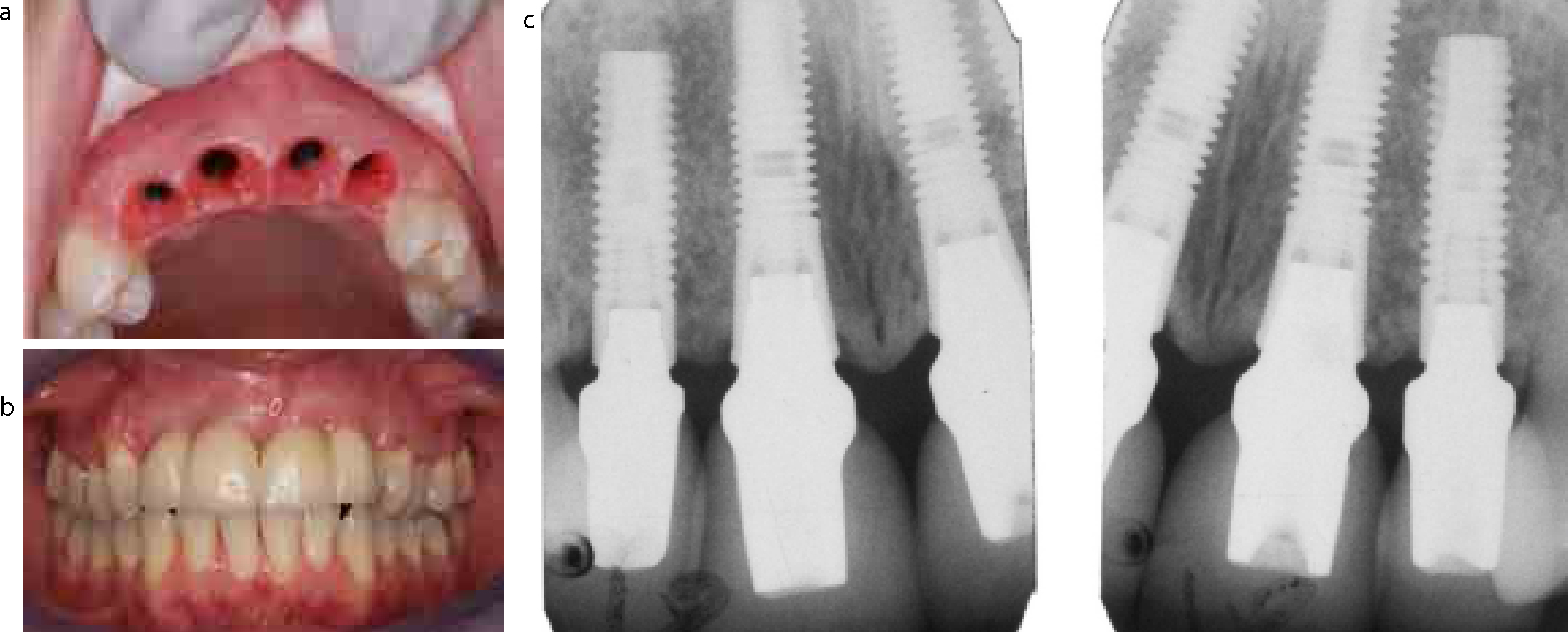
Approximately 12 weeks after the maxillary anterior teeth were extracted, four dental implants (Astra tech – 3.5 mm diameter, 15 mm length at lateral incisors and 4.0 mm diameter, 15 mm length at central incisors) were inserted under local anaesthetic and intravenous midazolam sedation (Figure 4). Twelve weeks following implant placement, the dental implants were uncovered, fixture level impressions were obtained using an open tray technique, the cast verified and four individual composite provisional crowns fitted (Figure 5a, b). Three weeks following insertion of provisionals, when good tissue conditioning was observed clinically, the restorations were replaced with all-ceramic crowns on zirconia abutment cores (Figure 6a, b). The patient was subsequently followed for three years and good bone levels were noted around the dental implants (Figure 6c).
Figure 4. OPG demonstrating four 15 mm dental implants.Figure 5.
(a) Clinical view of tissue healing following implant placement. (b) Provisional composite crowns in situ.Figure 6.
(a) Clinical view of excellent soft tissue conditioning with temporaries. (b) Definitive crowns in situ. (c) Intra-oral radiographs showing definitive crowns fit and bone levels after three-year follow-up.
Discussion
External root resorption that develops in the absence of a plausible cause is termed idiopathic. By definition, idiopathic external root resorption is a diagnosis of exclusion.38 From the number of reported cases in the dental literature, multiple idiopathic external cervical root resorption (MIECRR) appears to be more common than multiple idiopathic external apical root resorption (MIEARR).38 MIEARR affects a wide age range of patients, from 14 years to 39 years old and, in contrast to MIECRR, males appear to be more frequently affected by MIEARR than females, with a male:female ratio of 11:4.36 In addition, MIEARR appears to have a predilection for premolar and molar regions.38
Other common features of the MIEARR cases appear to be:36
Normal clinical appearance of teeth and periodontal tissues;
Root resorption associated with vital teeth and endodontically treated teeth;
Lack of periodontal and periradicular inflammation;
Alveolar bone levels within normal limits;
Absence of local aetiological factors;
Patients asymptomatic until very late in the pathological process where increased tooth mobility reported;
Commonly found as an incidental finding on radiographs;
Intramaxillary and intermaxillary symmetrical pattern of root resorption.
In this case, the patient was a 35-year-old female who was not aware of the resorptive process affecting her maxillary incisor teeth and no signs or symptoms of endodontic pathology were present. The radiograph also showed bone levels within normal limits and sensitivity tests showed a positive response to the teeth affected. The teeth were not mobile and pathology was found as an incidental finding on radiographs by the patient's general dental practitioner.
In an attempt to explain the cause of idiopathic external root resorption, Pinska and Jarzynka first suggested genetic susceptibility in their report of a family with generalized root resorption.39 Newman then followed this with a study of 37 families and a tentative genetic association was found.40 In the case presented, no family history of root resorption was found but missing isolated permanent canines were noted at clinical examination, which was confirmed radiographically. The patient was not aware of missing canines and did not give a history of previous extractions. Congenital absence of missing teeth excluding third molars is called hypodontia. The reported prevalence of hypodontia in the literature affecting the permanent dentition often varies, even within similar populations, with ranges as wide as 0.3–36.5%.41 The data from the literature confirms that hypodontia is more prevalent in females than in males in a ratio of 3:2. The reported sites and frequency of missing teeth is also varied among studies.41 The most common missing teeth in descending order are mandibular second premolar (3.0%), maxillary lateral incisor (1.7%), maxillary second premolar (1.5%) and mandibular central incisor (0.3%).41 Hypodontia affecting exclusively the maxillary permanent canines is extremely rare and there are only a few cases of absence reported in the literature.42,43 Several theories concerning the aetiology of hypodontia have been proposed, including suggestions that both genetic and environmental factors may play a role. Mutations in the genes Msx1 and Pax9 are associated with an isolated form of hypodontia.44 MIEARR in a hypodontia patient has not been reported in the literature.
With no absolute aetiological factors identified, treatment of MIEARR depends largely on the presenting symptoms and the extent and the severity of root resorption. The usual treatment is the extraction of teeth of poor prognosis and long-term monitoring of the remaining dentition using serial radiographs, periodontal assessment, sensitivity tests or patient symptoms.36 This was the option chosen in this case. Edentulous saddles may be restored using adhesive or conventional fixed bridges, removable partial dentures or osseointegrated implants. Abutment teeth must be carefully assessed for root resorption. The success of long-term osseointegration in sites where root resorption has been active is unknown.45 In severe cases where all permanent teeth are affected, the only option available may be extraction of all teeth and construction of a complete denture or an implant-retained fixed or removable restoration.
An option of endodontic treatment of the affected teeth has been well documented for inflammatory root resorption, where calcium hydroxide is the current intraradicular medicament of choice.46 However, a common finding in MIEARR is that teeth remain vital even after extensive root resorption, and Rivera and Walton stated that MIEARR does not seem to be mediated by or have its source from the dental pulp. Therefore, root canal treatment is not indicated.15 In this case too, the affected teeth showed a positive response to sensitivity testing and, in light of evidence of extreme root resorption radiographically on the affected teeth, root canal treatment of the affected teeth was not considered.
The use of implants to restore a patient suffering with MIEARR has not been described in the literature previously. Although an implant option was considered in the treatment, the authors were concerned that implant placement might result in lack of osseointegration and complications. However, in the present case, based upon radiological examination, the maxillary incisors were likely to have a guarded long-term prognosis.
Conclusion
Multiple idiopathic external apical root resorption is a rare dental pathology affecting the roots of teeth. The aetiology and pathogenesis of this condition is not known. Isolated bilateral agenesis of maxillary canines is also extremely rare. A combination of the above dental manifestations could affect successful dental rehabilitation and restorative treatment of such patients. This paper highlights that patients with MIEARR can be treated with dental implants if treatment is timed correctly. The use of 3-dimensional planning may facilitate optimum and precise implant placement, which in turn allows the implants to be placed in areas with appropriate bone quality and volume. The technique may also allow early loading protocols to be utilized.