Bouquot JE, Gundlach KKH. Oral exophytic lesions in 23,616 white Americans over 35 years of age. Oral Surg. 1986; 62:(3)284-291
Katsikeris N, Kakarantza-Angelopoulou E, Angelopoulos AP. Peripheral giant cell granuloma: clinicopathologic study of 224 new cases and review of 956 reported cases. Int J Oral Maxillofac Surg. 1988; 17:(2)94-99
Priddy RW. Inflammatory hyperplasias of the oral mucosa. J Can Dent Assoc. 1992; 58:(4)311-321
Pindborg JJ, Kramer IRH, Torloni H. Histological typing of odontogenic tumors, jaw cysts and allied lesions.Geneva: World Health Organization;
Moriconi ES, Popovich LD. Alveolar pyogenic granuloma: review and report of a case. Laryngoscope. 1984; 94:(6)807-809
Vilmann A, Vilmann P, Vilmann H. Pyogenic granuloma: evaluation of oral conditions. Br J Oral Maxillofac Surg. 1986; 24:(5)376-382
Hullihen P. Case of aneurism by anastomosis of the superior maxillae. Am J Dent Sci. 1844; 4:160-162
Recurrent exophytic growth on maxillary posterior edentulous alveolar ridge – a diagnostic challenge Aditya Patney Amar A Sholapurkar Keerthilatha M Pai Monica C Solomon Dental Update 2024 39:4, 707-709.
Authors
AdityaPatney
Consultant Oral Radiologist, Mahajan Imaging Centre, Hauz Khas Enclave, New Delhi – 110016, India
Assistant Professor, Department of Oral Medicine and Radiology, College of Dentistry, King Khalid University, Gregor Abha, Kingdom of Saudi Arabia – 61471
Accurate diagnosis of recurrent intra-oral exophytic lesions require a thorough history, meticulous clinical examination and the experience of assessing these lesions, because they are not commonplace. Despite this, instituting the correct diagnosis tests the skills of an oral medicine expert. Therefore, the same is all the more challenging for a general practitioner who may encounter these lesions without any significant experience. The importance of diagnosing such lesions cannot be understated, as they may represent a myriad of conditions ranging from seemingly innocuous benign pathologic processes to much more sinister ones, like oral malignancy; occasionally some of these lesions may manifest atypically. Such atypical presentations may cloud the diagnostic process. Here a case uncharacteristic of the condition it represented is reported with the aim of increasing awareness of the diagnosis of such lesions.
Clinical Relevance: When a clinician comes across recurrent exophytic intra-oral lesions, he/she must be careful, and consider all conditions in the differential diagnosis.
Article
Recurrent intra-oral exophytic lesions are uncommon.1 Recurrence of a lesion may suggest that the aetiological factor has not been addressed and, therefore, successful management will demand a more accurate diagnosis. Sometimes, a benign inflammatory lesion may be erroneously diagnosed as a serious condition. The clinician must therefore be well aware of all the possibilities that can manifest commonly or atypically.
Clinical presentation
A 60-year-old male farmer reported to our department with the chief complaint of a growth in the posterior region of the left maxillary residual alveolar ridge of 1½ years' duration. The growth developed after spontaneous exfoliation of two teeth. It was painless and gradually increased in size. He consulted a local dentist a year previously, and complete excision was carried out (histopathological details were not available with the patient). He was apparently asymptomatic thereafter but the growth recurred 8 months later and gradually increased in size to attain the current dimensions. This time it was associated with sharp shooting pain on touching and during mastication. There was no history of bleeding or pus discharging from the growth. The medical and family histories were not contributory. The patient had been a heavy smoker for 30 years. General examination revealed the patient to be in good general health. Intra-oral examination revealed a 3 x 2 cm exophytic growth associated with the left maxillary posterior residual ridge corresponding to the region of missing UL6, UL7 and UL8 (Figure 1). The lesion extended more in the buccal aspect and blended with the mucosa of the ridge on the mesial and distal aspects. It had a distinctly dimorphic appearance; the inferior aspect being creamy white to pale yellow, the buccal and palatal aspects being predominantly red in colour, with visible superficial blood vessels and interspersed blanched areas, with 3–4 areas of ulceration on the buccal surface of the mass. On palpation, the lesion was pedunculated with a broad stalk. It was readily mobile and the inferior aspect was much firmer in consistency. The ulcerations were tender and bled on palpation, but the rest of the mass was not tender.
Figure 1. Exophytic growth (3 x 2 cm) associated with the left maxillary posterior residual ridge.
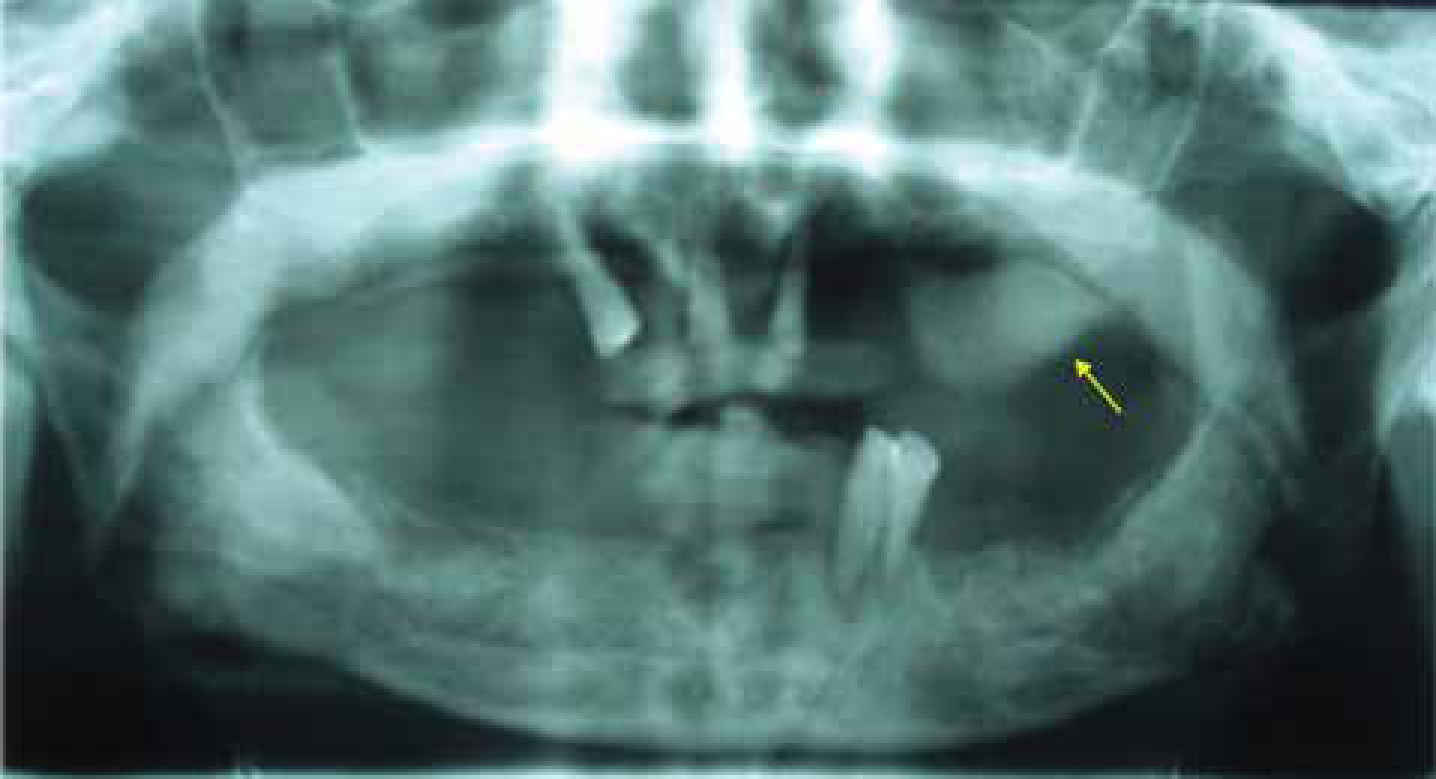
The panoramic radiograph demonstrated a well-defined, homogeneous and extra-osseous soft tissue radio-opacity measuring approximately 3 x 2 cm in the left maxillary posterior region (Figure 2). No embedded root stump or bony spicule was seen. A routine haemogram was advised and the findings were within normal limits.
Figure 2. Cropped panoramic radiograph demonstrating the soft tissue radio-opacity associated with the left maxillary posterior region.
Differential diagnosis
Considering the history of recurrence after excision, clinical presentation of the lesion, possible peripheral origin of the lesion and no radiographic evidence of bone loss, our differential diagnosis focused on benign inflammatory conditions including irritational fibrous hyperplasia, peripheral giant cell granuloma and peripheral odontogenic fibroma. Lastly, oral malignancy was not ruled out bearing in mind the patient's age, smoking habit and the history of recurrence after excision.
Irritational fibrous hyperplasias are the healed end products of inflammatory hyperplastic lesions. They were reported to be the second most common oral exophytic lesions in a large study.1 Usually, these lesions are sessile or pedunculated with a smooth contour, appear pale pink and are firm in consistency. They commonly occur on gingiva, tongue, buccal mucosa and palate with an asymptomatic presentation. Radiographic evidence of calcifications within these lesions is not uncommon. In the present case, no irritating factor could be established to consider irritational fibrous hyperplasia as the diagnosis. Also, the site of occurrence was not in favour for the same. Nonetheless, considering the clinical presentation of the lesion and the history of recurrence (which suggested a latent chronic irritational factor), irritational fibrous hyperplasia was the authors' first differential diagnosis.
Peripheral giant cell granuloma is an unusual proliferative response of the tissues to trauma and/or injury, which may be a result of tooth extraction, denture irritation or chronic infection. Gingival or alveolar process, mostly the mandibular premolar-molar region, is the most common site.2 These lesions have a female predilection and usually occur in the age group of 30–70 years. They appear as sessile or pedunculated growths which arise from deeper tissues with the risk of recurrence on excision. They are characterized by the presence of multinucleated giant cells whose origin is yet undetermined.3 All these features, except for the site of occurrence, were in agreement with our case. However, the lesions of peripheral giant cell granuloma are usually dark red, haemorrhagic and rarely exceed 2 cm in size. The radiographic features usually show peripheral cuffing. These features differentiated our case from peripheral giant cell granuloma.
Peripheral odontogenic fibroma has been defined by the World Health Organization (WHO) as ‘a fibroblastic neoplasm containing varying amounts of odontogenic epithelium. It may contain dentine and/or material resembling cementum.’4 It is a benign neoplasm with limited growth potential and has a predilection for attached gingiva, occurring most commonly on the maxillary anterior and mandibular cuspid-premolar regions. The lesion has a diverse distribution in the various age groups, but most cases appear to occur around the third decade without any gender predilection. The lesion commonly manifests as a slow growing mass that may be sessile or pedunculated, red or pink with a smooth surface and, in some cases, the overlying mucosa may be ulcerated. The lesion is usually firm in consistency, non-tender and occasionally causes displacement of associated teeth. These aspects were similar to our case.
Oral malignancy is also not uncommon in the elderly age group in Indian subpopulations with a strong risk factor of smoking. However, the patient was in good general health and there was no clinical indication of invasion or aggressive growth of the lesion. But, considering the chronic duration and recurrence, the possibility of oral malignancy was also considered in our differential diagnoses.
Diagnosis and management
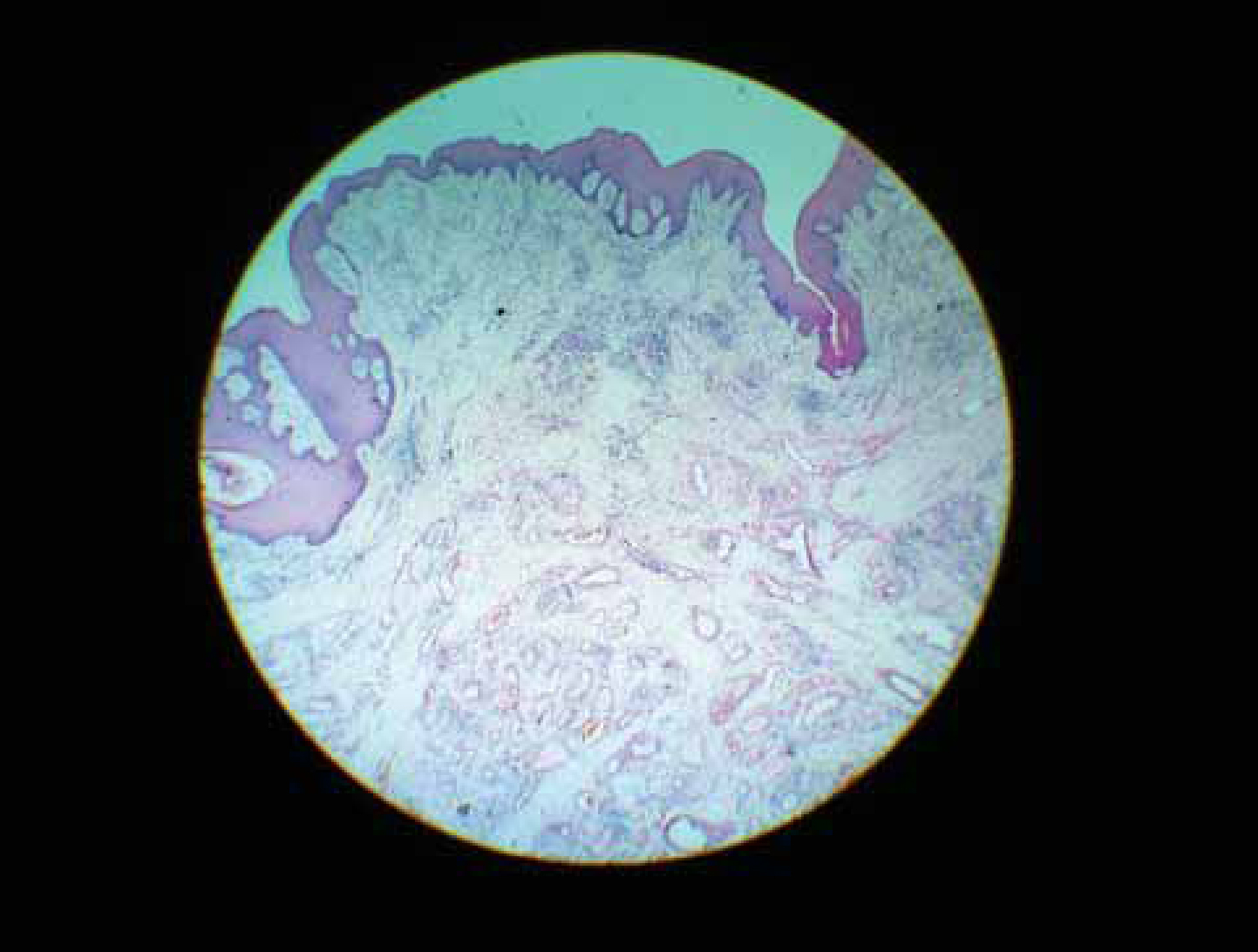
The patient was advised to stop smoking. An incisional biopsy of the lesion was done under local anesthesia. The Haematoxylin and Eosin sections (Figure 3) revealed a highly cellular connective tissue stroma composed of abundant dilated capillaries, proliferating endothelial cells and marked infiltration of lymphocytes, plasma cells and neutrophils. Overlying epithelium was parakeratinized, stratified squamous epithelium with extensive surface ulcerations. The ulcerated areas were covered with fibrinous exudate. These features were consistent with the diagnosis of pyogenic granuloma. The condition and its prognosis were explained to the patient and the lesion was excised uneventfully with a thorough curettage of the surgical site. Moderate bleeding was encountered, which was satisfactorily arrested. The post-operative period was uneventful and the patient has been on regular follow-up for the past 8 months with no recurrence.
Figure 3. Haematoxylin and Eosin sections of the lesion at 40x magnification, showing the parakeratinized epithelium with surface ulcerations and highly cellular connective tissue stroma.
Discussion
To the best of our knowledge, only one case of pyogenic granuloma of the alveolar ridge has been reported in the literature,5 by Moriconi and Popowich in 1984.
Pyogenic granuloma is a common tumour-like growth of the oral cavity that is considered to be non-neoplastic in nature.6 Hullihen's description7 in 1844 was probably the first case reported, but the term ‘pyogenic granuloma’ or ‘granuloma pyogenicum’ was introduced by Hartzell8 in 1904. The other synonyms include vascular epulis, benign vascular tumour, haemangiomatosis granuloma, epulis teleangiectaticum granulomatosa, and lobular capillary haemangioma. The name pyogenic granuloma is a misnomer since the condition is not associated with pus and does not represent a granuloma histologically.
It is commonly considered to arise in response to certain factors like chronic low grade irritation, hormonal disturbances, traumatic injury, certain drugs, or iatrogenic dental stimulation.9 Pyogenic granuloma may occur at all ages, but more frequently in the second decade of life, especially in young females, presumably due to the vascular effects of female hormones.
In the oral cavity, pyogenic granuloma shows a strong predilection for the facial gingiva in the maxillary anterior region, with interdental papillae being the most common site in 70% of the cases. The distinctive clinical manifestation of pyogenic granuloma is a small, deep red to reddish-purple lesion on the gingiva, which may be either sessile or pedunculated. The surface may be smooth, lobulated or occasionally warty, and shows a tendency to bleed either spontaneously or upon the mildest provocation. The lesion is painless and soft in consistency, although older lesions may become more collagenized and firm. The size of the lesion varies from a few millimetres to several centimetres and rarely exceeds 2.5 cm.10 In our case, several anomalous features were seen contrary to the characteristic features of pyogenic granuloma: the old age of the patient, no bleeding reported or evidenced from the lesion, extremely uncommon location and the clinical presentation of the lesion which was primarily firm and fibrotic. Hence, a clinical differential diagnosis of pyogenic granuloma was not considered.
In the only other reported case of pyogenic granuloma of the alveolar ridge,5 the panoramic radiographic examination disclosed a retained root stump in the substance of the soft tissue density of the lesion, which might have suggested a chronic irritant aetiological factor. However, in this case, no clinical or radiographic evidence of any irritant factor could be established.
Radiographic and histopathological investigations are crucial for confirming the diagnosis. Radiographs are advised to rule out osteolysis indicative of malignancy or to delineate a foreign object or sharp restorative margin that would need to be removed with the lesion. All lesions giving a clinical impression of pyogenic granuloma must be biopsied to rule out the aforementioned pathologic entities.
Excisional biopsy is indicated for treatment, except when it would produce a deformity, in which case, an incisional biopsy is mandatory.11 A recurrence rate of 15% has been noted after surgical excision.12 After surgical excision of gingival lesions, curettage of underlying tissue is recommended. Recurrences after surgery for extragingival pyogenic granulomas are, however, uncommon.13