Eccles JD. Tooth surface loss from abrasion, attrition and erosion. Dent Update. 1982; 9:373-381
Gow AM, Kelleher MG. Tooth surface loss: unusual interproximal and lingual cervical lesions as a result of bizarre dental flossing. Dent Update. 2003; 30:331-336
Mumghamba EGS, Honkala S, Honkala E, Manji KP. Gingival recession, oral hygiene and associated factors among Tanzanian women. E Afr Med J. 2010; 86:125-132
Wu CD, Darout IA, Skaug N. Chewing sticks: timeless natural toothbrushes for oral cleansing. J Periodont Res. 2001; 36:275-284
Darwish S. The management of the Muslim dental patient. Br Dent J. 2005; 199:503-504
Axelsson P, Lindhe J. Effect of controlled oral hygiene procedures on caries and periodontal disease in adults. J Clin Periodont. 1978; 5:133-151
Al-Khateeb TL Periodontal treatment needs among Saudi Arabian adults and their relationship to the use of the Miswak. Comm Dent Hlth. 1991; 8:323-328
Ndungu FL, Kaimenyi JT, Arneberg P, Muthami LN. A comparative study of the efficacy of plaque control by a chewing stick and a tooth brush. E Afr Med J. 1990; 67:907-911
Farooqi MIH, Srivastava JG. The toothbrush tree (Salvadora persica). Quart J Crude Drug Res. 1968; 8:1297-1299
Bader A, Flamini G, Cioni PL, Morelli I. The composition of the root oil of Salvadora persica L. J Essent Oil Res. 2002; 14:(2)128-129
Francis G, Kerem Z, Makkar HPS The biological action of saponins in animal systems: a review. Br J Nutr. 2002; 88:(6)587-605
Tannins and human health: a review. Crit Rev Food Sci Nutr. 1998; 38:421-464
Sofrata A, Claesson L, Lingstrom P A strong antibacterial effect of Miswak against oral microorganisms associated with periodontitis and caries. J Periodont. 2008; 79:(8)1474-1479
Almas K. The antimicrobial effects of seven different types of Asian chewing sticks. Odontostomatol Trop. 2001; 24:(96)17-20
Almas K, Al-Zeid Z. The immediate antimicrobial effect of a toothbrush and miswak on cariogenic bacteria: a clinical study. J Contemp Dent Pract. 2004; 5:(1)
Al Bayati K, Sulaiman K. In vitro antimicrobial activity of Salvadora persica L. extracts against some isolated pathogens in Iraq. Turk J Biol. 2008; 32:57-62
Darout IA, Skaug N, Albandar JM. Subgingival microbiota levels and their associations with periodontal status at the sampled sites in an adult Sudanese population using miswak or toothbrush regularly. Acta Odont Scand. 2003; 61:115-122
Norton M, Addy M. Chewing sticks versus toothbrushes in West Africa. A pilot study. Clin Prev Dent. 1989; 11:(3)
Eid MA, Selim HA. A retrospective study on the relationship between miswak chewing stick and periodontal health. Egypt Dent J. 1994; 40
Samad Younes SA, Angbawi MF. Gingival recession in the mandibular central incisor region of Saudi schoolchildren aged 10–15 years. Comm Dent Oral Epidemiol. 1983; 11:246-249
Eid MA, Selim HA, Al-Shammery AR. The relationship between chewing sticks (Miswak) and periodontal health. 3. Relationship to gingival recession.Berlin, Germany1985
Lee W, Eakle W. Possible role of tensile stress in the etiology of cervical erosive lesions of teeth. J Prosthet Dent. 1984; 52:374-380
Bartlett D, Shah P. A critical review of non-carious cervical (wear) lesions and the role of abfraction, erosion and abrasion. J Dent Res. 2006; 85:306-312
Kitchin P. The prevalence of tooth root exposure and the relation of the extent of such exposure to the degree of abrasion in different age classes. J Dent Res. 1941; 20:565-581
Ibiyemi O, Oluwatosin Oketade I, Taiwo J, Oke G. Oral habits and tooth wear lesions among rural adult males in Nigeria. Arch Orofac Sci. 2010; 5:(2)31-35
Butterworth C, Ellakwa E, Shortall A. Fibre-reinforced composites in restorative dentistry. Dent Update. 2003; 30:300-306
Malquarti G, Berruet RG, Bois D. Prosthetic use of carbon fibre-reinforced epoxy resin for aesthetic crowns and fixed partial dentures. J Prosthet Dent. 1990; 63:251-257
Smith DC. Recent developments and prospects on dental polymer. J Prosthet Dent. 1962; 12
Vallittu PK. Comparison of the in vitro fatigue resistance of an acylic resin removable partial denture reinforced with continuous glass fibres or metal wires. J Prosthodont. 1996; 5:115-121
Culy G, Tyas M. Direct resin-bonded, fibre-reinforced anterior bridges: a clinical report. Aust Dent J. 1998; 43:1-4
Kelleher MG, Bomfim DI, Austin RS. Biologically based restorative management of tooth wear. Int J Dent. 2012; https://doi.org/101155/2012742509
Tooth surface loss can present in a variety of ways, some of which can appear rather strange on first examination. This case report demonstrates an unusual presentation of tooth surface loss (TSL) and its subsequent treatment. This loss of hard dental tissue appeared to be affecting the whole of the patient's remaining dentition, both lingually and buccally. Detailed questioning revealed the origins of this problem which turned out to be due to excessive use of an intra-oral Miswak chewing stick.
Clinical Relevance: This article will enable clinicians to understand the importance of specific, targeted history-taking, involving a rare case of tooth surface loss as well as the use of minimally destructive restoration composites and a fibre-reinforced composite bridge.
Article
Tooth surface loss, affecting both the lingual and buccal aspects of teeth presenting as a generalized pattern, is a relatively rarely reported pathological finding. More commonly, tooth surface loss occurs mainly on the palatal aspects of teeth (eg in cases of bulimia or gastro-oesophageal reflux disease (commonly abbreviated to GORD), or on the incisal or occlusal surfaces of teeth, or a combination of both depending on the various aetiologic factors.
There are a number of different descriptions and indices of tooth surface loss, some implying a supposedly definite aetiology. In 1982, Eccles described ‘tooth surface loss’ as a pathological loss of hard tooth tissue by a disease process other than dental caries.1
The aetiological factors responsible for tooth surface loss are usually described as belonging in one of the following main categories:
Erosion;
Attrition;
Abrasion;
‘Abfraction’. This is a very controversial term and considerable doubt exists within the dental profession about the term itself or its supposed pathogenesis.
Tooth surface loss can be a progressive phenomenon, but it can also present as a reflection of past habits and/or of only slowly progressive tooth surface loss.
The primary focus prior to treatment planning should be on establishing the probable aetiology in the first place to increase the likelihood of an effective preventive strategy for that particular aetiologic factor, thereby increasing the chances of a long-term successful outcome for that particular patient and diminishing the chances of inappropriate interventions for that individual patient.
Case report
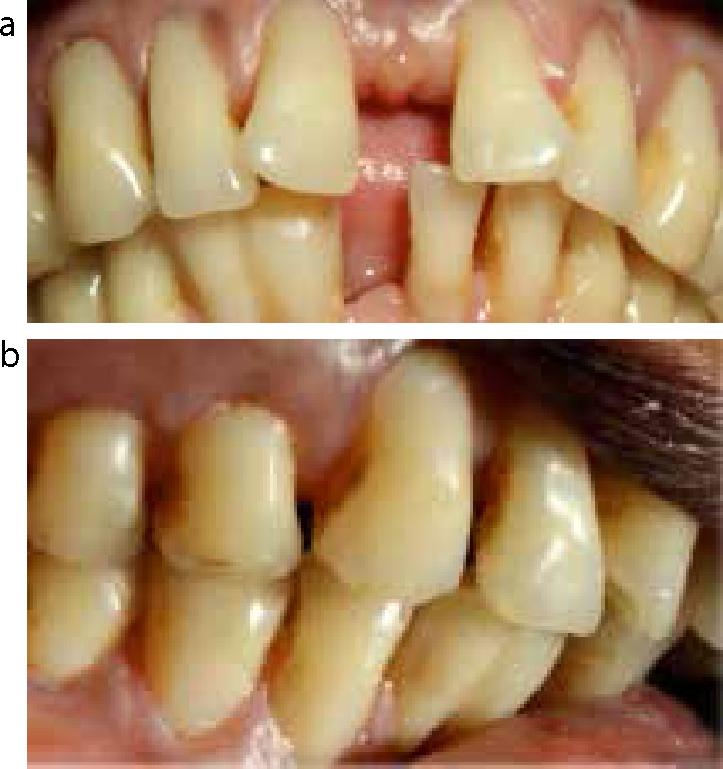
This case report describes an unusual cause of severe generalized pathological tooth surface loss. This 52-year-old lady presented to the Restorative Clinic at King's College Dental Institute, London, for assessment about replacing a lower central incisor which she had lost due to a traumatic injury. On clinical examination a generalized pattern of cervical tooth surface loss was observed affecting both the buccal and lingual surfaces of her adult dentition, accompanied by generalized gingival recession (Figure 1 a–d).
Figure 1. (a) Labial view of right side demonstrating cervical tooth surface loss and gingival recession (b) Lingual view of lower incisor teeth, demonstrating cervical tooth surface loss. (c, d) Lateral view exhibiting the severity of cervical tooth surface loss, all the way through significant parts of the dentine.
This case report demonstrates that, although detailed history-taking about dietary and regurgitation issues still remain important in trying to ascertain the possible causes of tooth surface loss, habits, including the use of unusual tools to maintain oral hygiene, or bizarre methods of use of more conventional ones, such as flossing, are also sensible lines of enquiry.2
The cervical portions of the enamel had been lost completely on many teeth and much, or all, of the way through dentine. In some areas, this exposed where the pulp had been.
Medically, the patient was fit and healthy and was not taking any medication. She specifically denied ever having had any gastric regurgitation type problems and was not a vegetarian. As a result, this pattern of tooth surface loss did not appear to be attributable to any medical cause. She had no clinically detectable caries and signs of significant active periodontal disease were absent. A basic periodontal examination revealed a score of 2 in every sextant, although there was significant recession obvious both labially and lingually.
Positive results were gained from sensibility (‘vitality’) testing of her remaining dentition with cold and electric pulp testing. Further detailed questioning about her diet revealed no present or previous abnormal intake of any erosive fluids or unusual dietary habits.
The patient was a clerical worker by occupation and enquiry about unusual habits did not reveal anything untoward. Further detailed and sensitive questioning of the patient about her oral hygiene habits uncovered the probable aetiological factor behind this unusual presentation. It appeared that this patient had been using an African chewing stick, known as ‘Miswak’, to clean her teeth instead of using a conventional toothbrush.
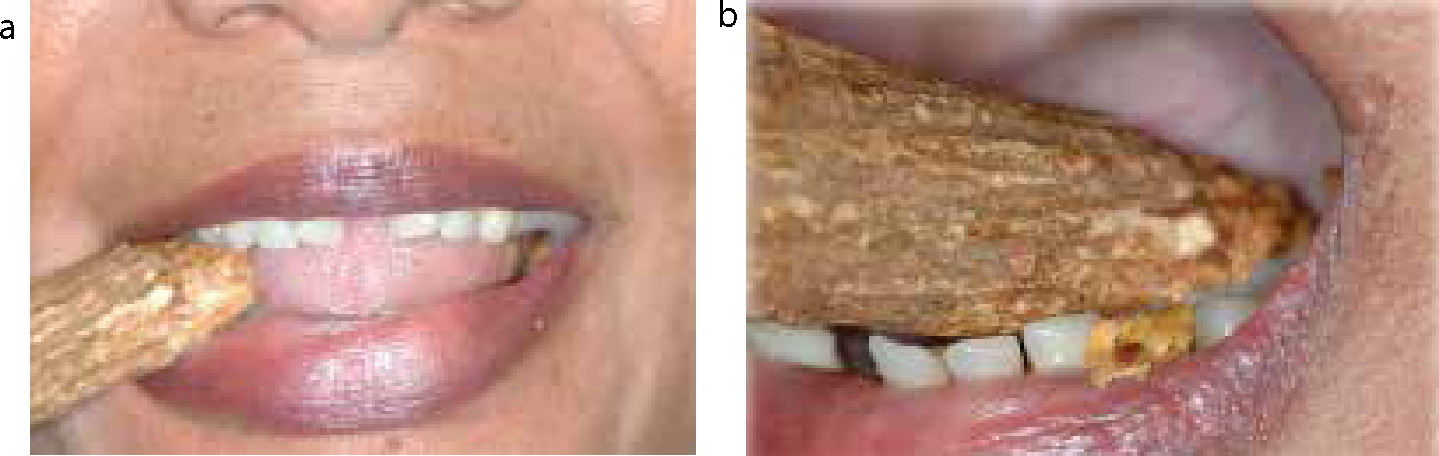
An internet search and demonstration of its use (Figure 2) brought to light the details of the Miswak stick's abrasive nature.3
Figure 2.
(a) Patient demonstrating chewing of Miswak, prior to its use. (b) Patient demonstrating use of a Miswak stick lingually.
Origin of the chewing stick
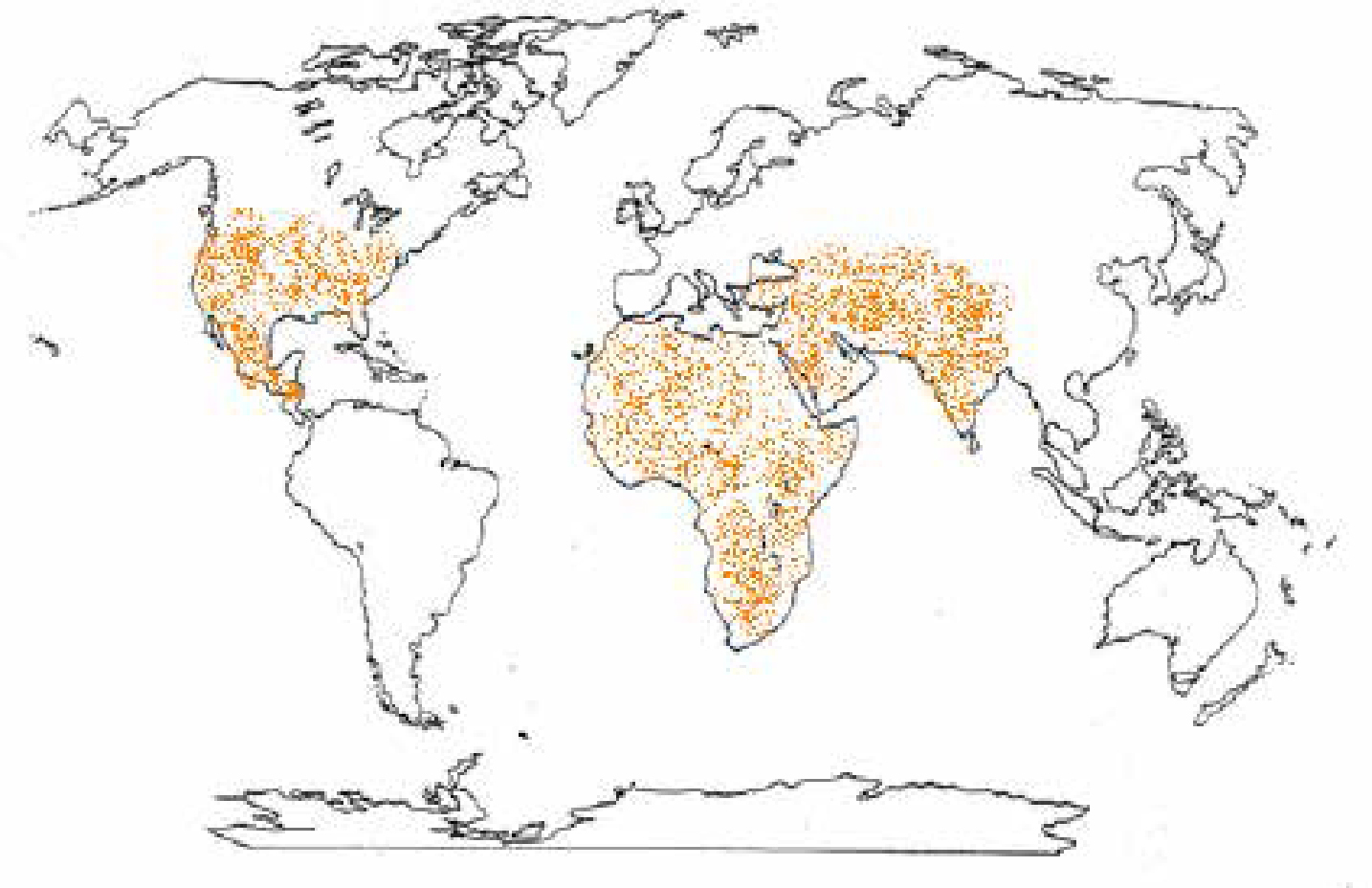
Chewing sticks are used internationally, but especially in parts of the world such as Africa, India and the Middle East (Figure 3). They have been known to have been used by the Babylonians approximately 7000 years ago. They appear to have been utilized by ancient Greeks, Romans and Egyptians. Many versions of such a stick exist and the wood used to make these ‘Miswaks’ comes from a variety of trees that are found all over the world (Table 1).4
Figure 3. Main distribution of Miswak use around the world.
Botanical Name
Local Name
Main Area of Use
Salvadora persica
Arak
Middle East
Citrus aurantafolia
Lime Tree
West Africa
Citrus sinenis
Orange Tree
West Africa
Cassia sleberlanba
Roots of Senna
Sierra Leone
Azadirachta Indica
Neem
India
Betula lenta
Cherry Birch/Black Birch
North America
Gaultheria procumbens
American Wintergreen
North America
The roots, twigs and stems of these evergreen trees are all used as oral hygiene tools. These trees are largely upright, have aromatic roots and usually do not exceed a height of 3 metres. The sticks are harvested, bundled together and sold in local markets as toothbrushes or tongue-cleaning aids.4
The low cost, ready availability, as well as it being favoured for different cultural and religious reasons,5 make this a popular oral hygiene tool, particularly in developing countries. The use was endorsed by the World Health Organization in 1986 and 2000 in international consensus reports.
Method of use of the stick
The stick measures approximately 15–20 cm and can have a diameter of up to 1.5 cm. Typically, the stick is chewed at one end (Figure 2a) until the bark becomes soft and frays. Once frayed, patients use the stick in a scrubbing motion, on every surface of the tooth, including buccal and lingual surfaces as shown (Figure 2b). The fibres of the Miswak are orientated in the same direction as the long axis of the stick and therefore allow easier access to the buccal surfaces of the teeth, when used in a horizontal motion, and to the lingual surfaces, when used in a vertical direction, as is most commonly practised. This is in contrast to a conventional toothbrush where the bristles are orientated perpendicular to the handle. This means that access interdentally is somewhat more restricted with the Miswak stick and may explain the staining found on the interproximal surfaces of this patient's dentition.
At times, patients may moisten the stick to speed up the effect and thereafter, rather than replace the whole stick, the frayed end is cut before it is re-used. Toothpaste is usually not available and not used with this toothbrushing stick and apparently was not used by this patient.
Properties of the Miswak stick
The benefits for the use of the Miswak in relation to oral hygiene are primarily owing to its chemomechanical properties.4 The frayed end serves to remove the build-up of plaque mechanically, whilst, the ‘sap’ of the stick contains many agents that have been found to have antimicrobial effects. Evidence for the use of Miswak, however, is controversial.
Mechanical effect on plaque
This is certainly an important factor as it has been shown that the mechanical cleaning of plaque can be a highly effective preventive measure for the control of gingivitis and caries progression.6
In fact, it has been found that the periodontal treatment need amongst a Saudi Arabian population using Miswak sticks is lower than non-users.7
Other studies, however, have found that the effect of the Miswak and the use of a toothbrush are similar in the mechanical removal of plaque,8 or that the former is less effective. For example, in a study comparing the use of a toothbrush and Miswak chewing sticks, it was concluded that, for patients with severe plaque deposits, the toothbrush is more effective than the chewing stick in plaque control. However, for those patients with moderate plaque deposits, the chewing stick was as efficacious as the toothbrush in plaque control. One can argue that, in this particular study, the sample size was too low to make valid inferences.9
Antimicrobial effects
Apart from the mechanical effects that the Miswak stick may have on the removal of plaque, many naturally occurring chemicals have been isolated from this chewing stick that have been found to have some beneficial effects (Table 2). These include: saponins along with tannins, silica, a small amount of resin, trimethylamine and a fairly large amount of alkaloidal constituents. In addition to this, benzyl-isothiocyanate has been isolated from the roots of the tree.10
This is supported by gas chromatography mass spectrometry analyses of the root oil, which revealed that it consists mainly of Benzyl-isothiocyanate (70%) which is known to have antibacterial activity.11
Many studies have further investigated the effect of the chemicals found in Miswak on oral health. One study14 suggests that the Miswak stick has inhibitory effects on common pathogenic bacteria, such as Aggregatibacter actinomycetemcomitans and Porphyromonas gingivalis, but less so on cariogenic bacteria, such as Lactobacillus acidophilus or Streptococcus mutans. This is corroborated by a study comparing the effect of seven different types of chewing sticks, where it was found that there was an antimicrobial effect on Enterococcus faecalis at 50% concentration of Kikar (Acacia arabia) from Pakistan and Arak (Salvadora persica) from Saudi Arabia, but had little effect on Streptococcus mutans, Staphylococcus aureus and Candida albicans.15 In contrast, Almas and Al-Zeid16 investigated the immediate antimicrobial effects of S. persica Miswak and its extract on Streptococcus mutans and Lactobacillus, and found a significant decrease in Streptococcus mutans count, but not in Lactobacillus count, in Miswak users. Other studies also support the antimicrobial effect on Enterococcus faecalis where it was found that it was the most sensitive micro-organism to be affected by the use of S. persica Miswak.15,17
Having looked at the mechanical and antimicrobial effect of Miswak, the actual efficacy of its use has been challenged in a number of studies, however, and current evidence suggests that it is either no better than conventional oral health aids or the results are inconclusive.4 For example, it has been found that Miswak users harboured significantly higher plaque levels of Staphylococcus intermedius, A. actinomycetemcomitans, Veillonellaparvula, Actinomyces israelii and Capnocytophaga gingivalis, as well as significantly lower levels of Selenomonas sputigena, Streptococcus salivarius, Streptococcus oralis and Actinomyces naeslundii, than did toothbrush users.18 This is supported by a pilot study19 which reports more plaque formation and gingival bleeding in people using chewing sticks than toothbrush users. This is despite finding a decrease in the rate of caries progression in such users.
In addition, a retrospective study conducted in Saudi Arabia showed Miswak users had deeper periodontal pockets and a higher prevalence of periodontal diseases than did non-users.20
Although conflicting results have been found suggesting the efficacious use of the Miswak, there seems to be a positive relationship between its use and gingival recession,21,22 which may explain the clinical appearance observed in the patient in this study.
Discussion
Despite the conflicting evidence base, this patient presented with no evidence of caries and did not suffer from noticeable active periodontal disease, although the significant recession was noted, which might well be expected after reviewing many of the above studies.21,22 At first, however, one might be forgiven for guessing that this presentation resembles that associated with the controversial theory of ‘abfraction.’ However, further enquiry revealed that, in fact, this was not true.
Abfraction lesions have been reported to present primarily at the cervical region of the dentition and are typically wedge-shaped, with sharp internal and external line angles. This appearance is supposed to be caused by excessive occlusal stress and masticatory forces.23,24 However, so far there has been little in the way of scientific literature to prove that this phenomenon actually exists, especially as these supposedly excessive occlusal forces should affect both the buccal and lingual aspects of the dentition equally.25 In particular, it has been reported that these lesions are found more prominently in the maxilla rather than the mandible and preferentially on premolars, canines and incisors.25 This is unlikely to be the cause of this particular clinical presentation reported by these authors, where there has been no obvious evidence of parafunction or grinding.
Detailed, culturally sensitive, enquiry into patient habits is considered to be a very important part of the history-taking process in trying to determine the cause of the tooth surface loss, but one may quickly overlook such rare, but salient facts, in order to attribute the tooth surface loss to a particular ‘preferred’ cause, such as abfraction, which was the speculative diagnosis offered by the referring general dental practitioner.
A reasonable question about the existence of ‘abfraction’ as a discrete pathologic entity could be: ‘If excessive occlusal forces really did produce this sort of cervical tooth surface loss how come one does not see this cervical tooth surface loss also in every wear case involving mainly attrition, considering that massive forces are involved in the tooth-to-tooth grinding producing that incisal and occlusal wear?’
Patients will not always be obliging in revealing details of their (oral hygiene) habits unless they are specifically asked. Many may not realize the relationship between their cleaning approaches and their clinical dental presentation. Taking adequate time to build rapport and allow sensitive questioning into patient oral hygiene procedures cannot only reveal the frequency in which patients brush but the manner in which they do so and the tools that they choose for this. Once the correct information has been gleaned from the patient, this approach enables the clinician to discuss with the patient the adoption of more appropriate preventive measures which should be of greater benefit to that individual patient.
Links between toothwear and other oral cleaning habits have, indeed, been found and26 may have contributed to the pattern of gingival recession shown in this case.21,22
Treatment
Initial treatment for this patient consisted of toothbrushing instruction with a medium toothbrush and a modified Bass technique. This would ensure that any future treatment would not be jeopardized by continual brushing using the chewing stick. Furthermore, as can be seen from Figure 1, this habit had hastened the process of gingival recession. The patient was advised that, although this process could not be reversed, it could be controlled.
The size and extent of the lesions meant that the remaining tooth structure needed to be protected. Treatment consisted of adding direct resin composite to the affected areas of the remaining dentition in order to prevent further weakening of her teeth and help avoid possible pulpal irritation (Figure 4). This form of treatment is biologically acceptable and preserves as much of the remaining structure as possible.
Figure 4.
(a) Labial and (b) lateral views demonstrating composite resin addition to remaining tooth structure.
In addition, this could facilitate the impression-taking stage, when fabricating replacement prosthesis for her lower central incisor, which was this patient's initial presenting complaint.
The options for replacing the lower central incisor that were considered with the patient were:
A removable partial denture;
A fixed resin-bonded bridge;
A fixed conventional bridge;
A fibre-reinforced bridge; or
A single tooth implant.
The patient was not keen on a surgical option and therefore declined implant therapy. However, she was keen to explore both removable and other fixed options. A removable partial denture would have permitted the replacement of soft tissue and hard tissue and, though removable, would be likely to offer this patient a good aesthetic advantage. In addition, as the long-term prognosis of the adjacent incisors was guarded, it was felt that, in due course, these could be added to the prosthesis. The idea of a resin-bonded bridge was explained to the patient and, being fixed, appeared advantageous to the patient, however, this approach would not provide soft tissue replacement. Metal shine through might also have been a significant issue in this case. An alternative to these, involving a fibre-reinforced composite bridge, was then considered because there would be less aesthetic compromise as the metal-retaining pad would not show through.27
Fibre-reinforced composite bridges are, by definition, resin-based restorations containing fibres aimed at enhancing their physical properties, largely by reduction in crack propagation.28 Their use in fixed prosthetic dentistry was first described in 1990,29 although its applications in dentistry first originate back to the 1960s.30 Fibre reinforcement, allegedly permits stresses to be redistributed more effectively throughout the restoration, conferring increased fatigue resistance to composite when compared to simple metal wire reinforcement.31
The fibres can be made from glass, ultra high molecular weight polyethylene, or Kevlar fibres and can vary in arrangement from uni-directional to multi-directional. The resin used fixes the fibres in place and provides further reinforcement to the restoration.28 In this case, ‘EverStick’ fibres were used (Sticktech Ltd, Turku, Finland) where the multi-directional fibres are pre-impregnated with light-curable monomers (PMMA) permitting cross-linking to occur with the overlying composite resin material used, thereby forming an effective network.
The adjacent teeth were isolated with rubber dam, before applying acid etch and a three bottle bonding system (Allbond 2, Bisco Inc, USA). The fibres were then fixed in place using flowable composite and a mesial cantilever design was used to provide replacement for this patient's missing lower central incisor (Figure 5).
Only short-term clinical data are currently available to compare these fibre-reinforced resin composites to the metal-based alternatives and the optimal design characteristics still remain to be established.27 In addition, the evidence base for the survival rates of fibre-reinforced composite bridges is considerably less than that available for metal retainer sub-frames. However, the technique provides an economic, direct, minimally destructive and aesthetic alternative to other conventional methods to replace anterior teeth in patients such as this. It can also be utilized when dealing with spaces within developing dentitions or for interim fixed prostheses, such as immediately after implant placement to avoid the use of a removable denture. The treatment can be completed in a single visit, does not require temporization, has low biologic cost and good operator control, in terms of shade, shape and repairs.27,32 Having said this, this method is reasonably demanding, especially when considering the shape of pontic and span size32 and can require more occlusal clearance for the retainers, although this was not a particular problem in this case.27
Conclusions
This report highlights the importance of sensitive and detailed history-taking as an aid to sound diagnosis and treatment planning. In this case, it revealed an unusual aetiological factor of what is now becoming a slightly more common clinical presentation in the UK and elsewhere owing to increased and changing patterns of immigration and travel. The importance of adequate preventive measures, particularly using a less destructive oral hygiene instruction, was required prior to starting active treatment. A minimally destructive treatment plan was put together in order to preserve what tooth structure remained, and such a pragmatic philosophical approach is well reported in the literature.33 Application of the above minimally destructive methods resulted in restoration of a functional, aesthetic and biologically acceptable outcome for this particular patient (Figure 6).