Malkinson S, Waldrop TC, Gunsolly JC, Lanning SK, Sabatini R The effect of esthetic crown lengthening on perceptions of a patient's attractiveness, friendliness, trustworthiness, intelligence, and self-confidence. J Periodontol. 2013; 84:(8)1126-1133
Tjan AH, Miller GD, The JG Some esthetic factors in a smile. J Prosthet Dent. 1984; 51:(1)24-28
Konikoff BM, Johnson DC, Schenkein HA, Kwatra N, Waldrop TC Clinical crown length of the maxillary anterior teeth preorthodontics and postorthodontics. J Periodontol. 2007; 78:(4)645-653
Gargiulo AW, Wentz FM, Orban B Dimensions and relations of the dentogingival junction in humans. J Periodontol. 1961; 362:261-267
Coslet JG, Vanarsdall R, Weisgold A Diagnosis and classification of delayed passive eruption of the dentogingival junction in the adult. Alpha Omegan. 1977; 70:(3)24-28
Bozzo L, de Almedia OP, Scully C, Aldred MJ Hereditary gingival fibromatosis. Report of an extensive four-generation pedigree. Oral Surg Oral Med Oral Pathol. 1994; 78:(4)452-454
Fletcher J Gingival abnormalities of genetic origin: a preliminary communication with special reference to hereditary gingival fibromatosis. J Dent Res. 1966; 45:597-612
Singer SL, Goldblatt J, Hallam LA, Winters JC Hereditary gingival fibromatosis with a recessive mode of inheritance. Case reports. Aust Dent J. 1993; 38:(6)427-432
Gorlin R, Cohen M, Levi L, 3rd edn. New York: Oxford Press; 1990
Coletta RD, Graner E Hereditary gingival fibromatosis: a systematic review. J Periodontol. 2006; 77:(5)753-764
Cuestas-Carnero R, Bornancini CA Hereditary generalized gingival fibromatosis associated with hypertrichosis: report of five cases in one family. J Oral Maxillofac Surg. 1988; 46:(5)415-420
Jones JE, Weddell JA, McKown CG Incidence and indications for surgical management of phenytoin-induced gingival overgrowth in a cerebral palsy population. J Oral Maxillofac Surg. 1988; 46:(5)385-390
Dahllof G, Preber H, Eliasson S, Ryden H, Karsten J, Modeer T Periodontal condition of epileptic adults treated long-term with phenytoin or carbamazepine. Epilepsia. 1993; 34:(5)960-964
Dongari A, McDonnell HT, Langlais RP Drug-induced gingival overgrowth. Oral Surg Oral Med Oral Pathol. 1993; 76:(4)543-548
Wise MD Stability of gingival crest after surgery and before anterior crown placement. J Prosthet Dent. 1985; 53:(1)20-23
Mavrogiannis M, Ellis JS, Seymour RA, Thomason JM The efficacy of three different surgical techniques in the management of drug-induced gingival overgrowth. J Clin Periodontol. 2006; 33:(9)677-682
McGuire MK, Scheyer ET Laser-assisted flapless crown lengthening: a case series. Int J Periodont Rest. 2011; 31:(4)357-364
Cunliffe J, Grey N Crown lengthening surgery – indications and techniques. Dent Update. 2008; 35:(1)29-25
This is the first article in a two-part series which aims to provide an overview of the different techniques used to increase clinical crown height. In the first paper, the focus will be on the management of patients who present with gingival tissue excess. The different aetiologies are discussed and illustrated with clinical cases, following which a range of procedures that may be employed in the management of these patients are presented. With an increasingly ageing population, more patients are taking regular medications prescribed from their general medical practitioner, and so having a working knowledge of the specific drugs that may cause gingival enlargement is essential.
Clinical Relevance: When patients with gingival tissue excess present in primary or secondary care, a clinician must have a good knowledge of the possible causes of the condition, as well as an idea of how the patient may be managed.
Article
This is a two-part series of articles that aims to provide an overview of the different techniques used to increase clinical crown height, a procedure known as crown lengthening. The need for increasing clinical crown height falls into two main groups: those that require increased crown length to improve aesthetics (commonly seen in patients with gingival tissue excess); and those that require increased clinical crown height to facilitate restorative treatment of a tooth or multiple teeth.
Smile aesthetics has been shown to play a vital role in the perception of an individual's attractiveness, friendliness and self-confidence.1 In patients where the gingival tissues have not retracted to their full extent during the eruption of teeth, this can have an impact where there is excessive gingival tissue on show. This condition is known as altered passive eruption and is more commonly referred to as a ‘gummy smile’. Similarly, the aesthetics may be affected in patients where normal tooth eruption has occurred but there has been gingival tissue overgrowth due to hereditary conditions, such as hereditary gingival fibromatosis, or secondary to certain types of medication. Gingival overgrowth can be mild, moderate or severe, where the full clinical crown is covered and the gingival tissues encroach upon the occlusal surfaces, making chewing and function difficult. In both groups, patients often become self-conscious of their appearance and often seek help to improve the appearance of their teeth. A key aspect of managing these patients is a thorough assessment of the complaint and their condition to ensure that the intervention offered will address their main concern.
Whilst the diagnosis of gingival overgrowth is straightforward, understanding the underlying cause is critical to ensure a successful outcome; failure to do this may result in adverse treatment outcomes which can compromise the patient's well-being.
Aetiology
Altered passive eruption
The reported prevalence of altered passive eruption varies between 10.6%2 to >65%,3 with the most common complaint being poor appearance due to ‘small’ teeth as a result of the gingival margin sitting in a coronal position on the crown.
During normal tooth eruption the processes of active and passive tooth eruption occur simultaneously. Active tooth eruption is the occlusal movement of a tooth as it emerges from its crypt in the gingiva, with this phase ending when the tooth makes contact with the opposing dentition. At the same time, apical migration of the dentogingival junction takes place, which is the passive eruption process, resulting in a normal clinical crown height whereby the gingival tissues have retracted to the cemento-enamel junction (CEJ).4
In some patients, however, the passive eruption process is disrupted and the gingival tissues do not retract to the CEJ, thus creating short clinical crowns. The exact reason for this remains unknown, however, the characteristics often seen in this group of patients include a high smile line, a thick gingival biotype and a square appearance of the clinical crown (Figure 1). In more severe cases, the excess gingival show can occur at rest, and is usually seen in combination with underlying skeletal factors, such as vertical maxillary excess, which usually leads to lip incompetence and an overall compromised appearance.
Figure 1. Classical appearance of a patient with altered passive eruption.
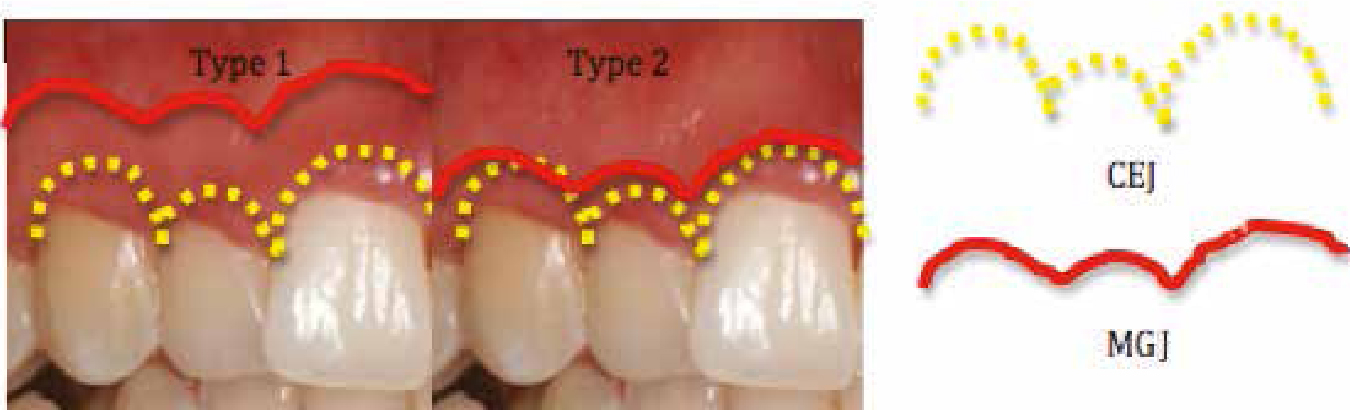
Altered passive eruption has been categorized into two main types, depending on the relationship of the gingivae with the crown and underlying alveolar bone:5
Type 1: Excess gingiva coronal to the CEJ with a wider band of keratinized tissue as measured from the free gingival margin to the mucogingival junction (Figure 2).
Type 2: Excess gingiva coronal to the CEJ, but there is a normal width of keratinized tissue as measured from the free gingival margin to the CEJ.
Both types can then be further subdivided into ‘A’ and ‘B’, depending upon the relationship of the alveolar crest to the CEJ. In subgroup A, the distance between the alveolar crest and CEJ is greater than 1 mm; in subgroup B, the alveolar crest is close to, or even at the same level as, the CEJ.
Gingival overgrowth: hereditary
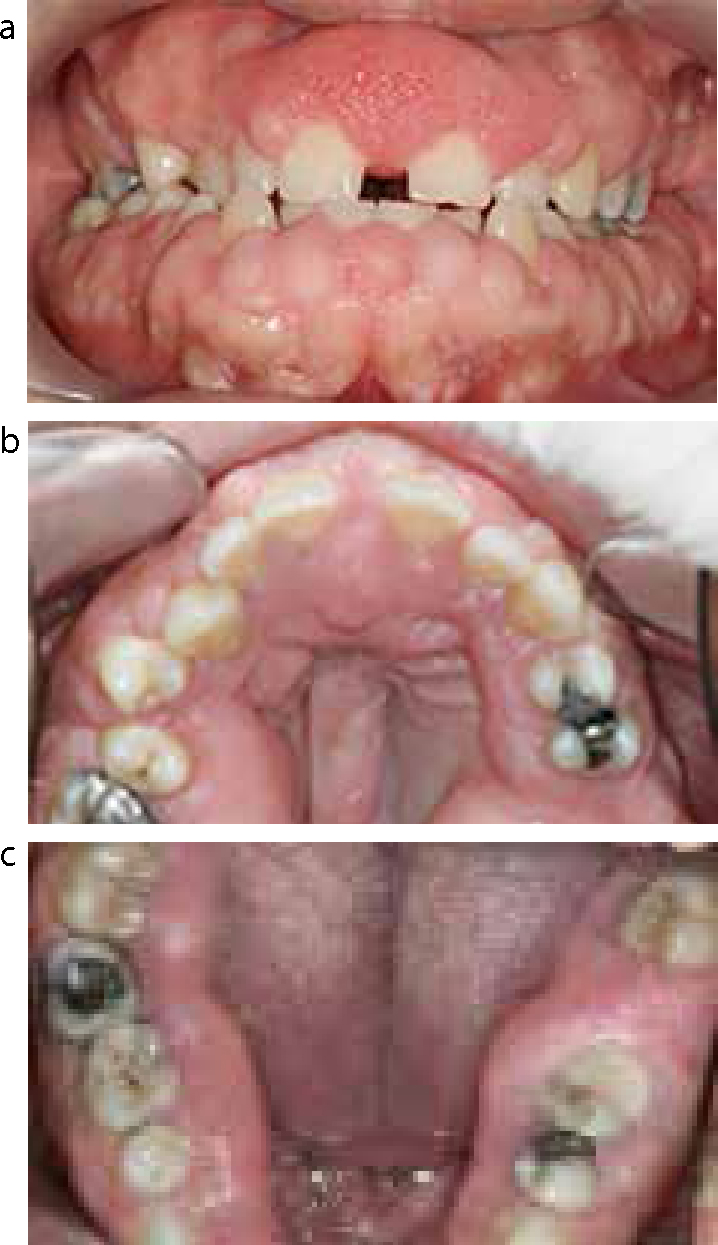
Hereditary gingival fibromatosis (HGF) is characterized by gingival enlargement of normal colour and firm consistency that is non-haemorrhagic and asymptomatic, but can affect function if excessive (Figure 3).6 It is reported to be a rare condition that affects males and females equally at a phenotype frequency of 1:175,000.7 It predominantly affects the permanent dentition and usually first occurs around the time of eruption of the permanent dentition.6,8
Figure 3. Classical appearance of a patient with hereditary gingival fibromatosis.
HGF is considered to be an autosomal dominant condition9 and, although it usually presents as an isolated disorder, in some individuals it can be associated with other alterations characterizing a syndrome.10 An example of an associated syndrome is ‘Gingival fibromatosis with hypertrichosis’, which is an autosomal dominant disorder characterized by excess growth of hair and mental retardation.10
The histological features of HGF have been found to be non-specific and so the definitive diagnosis is usually based upon family history and clinical findings.10
Within the literature there has been much debate regarding the most appropriate time to treat these patients in order to limit the risk of recurrence. Some have reported that intervention should be delayed until all permanent teeth have erupted, as the presence of teeth is required for the condition to occur.11 However, patients are usually unhappy with the appearance and often suffer from functional problems due to the enlarged tissue. It has therefore been recommended that treatment be undertaken when the patient can maintain his/her oral hygiene and is able to co-operate and consent to treatment to give maximum local and psychological benefits.10
The type of treatment provided will largely depend upon the severity and extent of the gingival enlargement. Whilst oral hygiene instruction and debridement are the first line of treatment, in cases of extensive enlargement, the overgrown tissue compromises plaque control, thus necessitating surgical intervention as part of the initial management. This usually involves a gingivectomy with a gingivoplasty where the excess gingival tissue is removed and recontoured, details of which are covered later. In the past management was much more aggressive with full mouth extractions often being advocated.11
Gingival overgrowth: drug-induced
Drug-induced gingival overgrowth is often seen in older patients. Three groups of drugs have been associated with gingival enlargement which include:12
Calcium channel blockers, such as nifedipine, which are used to manage hypertension by decreasing arterial smooth muscle contractility and subsequent vasoconstriction by inhibiting the influx of calcium ions through calcium channels; this leads to a vasodilatory effect resulting in an overall decrease in blood pressure. An association has been found between these drugs and gingival enlargement.13,14
Anticonvulsant medications, such as phenytoin, which used to be commonly prescribed for the management of epilepsy, and caused gingival hyperplasia in approximately 50% of patients.15,16 More recently, alternative medications have been introduced and so the prevalence of phenytoin-related gingival hyperplasia has reduced.
Immunosuppressant medications, such as cyclosporin, which is an immunosuppressant that is used to prevent rejection of transplanted organs, as well as managing various different autoimmune conditions; it has been frequently associated with gingival overgrowth within the medical and dental literature.17
Irrespective of the drug group, the presence of plaque is noted to be an exacerbating factor, with poor plaque control being a positive risk factor for the overgrowth. The management of these patients includes communication with the general medical practitioner to assess whether it is safe for the patient's medication to be altered, as well as a course of oral hygiene instruction and debridement.
Management
The management of gingival tissue excess is dependent on the aetiology, and the type of intervention undertaken will be determined by the patient's presenting complaint, clinical presentation and expectations. Thus a detailed clinical history and examination is the cornerstone of drawing up a definitive treatment plan.
History, examination and diagnosis
The focus of the history in these patients should be to ascertain their concerns and expectations to ensure the best treatment outcome. A detailed family and medical history that includes the patient's drug history, with the duration and dose, is fundamental, especially in those with drug-induced gingival overgrowth. A comprehensive history should be followed by a thorough clinical examination.
The extra-oral examination focuses on assessing the lip competence and the degree of gingival show, both at rest and on smiling. The intra-oral examination, in addition to the standard assessments, should incorporate an assessment of the texture and extent of the gingival tissue excess. The level of the patient's plaque control, as well as the presence of deposits, should be noted and, where appropriate, a six-point pocket chart should be undertaken, as well as special investigations including relevant radiographs and study casts. The latter will assist in the planning of the surgery and also the construction of post-operative stents that may be required to aid haemostasis following surgery.
Treatment
The treatment is usually undertaken in two phases:
Initial therapy aimed at optimizing plaque control and providing a course of non-surgical debridement to eliminate the marginal inflammation; and
Surgical removal of gingival tissue excess. In patients with drug-induced gingival overgrowth where the medication is the trigger, communication with the medical practitioner to alter the drug is often helpful in resolving the enlargement (Figure 4). However, this needs to be balanced against the medical needs of the patient.
Figure 4.
(a, b) A 68-year-old female presented to the department complaining of bleeding gums. She was hypertensive and was taking nifedipine to manage her hypertension. (a) The pre-operative appearance of her gingivae. (b) The appearance of her gingivae following a change in her medication by her GP, oral hygiene instruction and two courses of non-surgical debridement under local anaesthetic.
Surgical intervention is often required in these patients to optimize the appearance and to create an environment that facilitates maintenance of plaque control. In patients with altered passive eruption, the objective of the surgery remains the same, however, the endpoint is slightly different.
To this end, careful planning of the type of surgery is crucial and needs a clear understanding of the aetiology to avoid pitfalls.
The surgical planning will involve an assessment of the extent of tissue enlargement, the amount of keratinized tissue and local factors. This will enable a risk assessed plan to be drawn up and discussed with the patient.
There are three types of surgery that can be undertaken:
Gingivectomy with a gingivoplasty;
Apically repositioned flap surgery with no bone removal;
Apically repositioned flap surgery with bone removal.
Gingivoplasty
This is undertaken when there is a limited degree of gingival excess that needs recontouring to optimize the appearance. This intervention often provides an instantaneous result. This is also commonly undertaken in combination with gingivectomy procedures. This may be carried out using a scalpel or a large round diamond bur in an air turbine handpiece with water cooling.
Gingivectomy with a gingivoplasty
Gingivectomy refers to the surgical removal of the excess tissue. Pre-operative study casts and photographs can be a useful aid in planning and pre-operative periodontal probing will have provided the operator with adequate information to decide how much tissue removal can be afforded, depending upon the location of the CEJ in relation to the current gingival margin, the proposed gingival margin and the bony crest.
Once the gingivectomy procedure has been completed, pressure should be applied to the area with damp, sterile gauze to encourage haemostasis. Following this the authors recommend the placement of a periodontal dressing to aid with post-operative tissue stabilization, haemostasis and patient comfort.
Once the gross tissue has been removed, gingivoplasty can be undertaken to recontour the soft tissue to optimize the appearance. Gingivectomy and gingivoplasty may be carried out using a scalpel, angled blade holders, or a large round diamond bur in an air turbine handpiece with water cooling.
A case demonstrating the use of a gingivectomy and gingivoplasty in the management of HGF is presented in Figure 5.
Figure 5.
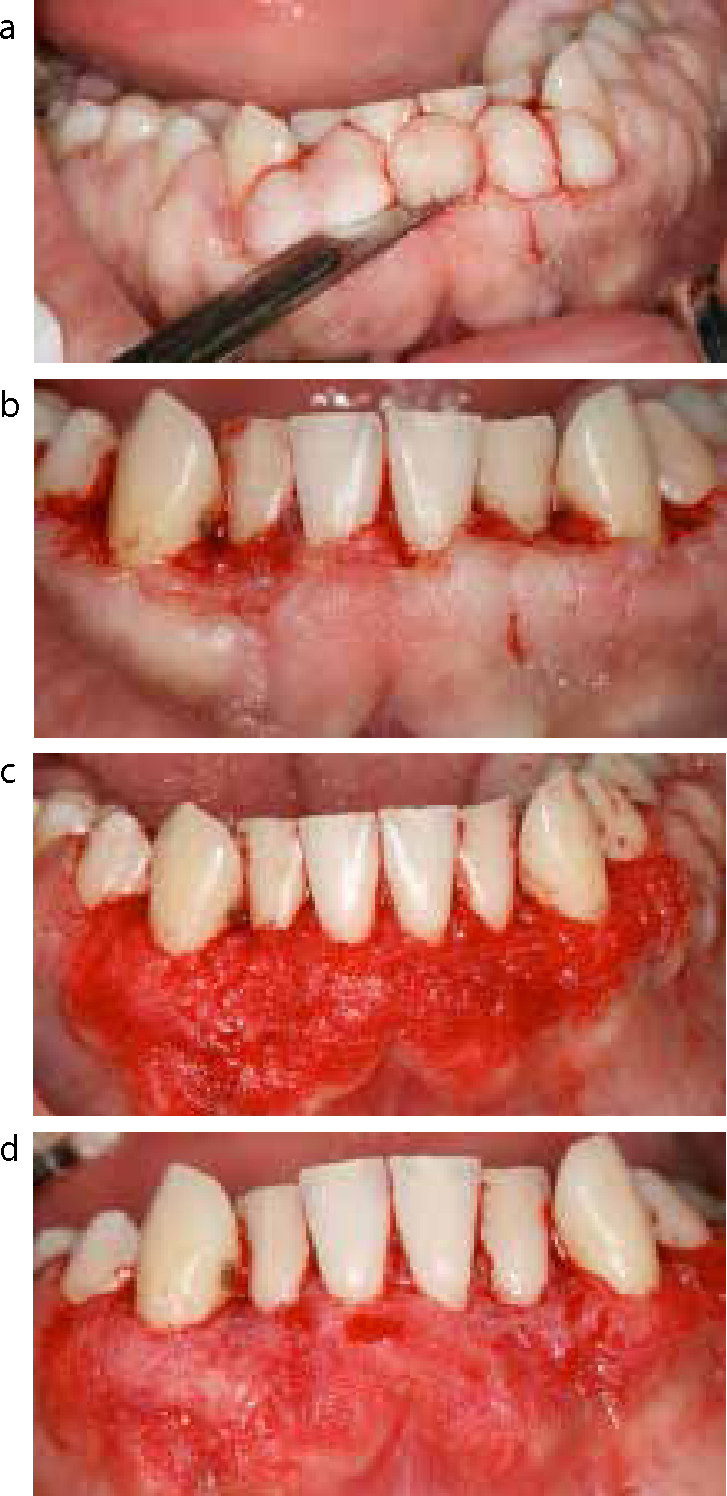
(a–c) A 26-year-old male patient presented to the periodontology department complaining of enlarged gingivae. He had previously been diagnosed with hereditary gingival fibromatosis and had undergone previous gingivectomy procedures under general anaesthetic. On examination he had extensive generalized gingival enlargement and the gingivae were firm and fibrous on palpation.
The treatment options were discussed with the patient and it was decided that the gingivectomy procedures would be undertaken under local anaesthetic over 4–6 sessions. Figure 6 shows the gingivectomy procedure that was undertaken. Externally, beveled incisions were utilized and, following the initial removal of excess tissue with a scalpel, a round bur in an air turbine handpiece was used to carry out the final recontouring of the gingivae (Figure 6).
Figure 6. Gingivectomy procedure: (a) the bulk of the excess tissue was removed using externally bevelled incisions, having first probed to feel for the CEJ of the teeth; (b) post initial soft tissue removal; (c) recontouring of the ridge was undertaken using a scalpel; (d) the final recontouring was completed using a round bur in an air turbine handpiece (Figure 7).Figure 7. The use of a round bur in an air turbine to undertake recontouring of the gingivae (gingivoplasty).
Apically repositioned flap surgery without bone removal
If there is a limited amount of keratinized tissue, then a gingivectomy alone is not indicated and, instead, an apically repositioned flap procedure is undertaken which allows the tissue to be preserved, but moved to a more apical position.
An example of a case presenting with drug-related gingival overgrowth, managed with a combination of gingivectomy and apical repositioning of the flap, without bone removal, is shown in Figure 8.
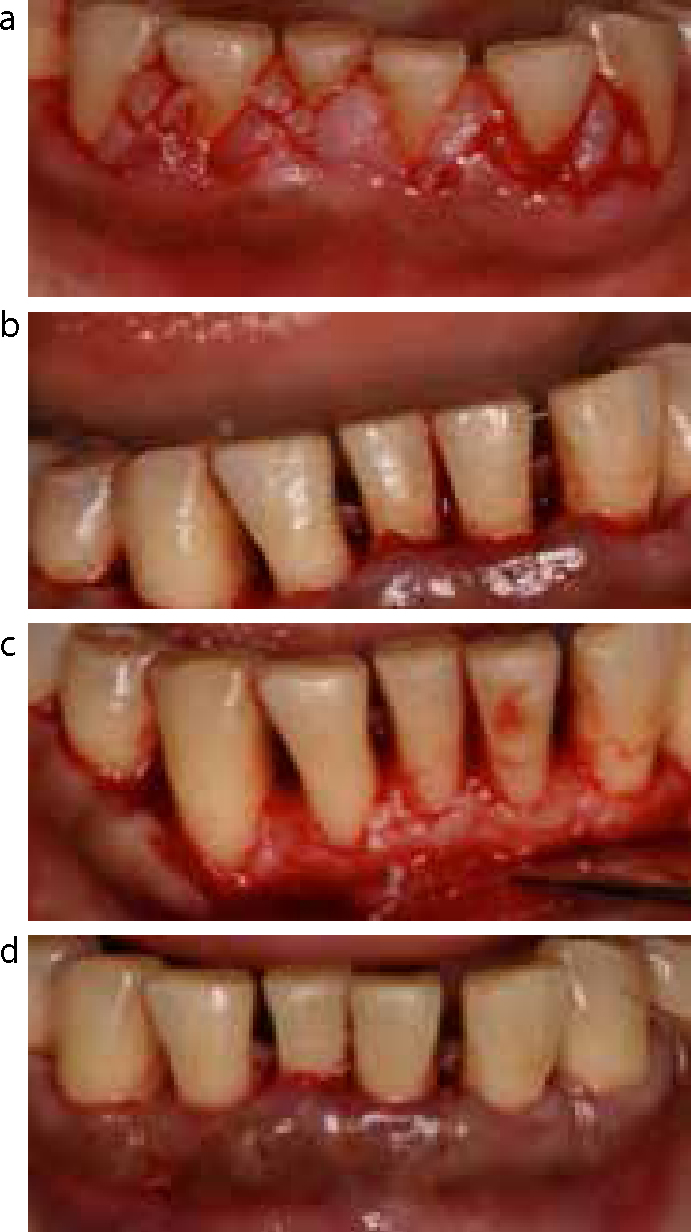
Figure 8. A 36-year-old female patient presented to the periodontology department complaining of swollen gums and occasional bleeding on brushing. The onset of the gingival enlargement coincided with her taking phenytoin, which she had been taking for 10 years for epilepsy. On examination, there was poor oral hygiene, with generalized gingival enlargement with marginal inflammation and generalized bleeding on probing and deep pocketing.
The treatment options were discussed with the patient and, following oral hygiene instruction and a course of non-surgical periodontal therapy, it was decided that gingivectomy in conjunction with open flap debridement was to be undertaken under local anaesthetic over 4–5 visits. Surgery involved external bevel incisions to remove the excess gingival tissue and underlying granulation tissue, maintaining the correct gingival contour. Subsequently, full muco-periosteal flaps were raised to allow open flap debridement prior to replacing the flaps at the new, more apical, position using a continuous resorbable suture (Figure 9).
Figure 9. Apically repositioned flap procedure: (a) the excess tissue was removed using externally bevelled incisions; (b) post initial soft tissue removal; (c) open flap debridement; (d) apical repositioning of the flap and placement of continuous suture.
Apically repositioned flap surgery with bone removal
The need for bone removal will depend on the position of the alveolar crest in relation to the CEJ. This procedure may be required in the management of patients with Type 2B altered passive eruption, where there is a normal width of keratinized tissue, but the alveolar crest is at the levels of the CEJ.
This procedure will be discussed in more detail in paper 2 of this 2-part series.
Post-operative care and healing
The patient should be advised to continue to maintain a high standard of oral hygiene within the rest of his/her mouth and to use a chlorhexidine-based mouthwash twice daily for a period of one week post-operatively. At the one week review appointment, if the periodontal dressing is still in place, it should be removed and the surgical site bathed in chlorhexidine and/or sterile saline solution. At this point the patient can be encouraged to re-commence brushing, initially using a soft surgical brush for the first 7–10 days. In extensive cases a stent can be made pre-operatively from a study cast to be used to aid haemostasis following surgery.
Studies have shown that the gingival margin does not stabilize until at least 20 weeks post-surgery;18 therefore, in the aesthetic zone, if any restorative work is planned, such as crowns or veneers, it should be delayed for at least this period of time.
Other techniques
Laser
Other techniques, such as the use of a laser for soft tissue resection, have also been reported in the dental literature. In 2006, Mavrogiannis and co-workers undertook a study to compare the rate of overgrowth recurrence between conventional gingivectomy, flap surgery and laser excision and, after six months, there was found to be significantly less recurrence in patients treated using laser excision.19 In 2011, McGuire and Scheyer published a case series of patients for whom they had undertaken external bevelled gingivectomies and other cases requiring osseous recontouring and apical flap repositioning, using an Er: YAG laser.20 The patients were followed up for between 6 months and 3 years and the data indicated stable aesthetic outcomes. However, a number of important observations were made, such as the creation of osseous troughs when using the laser to recontour the bone. In addition to this, laser-induced root surface pitting and scorching was noted by the operators and it was felt that this was difficult to prevent. It is the opinion of the authors that further work and more high quality, prospective, randomized clinical trials, with longer follow-up periods, are required before lasers can be recommended for surgical removal of gingival tissue excess.
Limitations and complications associated with intervention
The main complications that the patient should be forewarned about are:
The possibility of increased spacing between the teeth, which may compromise the aesthetics;
Patients should also be advised that, depending upon the reason for the enlargement, they may be at risk of recurrence of gingival overgrowth, and so may require further surgery in the future. If the patients have racial pigmentation of their gingivae, they must be forewarned that, following the surgery, the colour of their gingivae may be altered and become pinker in colour. Techniques can be employed to minimize this, such as avoiding externally bevelled incisions, however, they must still be made aware of this.