Assessing periodontal health and the british society of periodontology implementation of the new classification of periodontal diseases 2017 Mike R Milward Anthony Roberts Dental Update 2024 46:10, 707-709.
Professor and Honorary Consultant in Periodontology, The School of Dentistry, College of Medical and Dental Sciences, University of Birmingham, 5 Mill Pool Way, Edgbaston, Birmingham B5 7EG
Periodontal disease is a highly prevalent, chronic, inflammatory condition which is a major contributor to tooth loss and poor oral health-related quality of life. For the vast majority of patients, the disease is entirely preventable/manageable often aided by input from dental health professionals. As dental health professionals, understanding the periodontal disease process, the risk factors associated with it, standardized ways of detecting, diagnosing and monitoring the disease, along with the special tests needed to aid this process are essential skills for successful disease management.
This article summarizes the need for assessing periodontal disease including key aspects of detection, a brief history of periodontal disease classification and the new classification. The paper goes on to discuss the British Society of Periodontology implementation plan of new classification and how this can be utilized for use in general dental practice.
CPD/Clinical Relevance: This paper introduces the practitioner to the 2017 Classification of Periodontal Disease along with how this is implemented in general dental practice. The paper provides useful cases for practice as well as flowcharts to aid diagnosis.
Article
Mike R Milward
Periodontal disease is a chronic inflammatory disease that affects approximately 45% of the adult population.1 The disease is driven by development of a plaque biofilm but the majority of periodontal tissue damage is as a result of an exaggerated host inflammatory response.2 A number of risk factors impact on periodontal disease resulting in initiation or exacerbation of the disease process, examples include smoking, poor plaque control and unstable diabetes.
The importance of periodontal disease cannot be underestimated. It has a major impact on patients' self-esteem and can result in tooth loss, which compromises aesthetics and dietary intake.3 Periodontal disease management is labour intensive and time consuming, requiring long-term maintenance following successful treatment, resulting in a significant healthcare burden.4 The impact of periodontal disease on a range of systemic conditions has further raised the profile of this prevalent and debilitating disease.5
Periodontal disease cannot be cured but can be successfully managed and treatment outcomes are significantly affected by early diagnosis and prompt therapeutic intervention.6 Key to early diagnosis is adequate screening using the Basic Periodontal Examination (BPE) in order to identify patients that require further investigation. The accumulated clinical and radiological findings (alongside the results from any special investigations) assist the clinician in the process of determining an accurate periodontal diagnosis.
In order to arrive at an accurate diagnosis, a classification scheme needs to be utilized which will in turn lead to appropriate treatment options and then, following discussion with the patient, an agreed treatment plan or strategy.
There have been a number of classification schemes for periodontal disease developed over the years (Table 1). These have been introduced as understanding of the aetiology of disease has advanced. These changes can be frustrating for the busy practitioner but are important to ensure that what drives disease development and progression is fully understood.
Year Proposed
Responsible Body
Key Changes
1806
Joseph Fox
First recorded classification of ‘Gum Disease’
1942
Orban
First classification recognized by the American Academy of Periodontology
International Workshop on Periodontal Classification12
‘Chronic adult periodontitis’ replaced with ‘Chronic periodontitis’
‘Early onset disease’ replaced with ‘Localized or generalized aggressive disease’
Gingivitis classification introduced
This article aims to summarize the key aspects in detecting periodontal disease, the importance of disease classification and to introduce the New Classification for Periodontal Disease 2017,7 including the British Society of Periodontology implementation plan,8 which was designed to help its introduction into general dental practice.
Assessing periodontal disease
This stimulus for the present publication is primarily the publication of the New 2017 Classification of Periodontal Diseases.7 Of course, a new classification scheme does not alter the clinical presentation and features of patients with periodontal disease, rather the framework for the process is affected. It remains an unfortunate fact that, for many patients, the signs and symptoms of periodontal disease either go unnoticed or are ignored by patients, and it is only when key aspects of the patient's history and the subsequent examination are undertaken that the significance of his/her condition is realized. When periodontitis is allowed to progress unnoticed, regrettably many of the features of advanced disease, such as tooth mobility and tooth drifting, prompt the patient to seek dental care but, by that time, the ideal window of opportunity may well have passed. The term ‘periodontal disease’ is often misunderstood or misinterpreted across the profession to mean ‘periodontitis’. In fact, periodontal disease is an umbrella term that is used to describe both gingivitis and periodontitis and this potential confusion is further compounded by the fact that gingivitis and mild to moderate periodontitis are often indistinguishable from a patient's perspective. From a clinician's perspective, the use of a periodontal probe in the clinical assessment process is essential and fundamental. This key clinical examination will be discussed further below.
The acquisition of information for clinical assessment starts with the patient history and the chief complaint of the patient, which can assist the clinician in determining the diagnosis and management priorities for the patient. Given the aforementioned potentially ‘silent’ nature of periodontal diseases, there may be a need for the clinician to prompt the patient about any gingival bleeding when brushing, mobile teeth or swellings that they may have experienced.
Risk factors may be local, systemic, or both, and the medical, dental, family and social history are opportunities to explore these in greater depth. Medications, diabetic status and glycaemic control, smoking habits, brushing and interproximal cleaning habits/regimens, previous extractions, etc may all give a useful insight into what might be contributing to their condition, identifying therapeutic opportunities and providing an indication of success (or otherwise) of treatment. Indeed, addressing risk factors for periodontal diseases should be at the forefront of the clinician's mind when outlining treatment strategies, as failure to address these is likely to bode poorly for treatment outcome. In terms of the new classification system, these risk factors are termed ‘grade modifiers’ and relate to the progression rate of the disease, responsiveness to standard therapy and potential impact on systemic health.
Table 2 is a list of clinical features that should be considered when undertaking an examination of the periodontal tissues which, if significant issues are found, would also lead to a radiographic assessment of the teeth affected. In day-to-day clinical practice, the Basic Periodontal Examination (BPE, formerly CPITN) is the screening tool used by clinicians to alert them to those patients who require further investigations in the form of detailed periodontal charting and radiographic assessment (Table 3).15,16
Visual use of probe and/or calculated from probing depth and recession measurements
Bleeding on probing§
Visual use of probePerformed as part of BPE, marginal bleeding score or detailed periodontal chart
Tooth mobility (or hypermobility)
Visual assessment using indexeg Millar's mobility index
Furcation involvement of tooth
Visual assessment and use of probe using score (eg BPE) or index (eg Hamp et al14)
Levels of plaque, presence and location of calculus
Visual assessment and use of probe
Presence and location of plaque retention factors
Visual assessment and use of probe
Presence or absence of pus
Visual assessment and use of probe
*A particular focus on interdental attachment loss when assessing buccal recession defects and identifying historic periodontitis. § Determines criteria for health vs gingivitis, current periodontal status (stability/remission/unstable).
Scoring Code
BPE Probing Depth
First Black Band on Probe
Actual Pocket Depth Range
BOP
Calculus/Overhangs
0
Pockets <3.5 mm,
Entirely visible
<3 mm
No
No
1
Pockets <3.5 mm,
Entirely visible
<3 mm
Yes
No
2
Pockets <3.5 mm,
Entirely visible
<3 mm
Possible
Yes
3
Probing depth 3.5−5.5mm
Partially visible
4−5 mm
Possible
Possible
4
Probing depth >5.5 mm
Disappears
≥6 mm
Possible
Possible
*Furcation involvement − if identified (visibly or on probing) this should be recorded in addition to the numerical score.
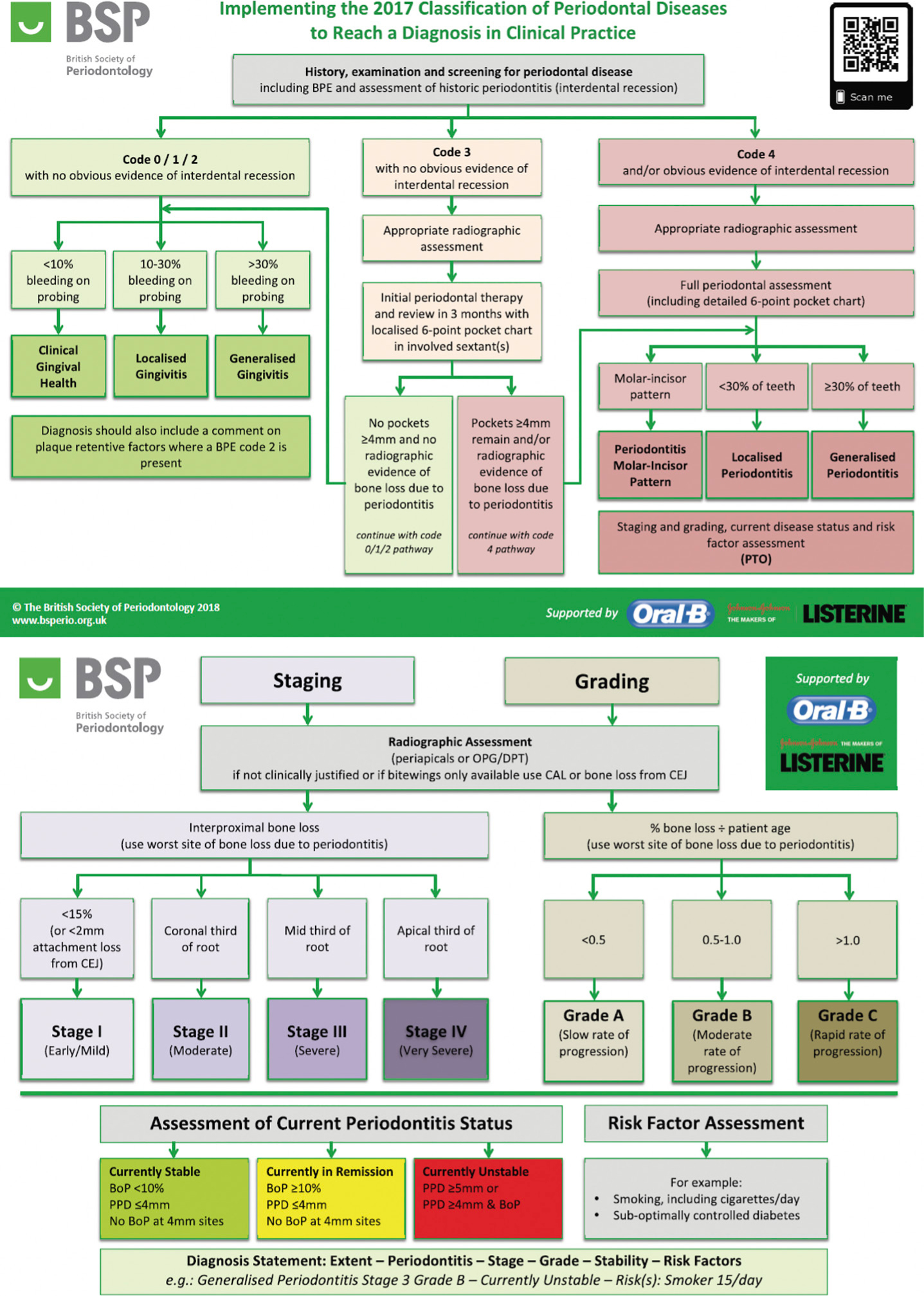
The BPE has never attempted to be a diagnostic tool, rather a periodontal alert mechanism for practitioners, however, the British Society of Periodontology (BSP) has recently produced an ‘implementation in clinical practice’ paper8 which grapples with the difficulty of integrating the new classification system into a useful scheme for practitioners. A useful algorithm has been produced in the paper which has been further supplemented by an info-graphic produced by the BSP (Figure 1) which has the BPE embedded within its content. The primary purpose of the BPE remains unchanged and its integration within the practitioner's guide still ensures that it is an assessment gateway.
Figure 1. The British Society of Periodontology Implementation of the 2017 Classification of Periodontology flow diagram.
Why and how do we classify?
A majority of diseases have classification schemes associated with them. These are useful in assisting clinicians to utilize appropriate treatment strategies for their patients based on clinical trials which provide evidence for the best treatment regimen. This equally applies to the management of periodontal disease. Disease classification also provides important frameworks to study the aetiology and pathogenesis of a specific disease, thereby allowing for development of new therapeutic strategies for disease management. In addition, a classification system allows for the use of a common international language, allowing practitioners to discuss patient management and the underpinning research in order to help provide the best patient outcomes.
An ideal classification scheme would involve use of the specific aetiological agent for a specific disease. An example of this would be Tuberculosis (TB): this disease is caused by a bacterial infection with Mycobacterium tuberculosis. Therefore, in this case, classification is straightforward and specifically relates to the causative factor. Unfortunately, it is not as straightforward in the case of periodontal disease, which has a multifactorial aetiology initiated and driven by a complex microbial biofilm, but the majority of the tissue damaged is caused by an exaggerated host inflammatory response. So classifying periodontal diseases proves a harder challenge.
The history of periodontal classification
Looking back in the literature, the first recorded classification system for periodontal disease was by Joseph Fox in 1806, who offered the first attempt to classify ‘gum disease.’ Since then, a number of different systems have been proposed. The first classification scheme to be accepted by the American Academy of Periodontology (AAP) was by Orban in 1942. Nearly 25 years later, in 1966, the AAP convened a workshop which resulted in a new classification. This was further revised in 1986.10 In 1989, an additional AAP meeting was held and further amendments made, including rate of disease progression, presence/absence of systemic disease, local risk factors and the patient's response to therapy.11 However, this classification omitted a classification of gingivitis and did not include the implications of systemic disease. The next landmark in periodontal disease classification was in 1993 when a European Workshop11 convened. This group considered the 1989 classification too complex, and simplified it, allowing clinicians to exercise more clinical judgement. This workshop introduced a number of proposals, which met with worldwide approval, but it was subsequently felt that it lacked sufficient detail to enable classification of the range of periodontal diseases that a practitioner may encounter and need to treat. As a result, a worldwide workshop met in 199912 and, based on the literature at the time, proposed a new classification with key features, including ‘Aggressive periodontitis’ which replaced ‘Early onset disease’ and ‘Chronic periodontitis’ which replaced ‘Chronic adult periodontitis’. In addition, a classification of gingivitis was introduced for the first time. This has worked well over the last 18 years, but research and understanding of periodontal disease and its pathogenesis has expanded in this time, meaning a new more appropriate classification was required. A summary of the history of periodontal disease classification can be seen in Table 1.
Why is the new system being introduced?
The aim of the 2017 World Workshop7 was to introduce a new classification that was driven by a better understanding of periodontal disease since the last classification workshop in 1999. The aims of the 2017 workshop, which were set out by the management committees of the European Federation of Periodontology (EFP) and the American Academy of Periodontology (AAP), were to produce a new evidence-based classification that could be implemented in general practice and that breaks down a complex disease process into key components that are important in determining disease severity, extent, and susceptibility to further disease progression, something the previous classifications have failed to achieve. In addition, patients who have experienced periodontal disease have a greater risk of further disease progression, so we need to be able to identify the current periodontal status as well as any previous history of periodontal disease. For the first time, the 2017 classification offers clear definitions of health and gingivitis for:
Patients with an intact periodontium;
Patients with a reduced periodontium due to causes other than periodontitis;
Patients with a reduced periodontium due to periodontitis.
The details and rationale that underpin these definitions are beyond the scope of this article but can be found in the paper published as a result of the 2017 World Workshop.7
The New Classification
The 2017 classification of periodontal disease has a number of key changes and extra detail that allows for better definition of our patients' diseases. The new system also includes details which are important in ensuring appropriate management strategies. One of the key changes from the 1999 classification is that ‘Aggressive’ periodontitis no longer appears in the new classification. The reasoning behind this is that clinical and biological research fails to clarify aggressive periodontitis as a distinct disease entity from chronic periodontitis, but rather as part of the same disease process. Other key elements include:
The introduction of ‘Staging’ and ‘Grading’;
‘Necrotizing Periodontal Diseases’ remain as a distinct category;
Endodontic-periodontal lesions being classified based on signs and symptoms that directly impact on prognosis and treatment;
Periodontal abscess being defined as acute lesions characterized by localized pus accumulation within the gingival wall.
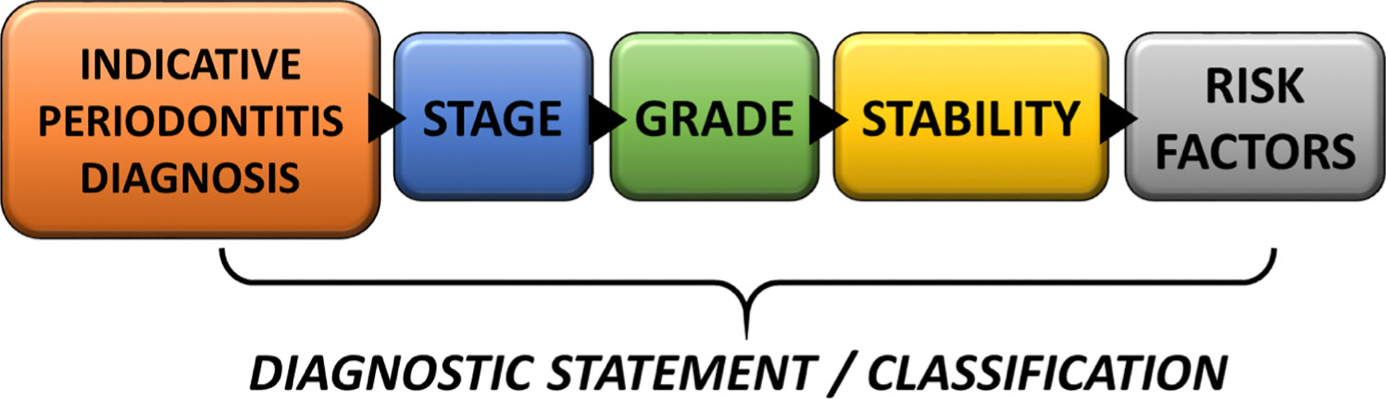
So classifying periodontal disease requires a number of steps (Figure 2).
Figure 2. Component parts of the New Classification of Periodontal Disease.
1. Indicative diagnosis of periodontitis
Arriving at a diagnosis for a patient continues to involve a comprehensive history, which includes identification of any systemic risk factors and a thorough clinical examination, including the BPE and radiographic examination where appropriate. The importance of the BPE cannot be overstated, as it is a fundamental gateway examination that indicates potential periodontal disease and has been discussed earlier in this article. One of the key clinical additions to the BPE examination in the new classification is the identification of interdental attachment loss, which is a key clinical indicator of previous periodontal disease experience. Even if the clinical examination identifies BPE scores of 0, 1, 2 or 3, if there is evidence of interproximal attachment loss this will result in a diagnosis of ‘Periodontitis’. Once an indicative diagnosis of periodontitis has been identified, the pattern of bone loss from radiographs is determined. If the bone loss is isolated to molar and incisor, then the pattern is ‘Periodontitis molar/incisor pattern’. If less than 30% of teeth have periodontal disease associated bone loss, the pattern is ‘Localized periodontitis’. If the bone loss exceeds 30% of teeth, then the pattern is ‘Generalized periodontitis’. Once a periodontitis has been identified, the next step is to ‘stage’ the patient.
2. Disease ‘staging’
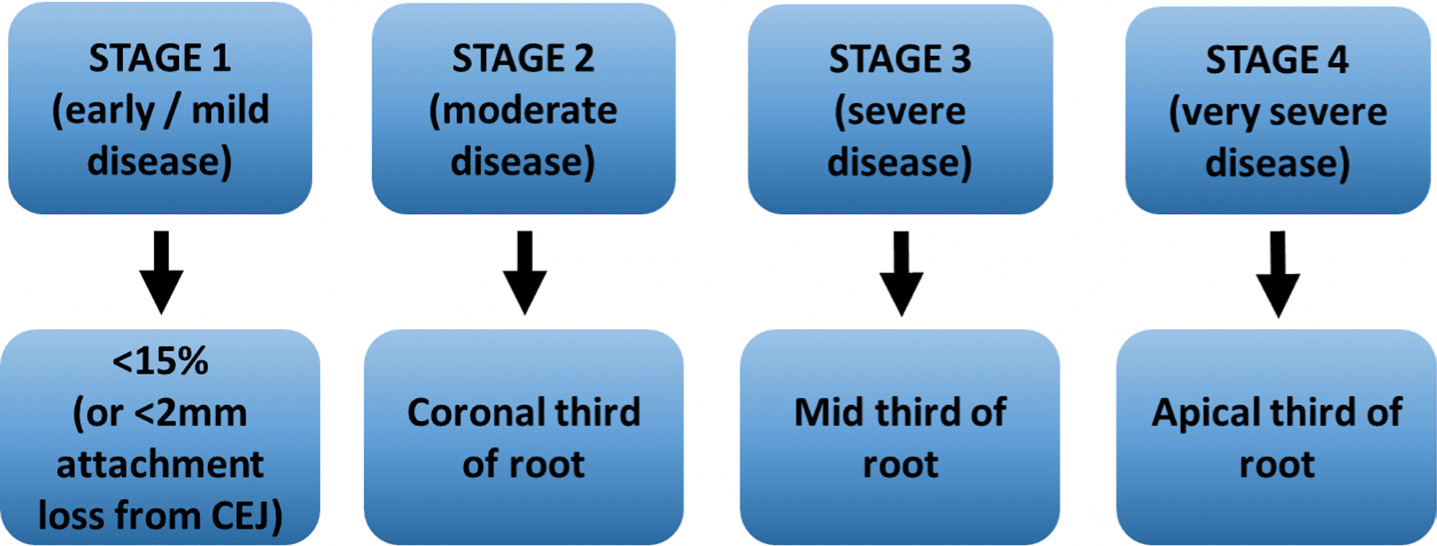
Staging aims to indicate the severity of disease, which will reflect the complexity of patient management. Staging utilizes the percentage bone loss at the worst site due to periodontal disease (Figure 3).
Figure 3. ‘Staging’ of periodontal disease.
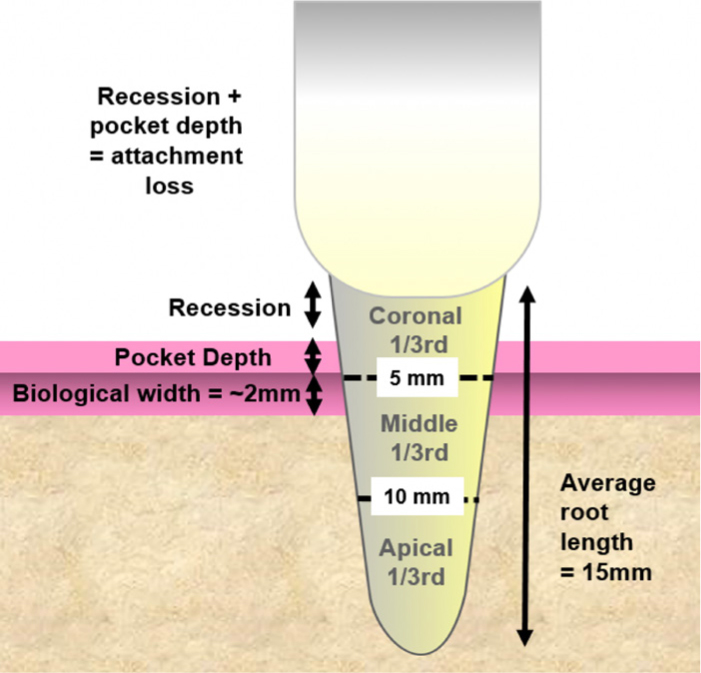
The ability to stage and grade a patient requires access to radiographs and this is not an issue with cases that score 3 or 4 BPE, where there is justification, and indeed a requirement, to take radiographs. However, where this becomes an issue is in relation to cases with a BPE of 0, 1 or 2, where radiographs cannot be justified on periodontal grounds. If radiographs are taken for other reasons, or recent radiographs are available, these can be used for staging or grading. However, if this is not the case, then Stage 1 (mild disease) can be determined if there is <2 mm attachment loss from the cemento-enamel junction (CEJ). The assessment of cases Stage 2−4, however, become problematic. One solution is to estimate the bone level clinically. The authors propose that this can be achieved by measuring recession and pocket depth using the worse tooth with interproximal recession, adding the biological width (~2 mm) to give an estimate of the distance that the bone crest is from the CEJ. If an average root length of 15 mm is taken (canines will be around 15 mm and incisors closer to 12 mm), it can be estimated whether the tooth has Stage 2 (coronal third), Stage 3 (mid third) or Stage 4 (apical third bone loss). In addition, this can be used to estimate percentage bone loss for grading. A summary of how this is calculated can be seen in Figure 4.
Figure 4. Estimating level of bone loss when radiographs not available.
An example of how this might work would be a patient who has a BPE Code 1 but obvious interproximal recession. The worst site of interproximal recession is chosen and this measures 4 mm, the pocket is 2 mm, the biological width is 2 mm (average standard measurement of the biological width). This makes the bone level to be estimated at 8 mm from the cemento-enamel junction (CEJ) and the average root length 15 mm. So, in this situation, the bone loss extends to the middle third, ie a Stage 3. (This would also equate to approximately 50% bone loss, which can be used in ‘grading’ of this case).
Obviously, if radiographs are required (BPE Code 3 and 4) or are already available, then an assessment of the worst bone loss due to periodontal disease can be made and an appropriate grading determined.
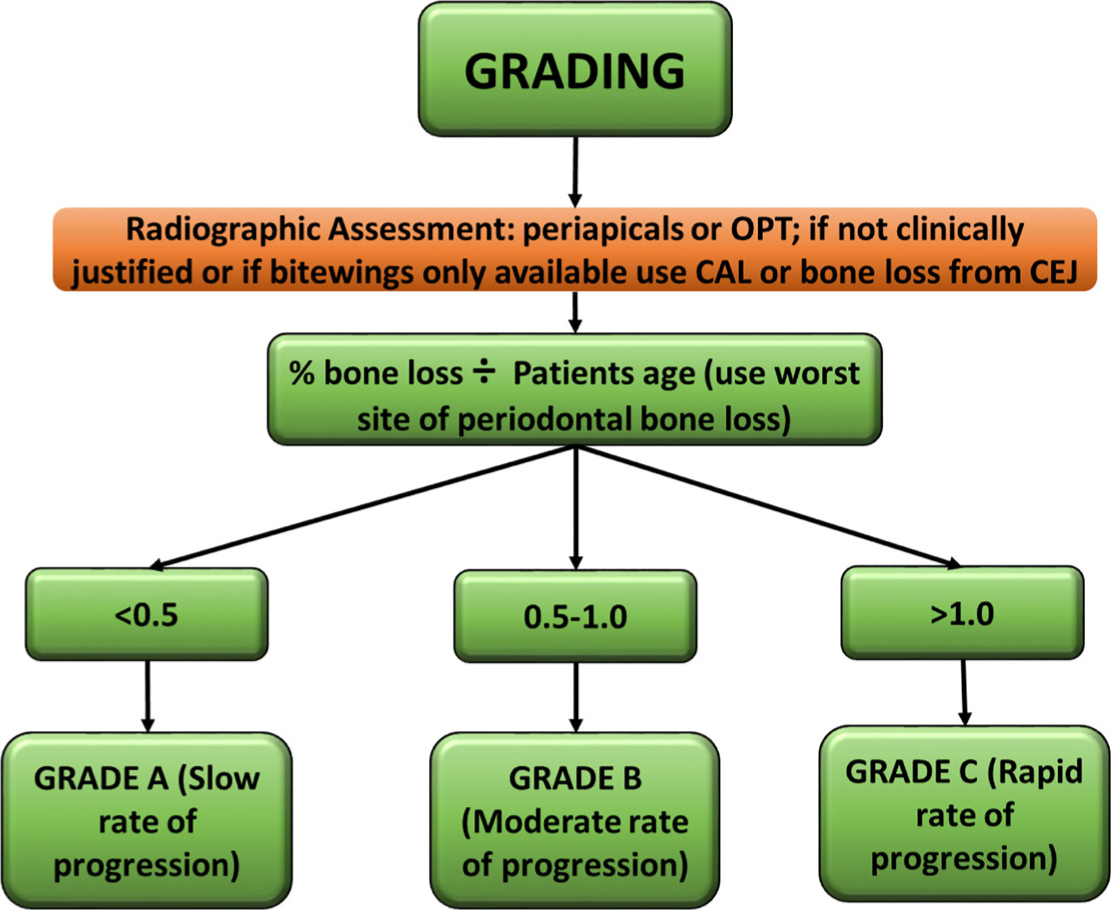
3. Disease ‘grading’
‘Grading’ aims to help identify how susceptible a patient is to periodontal disease by using the worst site of bone loss due to periodontal disease along with the patient's age. This will give an assessment of the rate of progression. The BSP implementation group looked at a range of thresholds of age versus bone loss to determine the most appropriate cut off. These are arbitrary but allow for easy calculation and were deemed clinically appropriate (Figure 5).
Figure 5. ‘Grading’ of periodontal disease.
In order to determine a grade for the patient, the worst site of bone loss due to periodontal disease is calculated as a percentage (if radiographs aren't justified, as previously discussed, estimate bone loss, as described in the previous staging section), then divide this by the patient's age. This gives a ratio, with <0.5 indicating a slow rate of progression, 0.5−1.0 a moderate rate of progression and >1.0 a rapid rate of progression.
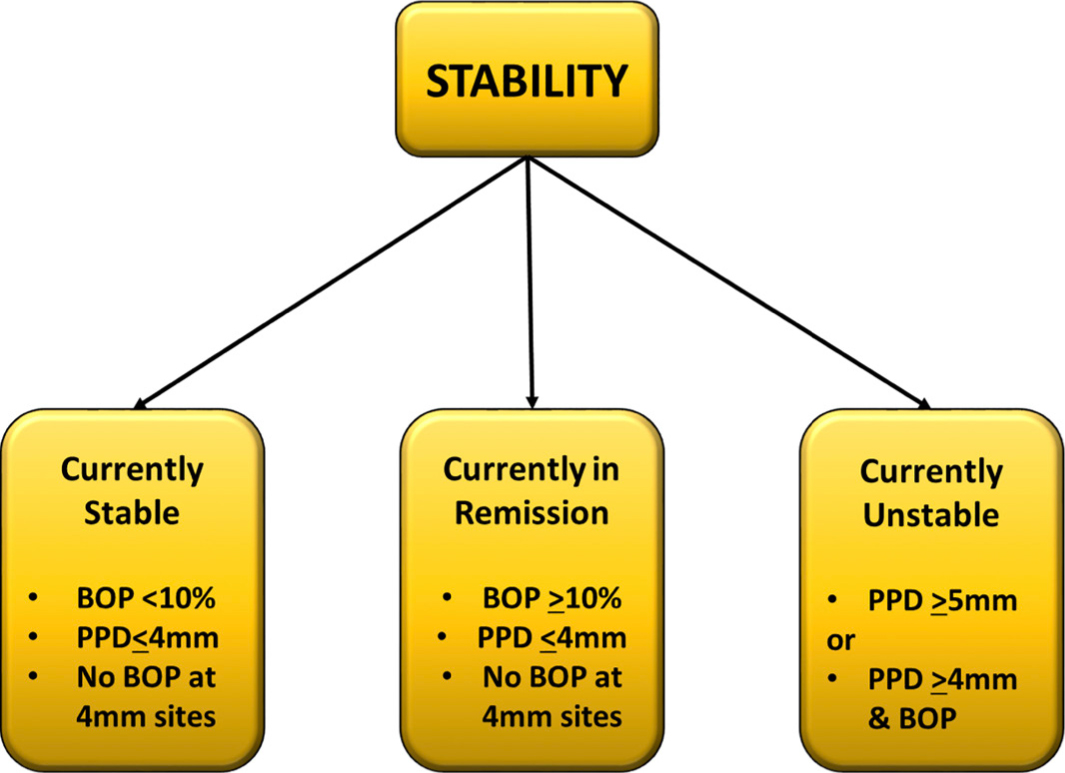
4. Assessment of disease ‘status’
It is important to determine the patient's current disease status. A patient may have historic periodontal disease, which the new classification identifies but may be currently stable. In previous classifications, a BPE screen did not identify this situation. This was a concern as patients who have had a history of periodontal disease are at higher risk of further periodontal disease progression and require long-term maintenance. The new classification allows such cases to be correctly identified and utilizes probing pocket depth (PPD) and percentage whole mouth bleeding scores in order to determine stability. If the patient has a PPD less than or equal to 4 mm and less than 10% bleeding on probing (BOP), then the case is ‘currently stable’. A patient with PPD less than or equal to 4 mm, greater than or equal to 10% BOP, and no BOP at 4 mm, the site is ‘currently in remission’, and if there is PPD greater or equal to 5 mm or PPD greater than or equal to 4 mm with BOP, then the case is ‘currently unstable’ (Figure 6).
Figure 6. Assessment of disease ‘status’.
5. Identification of ‘risk factors’
We are aware of the importance of risk factors that have the potential to impact development and progression of periodontal disease directly. Therefore it is important that these are incorporated into the classification of disease and, indeed, this is the case with the new classification. It is outside of the remit of this article to go into detail about risk factors, but examples include, poorly controlled type 2 diabetes, a family history of periodontal disease and smoking, amongst others. Any specific risk factors are included as the final part of the diagnostic statement. (Figure 2).
The BSP has developed a flow diagram based on the implementation of the 2017 Classification of Periodontal disease to help support practitioners in using the New Classification. This is available to download from www.bsperio.org, and is presented in Figure 1.
What additional clinical information is required in applying the New Classification?
One of the important aspects of implementing a new classification is to try and ensure that it is as easy as possible to use in general practice, where around 95% of periodontal treatment takes place. As can be seen, the New Classification is a significant departure from the 1999 system but, at a practical level, requires little additional information to classify disease. The key components are ‘Risk Assessment’, ‘Basic Periodontal Examination’ and ‘Radiographic Assessment’, all of which are part of a routine patient assessment. There are two pieces of additional information required: 1. Evidence of interdental recession; and 2. Full mouth bleeding on probing.
Evidence of interdental recession is easily identified during the clinical examination and BOP can be assessed during the BPE examination for BPE Codes 0, 1, 2 and 3, as full mouth probing is required to locate a Code 4. If a Code 4 is identified, then BOP forms part of the routine baseline indices required in patient management. So, in practical terms, this should not impact too heavily on patient assessment.
Clinical cases
In order to illustrate how this New Classification should be utilized in clinical practice, this will be applied to two clinical cases (see Case 1 and Case 2).
History
70-year-old male, regular attenderPoorly controlled diabetic, never smokerManual brushes x2/day, no interdental cleaningPrevious tooth loss due to periodontal diseasePoorly controlled type 2 diabetic
Examination
Plaque score 20%BOP <10% of sitesObvious interdental recession affecting 80% of teethBPE−/2/−2*/2/2*
Radiograph
No radiographs indicated (based on BPE Code 2) or available
Radiographs not available but, based on estimation of bone level – 8 mm recession (worst site interproximal recession) + 2 mm probing pocket depth + 2 mm biological width = 12 mm bone loss from CEJ. Average root length 15 mm, so apical third bone loss (also equates to approx 80% bone loss)
Extent
LocalizedGeneralizedMolar-Incisor
>30% of teeth affected
Grading
Slow
Moderate
Rapid
Maximum bone loss in this 70-year-old is 80% (determined by calculation above) 80% bone loss ÷ 70 years old = >1.0 and so rapid rate of progression
Disease Status
StableRemissionUnstable
Probing pocket depths 2 mm and less than 10% sites BOP
Risk Factors
Poorly controlled diabetes
Generalized periodontitis, Stage 4, Grade C, currently stable, unstable diabetic
History
30-year-old female, symptomatic attenderPregnant with no other relevant medical history, never smokerManual brushes x1/dayPrevious loss of teeth due to excessive mobility
Examination
Poor oral hygienePlaque score 70%BOP 80%Obvious loss of interdental papillaeBPE4*/4/4*4*/4/4*All teeth with pocket depths >5 mm
Radiograph
Supplied by referring practitionerNo other radiographs taken − patient pregnant
Radiograph of the worst site is showing bone loss into the apical third (and in some cases to the apices)
Extent
LocalizedGeneralizedMolar-Incisor
>30% of teeth affected
Grading
Slow
Moderate
Rapid
Bone loss in this 30-year-old is in excess of 90% in some areas = Grading ration of 3 (90/30) − which is >1.0 and so rapid rate of progression
DiseaseStatus
StableRemissionUnstable
Probing pocket depths >5 mm
Risk Factors
No specific risk factors identified
Generalized periodontitis, Stage 4, Grade C, currently unstable, no specific risk factors
These two cases help to illustrate how the New Classification should be implemented using the BSP implementation plan. These two cases result in a similar diagnosis one of which is currently stable with a Code 2 BPE the other being unstable. As previously indicated with the old classification, the first patient would have been classified as chronic gingivitis. There would have been no indication of the history of severe disease that this patient has experienced and the potential for relapse, especially in view of the unstable diabetes. This case obviously needs careful maintenance and this is clearly highlighted in the New Classification system.
Discussion
The key to successful management of periodontal disease is early detection of disease and instigation of suitable management regimens. The gateway to diagnosing disease is accurate utilization of the BPE examination. This article summarizes the importance and interpretation of this essential gateway examination and how it relates to the New 2017 Classification.
The New Classification has been developed based on current literature and a better understanding of the natural history of periodontal disease. It is a significant change from the 1999 scheme but offers a more detailed approach that gives detail of the patient's current disease exposure and rate of progression, both important features in determining prognosis and management strategies. As illustrated, it is able to capture historic disease that, although may be currently stable, such cases are at higher risk of future disease progression. The New Classification also offers future proofing, so it is envisaged that future modifications will not require major changes from the 2017 system set out in this article. The ramifications of a change in the classification system for any disease are significant and periodontal disease is no exception. Since 2017, great effort has been expended by the BSP, and its associated clinicians, teachers and researchers to ensure that patient management remains optimal and that the potential negative impact caused by any change is overcome by efforts to communicate the change in a clear and effective way. In this manner, the New Classification system provides a positive step forward. This paper aspires to add a further piece of the ‘communication jigsaw’ to the profession and no doubt further publications will follow. Indeed, during the preparation of this paper, further toolkits have been published by the European Federation of Periodontology, which the authors would encourage this readership to review, thereby further assisting clinicians in their management of periodontal diseases.13