Pjetursson BE, Brägger U, Lang NP, Zwahlen M. Comparison of survival and complication rates of tooth-supported fixed dental prostheses (FDPs) and implant-supported FDPs and single crowns (SCs). Clin Oral Implants Res. 2007; 18:97-113
Tan K, Pjetursson B, Lang N, Chan E. A systematic review of the survival and complication rates of fixed partial dentures (FPDs) after an observation period of at least 5 years. III. Conventional FPDs. Clin Oral Implants Res. 2004; 15:654-666
Creugers NHJ, Käyser AF, Hof MAv. A meta-analysis of durability data on conventional fixed bridges. Community Dent Oral Epidemiol. 1994; 22:448-452
Holm C, Tidehaq P, Tillberg A Longevity and quality of FPDs: a retrospective study of restorations 30, 20, and 10 years after insertion. Int J Prosthodont. 2003; 16:283-289
Goodacre CJ, Bernal G, Rungcharassaeng K, Kan JYK. Clinical complications in fixed prosthodontics. J Prosthet Dent. 2003; 90:31-41
Reuter JE, Brose MO. Failures in full crown retained dental bridges. Br Dent J. 1984; 157:61-63
Foster LV. The relationship between failure and design in conventional bridgework from general dental practice. J Oral Rehabil. 1991; 18:491-495
Briggs P, Ray-Chaudhuri A, Shah K. Avoiding and managing the failure of conventional crowns and bridges. Dent Update. 2012; 29:78-84
Planciunas L, Puriene A, Mackeviciene G. Surgical lengthening of the clinical tooth crown. Stomatologija. 2006; 8:88-95
Rosenstiel SF, Land MF, Fujimoto J. Mouth preparation, 5th edn. Oxford: Mosby; 2015
Lanning S, Waldrop T, Gunsolley J, Maynard J. Surgical crown lengthening: evaluation of the biological width. J Periodontol. 2003; 74:468-474
Deas DE, Moritz AJ, McDonnell HT, Powell CA, Mealey BL. Osseous surgery for crown lengthening: a 6-month clinical study. J Periodontol. 2004; 75:1288-1294
Rosenstiel SF, Land MF, Fujimoto J. Retainers for partial removable dental prostheses, 5th edn. Oxford: Mosby; 2015
Pihlaja J, Näpänkangas R, Kuoppala R, Raustia A. Veneered zirconia crowns as abutment teeth for partial removable dental prostheses: a clinical 4-year retrospective study. J Prosthet Dent. 2015; 114:633-636
Kancyper S, Sierraalta M, Razzoog ME. All-ceramic surveyed crowns for removable partial denture abutments. J Prosthet Dent. 2000; 84:400-402
Case Study: Management of Failing Maxillary Bridgework David Gray Dental Update 2024 47:2, 707-709.
Authors
DavidGray
Associate Dentist, The Broadway Dental Practice, Catford, London, SE6 4SN and Specialty Doctor in Prosthodontics, Eastman Dental Hospital, 47-49 Huntley Street, London WC1E 6DG, UK
The current trend, and often gold standard, for replacement of missing teeth is implant-retained fixed or removable prostheses. These, however, are not always suitable, whether due to financial constraints, or the patient wishing to avoid the associated surgical treatment. Utilizing crowns as retainers for partial removable dental prostheses in such cases can provide a favourable aesthetic and functional outcome, whilst avoiding many of the retentive pitfalls that patients fear are associated with a removable appliance.
CPD/Clinical Relevance: A systematic approach is required when approaching failing bridgework in order to overcome the unique challenge involving unpredictable abutment status, which often cannot be appraised until the bridgework is dismantled.
Article
David Gray
Whilst appropriately prescribed and maintained bridgework is likely to provide good clinical service, it will ultimately fail. Survival rates for conventional fixed dental prostheses (FDPs) vary in the literature, with an estimated 5- and 10-year survival of 93.8% and 89.2%, respectively,1 and 15-year survival reported at 68−74%.2,3 Complication rates over a 5-year observational period are 15.7%,1 with the most frequent complications being biological, such as caries and loss of pulp vitality.1,4 An earlier study supported these findings, with the two most commonly reported complications as caries (18% of abutments) and need for endodontic treatment (11% of abutments).5
This particular case highlights an additional risk factor − an increased number of units and, more significantly, abutment teeth, within the bridge. A bridge of greater than four units is considered to be at increased risk of failure, and use of three or more abutments reduces survival by almost half.6,7 Despite this, additional abutment teeth are often incorporated into bridge design where one or more abutments are considered suboptimal. This, however, is a false economy, as bridge survival is dictated by the most compromised tooth. Many such bridges will fail as a result of partial de-cementation and decay − whilst it is often difficult to know whether abutment de-cementation preceded the caries or not, it has been suggested that this loss of the marginal seal is a common cause of catastrophic caries beneath bridges.8
The replacement of failing bridgework, especially where a large span is involved, is a challenge for both the practitioner and patient. The patient may often have had the bridge(s) for a number of years and will have become well accustomed to the fixed appliance. As such, when it comes to a point that the bridgework is failing, particularly as a result of caries or infection (thereby compromising the status and longevity of the underlying abutment tooth), he/she will often be faced with the reality that simply replacing the bridgework ‘like for like’ is neither feasible nor suitable. A transitionary period wearing a removable appliance is often required, and definitive options may not be to the patient’s liking.
This case is of a patient whose bridgework had been in service for around 20 years. With an implant-supported fixed prosthesis not financially viable, the only suitable definitive replacement option was a removable partial denture (RPD).
Whilst patients may favour a fixed prosthesis, a well-executed treatment plan involving removable prostheses can deliver excellent results. Replacement of the bridgework can be seen as an opportunity to execute a treatment plan that may be otherwise seen as unnecessary or superfluous to needs. For example, routinely preparing teeth for milled crowns during denture provision may be considered overtreating. However, where abutment teeth have been prepared previously, these preparations can be restored with conventional crowns or, preferably, the opportunity used to provide milled crowns that will serve as retainers for the partial denture.
Case report
A 37-year-old male with an extensively restored upper arch presented complaining of several problematic abutment teeth that he had been recently advised would require treatment.
The fixed prosthesis in situ had been placed after an assault whilst a teenager. He had since become an irregular dental attender. Several months previously, an infection prompted a dental visit, whereupon two teeth were removed (UL6 and LR7). At this stage he was informed of the poor prognosis of several other teeth. The treatment proposed, involving several implants, was cost prohibitive, and he attended the author's practice on recommendation to seek an alternative plan.
His medical history revealed that he was fit and well, taking no regular medications and having no allergies.
Extra-oral examination revealed no abnormalities, with a Class I skeletal relationship and a medium smile line. Basic Periodontal Examination (BPE) was:
2
2
2
1
2
1
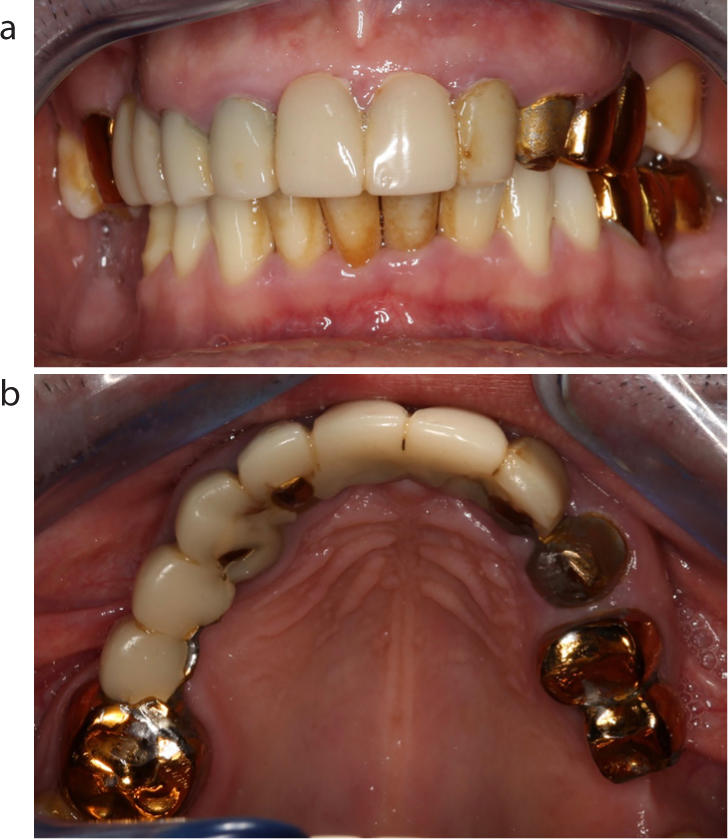
On intra-oral examination (Figure 1) the patient had a nine-unit upper conventional FDP, spanning UR6 to UL3, with a separate two-unit distal cantilever FDP off the UL4 (the distal abutment, UL6, having been recently removed). Two abutment teeth, the UL2 and UL3, were found to be grossly carious and unrestorable and the remaining bridgework was cosmetically unacceptable. Radiographic examination, consisting of periapical radiographs and an orthopantomogram (Figure 2), highlighted the extent of decay in UL23, whilst showing the remaining teeth to be free of decay and apical pathology. Other relevant findings included generalized gingivitis, although no periodontal pocketing. The remaining dentition was healthy and caries free.
Figure 1.
(a, b) Pre-treatment presentation.Figure 2. Orthopantomogram showing extensive bridgework, and carious abutment teeth UL23
Two viable treatment options existed − that by which an attempt to salvage some of the bridgework was made (namely the four units spanning UR6 to UR3), and another whereby all bridgework was removed, followed by rehabilitation. The latter was opted for insofar that it would create the most homogeneous end result cosmetically and would allow the most predictable long-term outcome.
Prognosis
The patient was well motivated to treatment, and willing to undertake the measures to secure a successful outcome. Nonetheless, it was emphasized that the demise of his previous bridgework was significantly impacted by inadequate oral hygiene and a poor diet. Failure to address these factors through implementation of optimal diet and oral hygiene was likely to risk failure of the work being provided.
It was also important that treatment was planned to optimize the patient’s capacity to maintain his dentition − long span bridgework and plaque-retentive restorations were avoided to achieve this.
Final treatment plan
Stabilization phase
Oral hygiene instruction, diet analysis
Removal of bridgework
Placement of temporary crowns on restorable abutment teeth (UR6, UR3, UR2, UL4)
Extraction of unrestorable teeth (UL2 and UL3)
Placement of immediate denture to replace missing upper teeth
Restorative phase
Restore teeth UR6, UR3, UR2, UL4 with milled crowns
Placement of definitive cobalt chrome denture to replace missing upper teeth
Crown lengthening of the UR2 and UR3 was incorporated into the treatment plan after appraisal of teeth
The treatment
Prior to undertaking treatment, the patient was advised on his sugar intake, and sub-optimal oral hygiene. He was informed that he should make efforts to reduce both the amount and frequency of sugar consumption. The importance of optimal plaque control was emphasized; the patient was given advice on effective toothbrushing technique and interdental cleaning.
The first phase of treatment involved removal of the bridgework and temporary restoration of the retained and missing teeth. In a single visit, the upper FDPs were sectioned and removed, and those unrestorable abutment teeth extracted. The remaining abutment teeth were restored with chairside-made temporary crowns constructed from a pre-operative putty impression (Figure 3) and an immediate acrylic denture was fitted. The retainers on the UR6 and UL4 were maintained initially as temporaries.
Figure 3. After extraction of the unrestorable abutment teeth, and placement of temporary crowns.
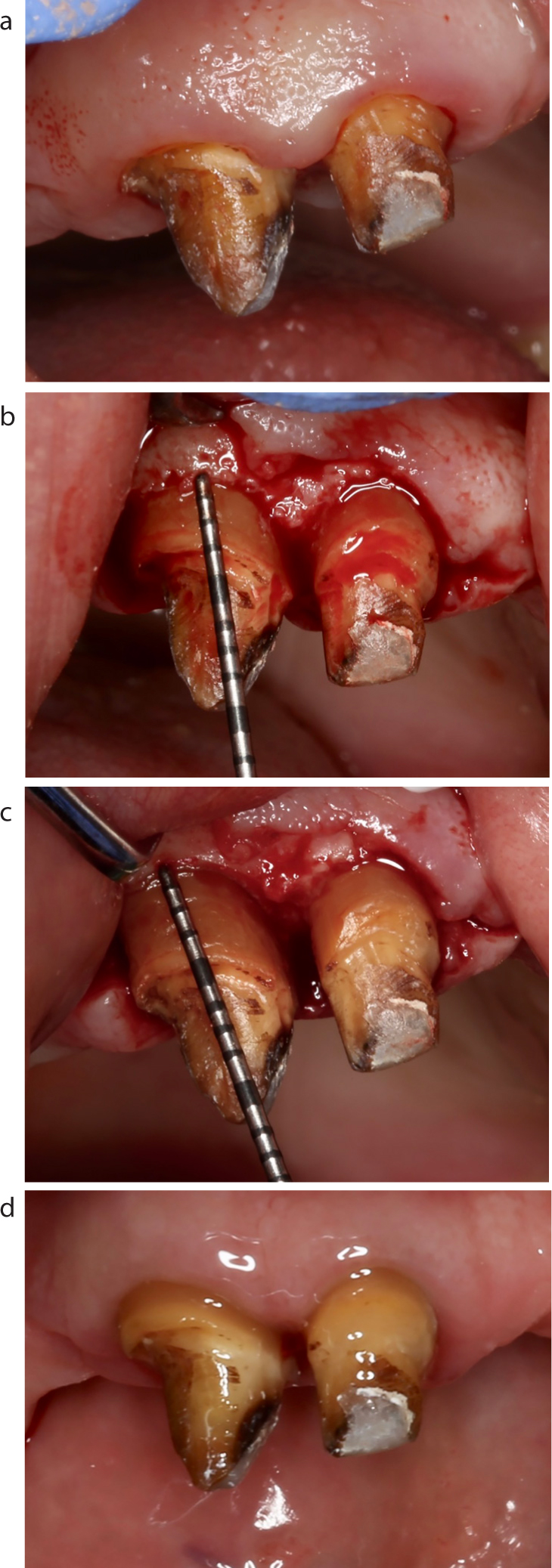
At this stage, the UR2 and UR3 were found to have been previously heavily prepared, with very tapered preparations and large cores. After discussion of the various options with the patient, it was decided that these two teeth would benefit from crown lengthening surgery (Figure 4).
Figure 4. Crown lengthening surgery: (a) pre-operative, (b) prior to bone removal, (c) after bone removal, (d) six-weeks post-operatively.
Nine weeks later (to allow for healing and gingival remodelling), the patient returned for the restorative phase of treatment. Diagnostic casts were taken, and these mounted in the retruded axis position on a semi-adjustable articulator for treatment planning.
On the following visit, the four teeth to be restored with crowns had their existing preparations refined, and definitive impressions taken (see discussion for preparation considerations with milled crowns). Of note, the author feels, in hindsight, that this was too short a period. As a rule, with any crown lengthening procedure, final crown restorations should be delayed until 4–6 weeks after the surgical procedure.9,10 However, clinical studies have demonstrated that biological width and position of the free gingival margin exhibit some change between 3–6 months post-surgery.11,12 As such, in the aesthetic zone, it may have been advisable to restore the teeth provisionally, delaying fabrication of definitive restorations for a period of 12 weeks or more.10
The working cast was cross-mounted with a diagnostic cast, and four crowns constructed (Figure 5).
Figure 5. Extra-coronal restorations prior to cementation.
The final phase of treatment was denture construction, completed over four visits. At the first visit, the temporary crowns were removed, and the definitive crowns inserted. A working impression was taken in a spaced special tray using a polyether. From this final working cast, the framework could be constructed. At the second denture visit, the framework was tried in alongside the milled crowns. A bite registration (wax block on an acrylic base) was taken at this stage, with the crowns in situ, to confirm the articulation of the casts, and mark smile line, canine lines and centre lines. The third denture visit was tooth try-in on the framework. Tooth arrangement, both with respect to positioning and occlusion, and aesthetics, were considered excellent by the patient and clinician, and the denture was returned to process to fit.
The final appointment was for denture fit. The temporary crowns were removed, and the teeth cleaned with pumice slurry and rinsed. After cleaning the fitting surfaces of the crowns with air abrasion, the crowns were cemented using a dual-core self-adhesive resin cement (Figure 6). After the cement had hardened, the denture was fitted (Figures 7 and 8). Retention was excellent, albeit initially rather difficult to fit and remove. After several insertions and removal, and identifying the exact path of insertion and removal, this became significantly easier.
Figure 6. Extra-coronal restorations after cementation.Figure 7. Extra-coronal restorations and denture in situ.Figure 8. Anterior smile view.
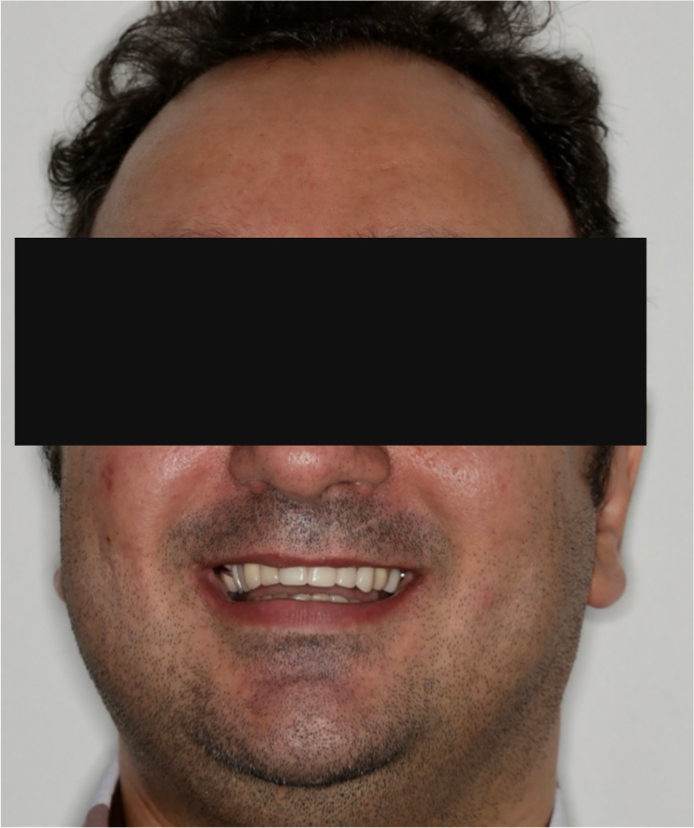
A review three weeks later found that the patient had adapted well to the denture (Figure 9). He commented that taste, comfort and the overall wearing experience far exceeded the acrylic denture.
Figure 9. Full face smile view.
Further, the precision attachments made the denture feel especially secure. He noted that, for the first few days, insertion and removal was tricky, and best performed in front of a mirror, however, once this had been learnt, it posed no issues. There was no presence of rubbing or ulceration, and the denture required no adjustment.
Discussion
Replacement of missing teeth was agreed with the patient to be with a removable prosthesis. The need to provide four replacement crowns was also an opportunity to introduce design features that would improve the retention for the removable prosthesis.
‘The use of cast restorations on abutment teeth enables precise shaping of the axial contours of such restorations, which in turn allows the masticatory and retentive forces to be directed more favourably through appropriate use of occlusal rest seats and precisely shaped guide planes.’13 Furthermore, cast retainers can also enable the incorporation of precision attachments, which can offer significant aesthetic advantages over clasp-retainer RPDs.
Gathering information
Careful, comprehensive diagnostic evaluation and a well-designed treatment plan is essential to the successful provision of these crowns. This requires additional diagnostic procedures, including:
Accurate diagnostic casts mounted in centric relation;
The use of a dental surveyor:
To help evaluate tissue undercuts and their influence on RPD design;
To help evaluate the relative alignment of the long axis of teeth that support the partial RPD;
To help determine the optimal path of displacement and removal of the RPD (and, by inference, its effect on the geometry of crown preparation).
Crown design
Once the teeth have been appraised, the crowns and denture may be designed. There are several modifications that may be incorporated into the cast restoration to accommodate a partial RPD:
Occlusal rest seats;
Minor connectors;
Clasp retention;
Reciprocation.
Occlusal rest seats
This is a prepared recess in the restoration to receive the occlusal, incisal, cingulum, or lingual rest. The occlusal rest of the partial RPD should fit precisely into the corresponding rest seat. To reduce laterally directed forces, the rest seats should be spoon-shaped, and the junction between the internal aspect of the rest seat and the proximal guide plane should be rounded to minimize stress on the RPD framework and thereby reduce the chance of an RPD fracture at the interface between the occlusal rest and the minor connector.
Minor connectors
These are the connecting link between the major connector and other parts of the RPD, such as the clasp assembly, indirect retainers and rests. They should fit intimately against the proximal guide plane on the cast restoration. Within the principles of RPD design, guide planes should be as tall as possible occlusocervically and should follow the normal configuration of the tooth buccolingually. All proximal and reciprocal guide planes should parallel each other.
Clasp retention
Clasps engage a portion of the tooth surface, either entering an undercut for retention, or remaining above the height of contour to act as a reciprocating element. The cast restoration can be designed with a survey line (as related to the path of insertion) placed as is most useful.
This will include factors such as ensuring that when a clasp is in its normal position with the partial RPD fully seated, it should fit passively against the retainer, whilst remaining at least 2 mm away from the gingivae to avoid impacting on periodontal health. This means that the survey line should not be placed too far cervically. Likewise, the height of contour must not be placed too far occlusally, otherwise binding of the retentive arm may occur during insertion of the RPD. Ideally, this height should be within the middle third of the retentive surface of the retainer. A properly contoured surface enables the retentive arm to flex gradually along the path of insertion.
Reciprocation
This is the means by which lateral forces generated by a retentive clasp passing over a height of contour are counterbalanced. This is usually done by a reciprocal clasp or plate that engages the reciprocal guiding plane.
Guide planes are needed on the crowns to allow for successful reciprocation. These should extend from the proximal guide plane to an area directly opposite the terminal position of the retentive clasp. Reciprocal clasps must contact the guide plane before the retentive arms start to flex, so that the periodontium is protected against excessive loading.
Tooth preparation
The practitioner will need to plan the preparation of each individual crown on the basis of its design. Once the path of insertion for the RPD has been determined, those teeth that require abutment crowns can be prepared, taking into account the following:
Path of placement;
Rest seats;
Axial contours.
Path of placement
Favourable tooth alignment in relation to the planned path of placement of the partial RPD is essential. Thus, whilst conventional crowns typically have a path in the long axis of the tooth, RPD retainers may not. Those surfaces on which both guide planes and reciprocal planes are planned, as well as areas that require survey lines in the gingival third, typically require additional reduction. Of note, these modifications should not lessen the retention form excessively because, during prosthesis removal, the retainers are often subjected to forces parallel to their path of placement.
Rest seats
Sufficient tooth structure must be removed to allow for the minimally required metal thickness of 1.0 mm in the area of an occlusal rest seat. There are two methods of achieving adequate reduction:
Prepare a rest seat in the tooth prior to starting the crown preparation. Then a 1.0 mm reduction groove is used to ensure adequate reduction. Or, preferably;
The less conservative method of a wider zone of reduction in the area of the rest seat, as having the flexibility to move the rest seat during the laboratory phase is very useful.
Axial contours
When a crown is to serve as an RPD abutment, modifications may be required in the normal axial reduction. The extent of these additional reductions depends upon the RPD design. For example, where the retainer must be under-contoured with regard to the original tooth form to accommodate proximal or reciprocal guide planes and to allow the non-retentive part of an occlusally approaching clasp to be positioned as far gingivally as possible.
Material selection
Conventionally, incorporation of retentive features would make the material of choice metal-ceramic, whilst omitting such features would broaden material selection by including allceramics such as lithium disilicate.
At present, whilst all-ceramic crowns have a relatively wide literature base for their conventional use, the literature is less voluminous when it comes to their use as abutment crowns, particularly when their construction will involve features such as guide planes or rest seats. The mechanical properties of zirconia suggest that it might serve well as a material for abutment crowns for partial RPDs.
One study retrospectively looked at veneered zirconia single crowns as abutment teeth for a clasp-retained RPD with a metal framework.14 The complications found were fracture of the veneering porcelain (11%) and fracture of the occlusal rest seat (3%). Wear of porcelain at the occlusal contact point was found in 24% of the zirconia single crowns. Wear of the ceramic surfaces of the rest seats for the RPDs was not found. The retention was good in all RPDs. The stability was good in 73% and moderate in 23% of the RPDs. Thus, the complication rates mimic conventional (non-abutment) veneered zirconia crowns − veneer fracture is yet to be a problem that is readily overcome.
Another study described the fabrication of all-ceramic crowns for RPDs with rest seats and guide planes in densely sintered aluminium oxide and retentive areas in veneering porcelain.15 Results, albeit limited by study size, were favourable.
In this case, given the previous preparations to the teeth, it is likely that minimal alteration to the tooth would be required. The previous bridgework had porcelain both buccally and palatally, and thus a heavy preparation had been completed. This means that the significantly more conservative nature of a metal-ceramic crown preparation (palatally a metal-ceramic crown would require only around 0.5−0.8 mm reduction (metal only), compared with 1.5 mm for an e.max) is largely negated. However, leaving metal only palatally does confer the advantage of reducing wear of the opposing teeth.
On balance, it was felt that metal-ceramic crowns offered greater predictability, and the significant advantage of keeping occlusal surfaces in metal only, thereby reducing opposing arch wear.
Conclusion
This case highlighted the means by which utilization of milled crowns, coupled with a well designed and constructed cobalt chrome partial denture, can give patients an outcome that is far from their preconceived notion of removable prosthodontics − the denture can in fact be incredibly retentive, especially in function.
One prerequisite to successful outcomes in combined fixed-removable cases such as this one is careful planning. The success of each stage is reliant on the prior step, in particular in ensuring that the laboratory can construct the fixed-removable prosthodontics required; for example, poorly planned crowns will likely result in under preparation and technical difficulties in constructing the required milled surfaces. Subsequently, poorly constructed milled crowns will risk creating guide planes and surfaces that are not conducive to insertion of a denture.
However, when planned correctly, these cases are thoroughly rewarding for the patient and practitioner.