There is increasing recognition, made explicit in the new classification for periodontitis, that periodontitis is a lifelong disease that is not ‘cured’ but rather ‘managed’. This paper focuses on how the response to periodontal treatment is ideally measured and how decisions are made as to whether the treatment has been ‘successful’ or not. The roles of both the patient and practitioner in the maintenance of periodontal health for those patients who respond to initial therapy are crucial. Patients not responding to initial, non-surgical periodontal therapy also need to be appropriately managed, as outlined in this paper.
CPD/Clinical Relevance: This paper highlights the importance of maintenance of periodontal health, as an integral part of the overall management of patients with periodontitis, in order to minimize further periodontal breakdown and eventual tooth loss.
Article
Joanna Batt
In this paper, it be will assumed that the steps outlined in the previous papers have been followed and the patient with unstable periodontitis is adequately motivated, has had an initial course of periodontal treatment, and is now being reviewed after a period of at least 8−10 weeks (commonly at the 3-month time point). For the purposes of this paper, the terms ‘periodontal treatment’ or ‘periodontal therapy’ may be used instead of the longer (and more accurate) ‘non-surgical root surface debridement (NS-RSD)’. This paper will discuss:
How to measure periodontal treatment response;
What measures to look for in assessing periodontal treatment response;
How to assess success of periodontal treatment;
Challenges in periodontal maintenance;
Tips on helping patients who do not respond to initial periodontal treatment.
How to measure periodontal treatment response?
For most practitioners, the Basic Periodontal Examination (BPE) would be a familiar screening tool for entry into periodontal therapy. There is growing recognition, now reaffirmed by the 2017 World Workshop Classification and its UK adoption,1 that periodontitis is a lifelong condition. Once a patient has periodontitis, he/she is always more susceptible to this disease and therefore remains classified as a periodontitis patient. However, with adequate treatment, risk factor management and home care, the patient may be classified as having periodontitis which is ‘currently stable’.2 The benefits of the BPE as a quick and simple screening test are self-evident but its shortcomings as a tool to assess periodontal treatment response do need to be addressed. The BPE does not provide the practitioner or patient with site-specific information on key measures of periodontal health in a way that a Detailed Pocket Chart (DPC) can. The DPC allows the practitioner to review, for example, the mesio-buccal site on the UR6 to see if the site is changing in its appearance or phenotype with regard to probing depth, bleeding on probing, suppuration and other measures detailed below. Having this site-specific information, as opposed to the less detailed information contained in the BPE, allows practitioners to monitor the periodontal health of their patients with a history of (and therefore a susceptibility to) periodontitis appropriately, therefore allowing for early intervention, if needed.
What measures to look for in assessing periodontal treatment response
The measures available to assess treatment response (often called ‘outcome measures’) fall into two broad categories. Firstly, these may be clinical outcome measures (including laboratory measures in the future) and secondly, these may be patient-reported outcome measures (PROMs). In this section, the most common clinical and patient-reported outcome measures are considered, along with their pros and cons, and what can be expected if periodontal health is improving or stable.
Clinical outcome measures
Periodontal probing depth
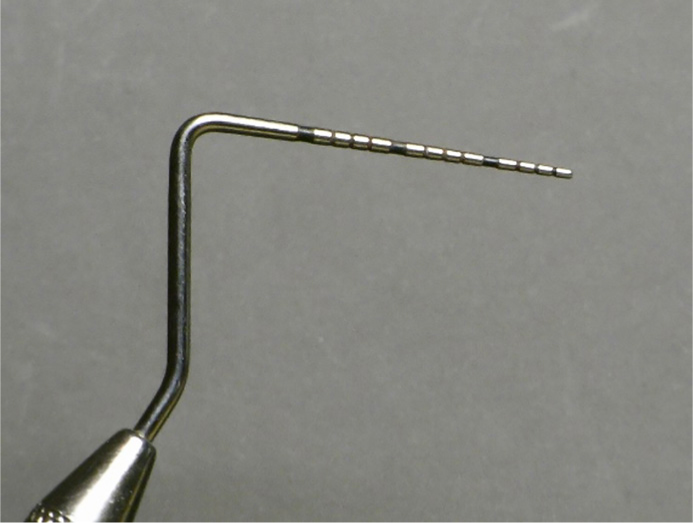
The periodontal probing depth is routinely recorded in DPCs and forms a key clinical outcome measure to assess periodontal health. It is commonly measured with a manual probe, such as the UNC-15 probe, and measures the probing depth (to the nearest millimetre) from the gingival margin to the base of the pocket (Figure 1).
Figure 1. UNC-15 periodontal probe.
The probing force should be between 0.20N and 0.25N, equivalent to 20−25 g. There are constant force probes available which maintain the desired probing force, which can be manual, such as the Chapple UB-CF-15 probe (Implantium, Shrewsbury, UK) or electronic, such as the Florida Probe (Clark Dental, UK). The primary benefit of using probing depth in a DPC is that it is quick to perform and provides an adequate level of detail. The downside of using probing depth is that the probing pressures and techniques can vary, leading to a loss of reliability when comparing probing depths within and between practitioners.3 Some of this downside is mitigated by constant force probes and error can be minimized by ensuring that, for any individual patient, the DPC is always recorded by the same clinician using the same type of probe.
In assessing periodontal treatment response, practitioners are ideally looking for a reduction in probing depths in sites which were previously ‘deep’ reduced to a depth of 4 mm or less.1 This anticipated reduction in probing depth is due to two main processes: firstly, recession, which is responsible for the apical migration of the gingival margin and, secondly, from re-attachment to the root surface by means of the long junctional epithelium. As reductions in probing depth can be a result of recession alone, clinical attachment loss is a more detailed measure of the patient's cumulative burden of periodontitis.
Clinical attachment loss (CAL)
Clinical attachment loss is a combined measure of recession and probing depth. Given that recession is measured from the cemento-enamel junction (CEJ) to the gingival margin and probing depth is measured from the gingival margin to the base of the pocket, CAL is simply the sum of the two, or the distance between the CEJ and base of the pocket. CAL as a measure can be superior to probing depth in that it provides more detail about the cumulative burden of periodontitis at a site-specific level. For example, consider two sites; both have a probing depth of 3 mm but one has CAL of 7 mm and the other has CAL of 3 mm. The former site has had more prior experience of periodontitis (assuming that periodontitis is related to the cause of recession) and therefore the former site is more prone to further periodontal breakdown and has a higher maintenance burden. The benefit of using CAL in addition to probing depth in a DPC is that it provides more detail, as mentioned earlier, but the downsides are that it is more time consuming, and the CEJ as a landmark may be obscured by direct or indirect restorations. It is fair to say that most clinicians in general practice rely on probing depth rather than CAL in terms of periodontitis measurements.
To assess treatment success, practitioners will look for stability in CAL over time or maybe reduction in CAL seen with re-attachment.
Plaque and bleeding scores
A plaque score aims to quantify the presence/absence of plaque on buccal, lingual/palatal and interproximal surfaces of all natural teeth. It is usually expressed as a percentage of all such scorable surfaces of teeth, and can be used as an indicator of levels of home care. Plaque score may also be used as a patient motivator as well as a guide to providing tailored Oral Hygiene Instructions (OHI). For example, the patient in Figure 2 demonstrates increased levels of plaque build-up. Baseline plaque scores can be used firstly to tailor OHI, and then be compared to subsequent scores in order to motivate the patient further (Figures 3−6).
Figure 2. Patient at presentation. Note plaque accumulation.Figure 3. Patient from Figure 2 after 6 weeks of implementing a tailored oral hygiene regimen alone.Figure 4. Patient from Figure 2 after 3 months of implementing a tailored oral hygiene regimen alone.Figure 5. Patient from Figure 2 immediately following non-surgical initial therapy.Figure 6. Patient from Figure 2 following 18 months of maintenance therapy.
Similarly, tailored OHI can be provided in regard to interproximal cleaning based on the localization of plaque as identified by the plaque score. Given that the presence of plaque beyond a threshold that the patient's immune response can tolerate is the main cause of periodontitis, the detriment of a high plaque score is self-evident. Arbitrarily, this threshold is set at 20% for patients but, in practice, this may need titrating as a plaque score of 20% could be too high for some patients looking to improve or maintain their periodontal health. The shortcomings of a plaque score is that, unlike a plaque index, it only records the presence or absence of plaque and not the quantity or localization of these deposits. This can make it a more stringent measure of plaque control. In addition, patients will often brush particularly well just prior to a dental appointment, thereby artificially lowering the plaque score below a level they would usually maintain; however, this challenge can be addressed by the bleeding score.
Bleeding scores are a dichotomous (presence or absence) record of bleeding associated with the buccal, lingual/palatal and interproximal surfaces of all natural teeth. It can be recorded as bleeding from the base of the pocket, following a DPC, or bleeding from the gingival margin, elicited by performing a marginal bleeding score. Bleeding on gentle manipulation of the base of the pocket or the gingival margin results from a breakdown of micro-ulceration at these sites, formed in response to local plaque deposits. As this micro-ulceration does not heal immediately following removal of the causative agent (plaque), bleeding can be used as a measure of somewhat longer-term plaque control, as opposed to the presence or absence of plaque alone. For example, if patients brush diligently just before their dental appointment but do not do so regularly, they may present with a low plaque score but still have a high bleeding score. Again, somewhat arbitrarily, the threshold of ‘high’ bleeding score has been set at 10% or more. In reality, this again needs customizing to the individual patient in the chair. Care should be taken in assessing bleeding on probing as it is a subjective measure and can be especially problematic in smokers where bleeding may be masked.
Hence, for these outcome measures, the purpose of maintenance is attaining and maintaining a level of plaque and bleeding conducive with periodontal health in the particular patient. Sequential recording of plaque and bleeding scores can help personalize this threshold, as well as informing and motivating the patient.
Suppuration
Suppuration, or pus formation, is a sign of infection. In the maintenance phases of periodontal therapy, resolution of suppuration is aimed for. If resolution does not occur, the initial diagnosis must be confirmed, as a mis-classified endo-perio lesion case would not respond to periodontal therapy alone and may present with persistent suppuration. If the origin of suppuration is confirmed as periodontal, and there is no resolution even after good care on the part of the dental care provider as well as the patient, both in terms of home care and risk factor management, then other systemic pathology may need to be considered. Multiple, recurrent periodontal abscesses are sometimes seen in patients with undiagnosed or poorly controlled diabetes and other co-morbidities.
Mobility/drifting
Mobility and drifting of teeth are both features of periodontitis, resulting from a loss of alveolar bone support. Mobility existing as a result of the presence of periodontal disease but exacerbated by an occlusal component, known as secondary occlusal trauma, may need further management of the occlusal contributor once periodontal health is established. This may take the form of hard, full coverage, occlusal splints (Michigan/Tanner type splints) or non-rigid periodontal splinting or occlusal adjustments. The last option should be reserved for the most severe cases and may warrant referral for treatment planning and delivery. Improvements or lack of progression in mobility and drifting can be considered measures of periodontal stability.
Radiographs
In the majority of cases of periodontitis, bone loss is irreversible with conventional, non-surgical periodontal care. The need for radiographs to assess treatment response or maintenance alone is therefore not currently justified. However, in certain cases, such as furcation lesions or Stage IV bone loss, individual teeth may warrant clinical and radiographic monitoring, but this should be decided on an individual clinical basis.
Other outcome measures
Other outcome measures, which are not currently widely used but may play a part in future care of patients, include the use of ‘biomarkers’. Biomarkers are biological substances (for example bacterial strain, inflammatory cytokines and others) that can be used to identify a particular disease process. For example, in rheumatoid arthritis, antibodies to altered proteins can be detected in patients long before arthritis is clinically detected, therefore antibodies are used as biomarkers of the disease. In periodontitis, advances in salivary biomarkers may mean that, in the future, saliva samples can be employed as a way of measuring periodontal health, treatment response, or the success of maintenance regimens as a potential adjunct to the other measures and scores described above.
Patient Reported Outcome Measures (PROMS)
While the clinician may be interested in probing depths and plaque and bleeding scores, most patients will not measure the outcome of treatment in these terms. With education, this may change and patients will often want to discuss their plaque score and ways to reduce this. For most patients, the outcome of treatment is measured in aspects such as reduction in bleeding on brushing, reduction or resolution of pain, reduction in mobility, improvement in aesthetics and ultimately tooth retention. These aspects are not currently routinely collected in general dental practice as ways of evaluating the treatment response to periodontal therapy. As there is a growing recognition of the shared role of the patient in healthcare, future treatment outcomes may incorporate some aspects of PROMs.
How to assess success of periodontal treatment
Given the numbers and types of outcome measures that can be used to assess periodontal treatment response, and the various pros and cons of each measure, it will come as no surprise to the reader that assessing the success of periodontal treatment requires a combination of outcomes (both clinical and patient reported) and clinical judgement. The UK adoption of the 2017 World Workshop Classification1 provides some guidance on what may be classified as successful periodontal treatment and maintenance (Table 1).
Intact periodontium
Health
Gingivitis
Probing attachment loss
No
No
Probing pocket depths (assuming no pseudo pockets)
≤3 mm
≤3 mm
Bleeding on probing
<10%
≥10%
Radiological bone loss
No
No
Reduced periodontium non periodontitis patient
Health
Gingivitis
Probing attachment loss
Yes
Yes
Probing pocket depths (all sites and assuming no pseudo pockets)
≤3 mm
≤3 mm
Bleeding on probing
<10%
≥10%
Radiological bone loss
Possible
Possible
Successfully treated periodontitis patient
Health (stable)
Gingival inflammation in a patient with history of periodontitis (remission)
Probing attachment loss
Yes
Yes
Probing pocket depths (all sites and assuming no pseudo pockets)
It is important to note that a higher probing depth of 5 mm or 6 mm in the absence of bleeding may not necessarily represent active disease in particular soon after peridontal treatment
*A successfully treated periodontitis patient, in whom sites of gingival bleeding appear, remains at high risk of disease recurrence at those sites and of progressive attachment loss. Therefore, gingival inflammation is defined as bleeding at a shallow site of ≤3 mm rather than ≤4 mm, as is the case in gingival health. Where the probing depth is 4 mm with bleeding, or higher, this is no longer a ‘closed pocket’ and is assumed to be unstable periodontitis.1
In particular, this identifies probing depth of 4 mm or less, with no bleeding at sites of probing depth 4 mm and a bleeding score of less than 10% as being ‘stable’. If the previous criteria are met but the bleeding score is greater than or equal to 10%, the patient is classed as being in ‘remission’. This situation may improve following tailored oral hygiene and generalized supragingival debridement along with risk factor management. Finally, if probing depths of 5 mm or more exist, or if there is bleeding on probing at sites of 4 mm, the patient's periodontal health is considered ‘unstable’. As well as the management strategies used for the periodontitis patient in remission, these patients may require further root surface debridement and periodontal care.
Challenges in periodontal maintenance
From the previous sections, it should be apparent that maintenance of periodontal therapy is an essential part of the care provided to such patients. Numerous studies have shown the benefit of supportive periodontal therapy in outcomes in periodontitis, including tooth retention. The role that the patient plays in this, by way of at least twice daily disruption of the supra- and sub-gingival biofilm using toothbrushes, floss and interdental brushes, is paramount. Given the burden of care for the patient, both in terms of biofilm disruption and risk factor management, it is easy to understand why some patients may find this difficult to maintain without professional support. The frequency and costs of appointments, as well as any underlying dental anxiety, coupled with falling into old habits developed over decades, all work against the practitioner trying to improve the patient's periodontal health.
Patients can be motivated in this journey by regular (3-monthly) visits to a dental care professional for plaque and bleeding scores, reinforcement and personalization of oral hygiene instruction, and generalized supragingival debridement. Repeating the DPC at every or alternate 3-monthly appointments may be appropriate. Regular DPCs allow for the early identification and treatment of recurrent periodontal disease. Patients must feel positive about their healthcare interventions and perceive the intended benefits of their home care regimen in order to increase the chances of compliance.4 The consequences of not adhering to their appointment schedule and home care routine as prescribed must be clear. These discussions should be recorded in the patient's notes.
The evidence for a three-monthly maintenance regimen is based upon the knowledge that sufficient time needs to be allowed in order for development of the long junctional epithelium, re-establishment of the sub-gingival flora and maturation of healing following surgery.5 Three months also allows time for patients to get used to, or adapt to, their existing oral hygiene regimen from a previous visit, and longer term plaque control can be monitored post prophylaxis.
Tips on helping patients who do not respond to initial periodontal treatment
There is a spectrum of interventions when particular periodontal sites appear to be non-resolving, or if a patient does not achieve the anticipated level of resolution following periodontal interventions. They range from simple to more involved:
Simple steps:
Is the patient's diagnosis accurate? Consider the possibility of any other components to this patient's periodontitis, for example an endo-perio lesion, secondary occlusal trauma involvement, or a root fracture.
Was the instrumentation of the initial course of periodontal therapy adequate? Do the root surfaces feel smooth (supra- and subgingivally) when gently felt with a BPE probe? Retained calculus deposits may act as plaque retentive factors.
Is the patient managing to maintain adequate oral hygiene? This needs to be documented using full mouth plaque and bleeding scores paying particular attention to the assessment of interproximal cleaning. As discussed above, this is a major reason for failure of periodontal therapy and something that patients need to be re-motivated about. If recession has occurred, then interdental cleaning may need to be re-assessed using different OH aids, for example a larger interdental brush size may now be needed.
Is the patient managing other periodontal disease risk factors? For example smoking, lack of antioxidants and poor diet, stress.
Are there local risk factors associated with non-resolving pockets? For instance furcations, overhanging restorations, excess cement from indirect restorations.
Once the ‘simple’ causes are addressed, the practitioner can investigate the presence of more complex causes for failure of treatment.
Complex steps:
Are there any ‘uncommon’ risk factors present? Ensure that there are no more unusual local plaque retentive factors, such as root grooves.
Is medical or pharmacological management needed? For example, poorly controlled diabetes, drug-induced gingival overgrowth.
For isolated sites that do not respond to treatment in the presence of good oral hygiene and the absence of other complicating factors which could be resolved:
Consider local antimicrobial use;
Consider periodontal surgery to improve physical and visual access to root surface to improve instrumentation or oral hygiene maintenance;
Consider referral to secondary care if sites remain despite checking the above.
Conclusions
Maintenance is of paramount importance in the successful management of periodontal disease. As discussed above, periodontal disease is not a condition which can be considered as ever being fully treated, and it is expected that patients will have specific sites in their mouth, or times in their life, when the disease becomes more active. The identification of these areas and sites is therefore essential and, as noted, the patients' home care regimen is often encouraged and informed by measures of current periodontal status.