
References
Oral and dental management for people with lymphoma
From Volume 46, Issue 2, February 2019 | Pages 133-150
Article

This paper offers a literature review that describes the recommended oral and dental management for people with lymphoma. From 1980 to 2017, the electronic databases, PubMed, Scopus and Google Scholar, were searched using the following keywords: lymphoma, treatment of lymphoma, monoclonal antibodies, medication-related osteonecrosis of the jaw, thrombocytopenia in relation to chemotherapy, neutropenia in relation to chemotherapy, antibiotic prophylactics, lymphoma and chemotherapy, radiotherapy and lymphoma. The search included both in vivo and in vitro studies published in the English language. The main inclusion criteria were any studies described ‘lymphoma’, ‘types of lymphoma’, ‘treatment of lymphoma’, ‘aetiology and physiology of lymphoma’, and ‘dental management of patients with lymphoma’.
Lymphoma
Lymphoma is a solid neoplasm that arises in lymphoid tissues and spreads to distant lymphoid glands and organs.1 It occurs when abnormal lymphocytes increase in number without proper control. They divide in an abnormal pathway or do not die when they should. In 2015, the Office for National Statistics (ONS) reported that non-Hodgkin's lymphoma affected 11,690 patients, while Hodgkin's lymphoma affected 1,782 patients.2 However, in 2016, these incidences were increased to nearly 17,000 and 2,000 cases diagnosed with non-Hodgkin's lymphoma and Hodgkin's lymphoma, respectively.3 It affects any age, including children. Currently, it is mostly treatable, and people live for many years after being diagnosed.
Pathophysiology of lymphoma
Functional lymphocytes circulate the body in the lymphatic system as a part of the immune system. This lymphatic system includes lymphatic glands such as axillary and inguinal lymph nodes and also includes lymphatic organs (extranodal) such as thymus, spleen, lungs, liver and bone marrow. In the case of lymphoma, proliferated abnormal lymphocytes collect in the lymphatic glands and organs with variant signs and symptoms based on the affected glands and/or organs.
Aetiology
In many cases, the cause of lymphoma is unknown. However, people who have a medical condition that affects their immune system have a predisposition to develop lymphoma. For example, after starting the highly active antiretroviral therapy (HAART) for human immunodeficiency virus (HIV), patients with insufficient immunologic responses are at highest risk of non-Hodgkin's lymphoma (NHL).4 Solid organ transplantation and the associated immunodepression is a risk factor for lymphoma.5 Patients with Sjögren's syndrome (an autoimmune disorder) are at increased risk of developing NHL, and mainly mucosa-associated lymphoid tissue lymphoma.6 One study found that 5% of people diagnosed with Sjögren's syndrome develop lymphoma.1 Studies show that lymphoma does not run in families and does not have a genetic predilection.3 Additionally, viral infection with Epstein-Barr virus7 and bacterial infection with Helicobacter pylori are linked to specific types of lymphoma affecting the gastric mucosa.
Diagnosis and investigation
A thorough medical history accompanied by examination and investigation of a swollen lymph node is usually the first step taken by the physician. However, some suggest waiting for a few weeks prior to further investigations as enlarged lymph nodes with lymphoma-like symptoms are commonly seen in other less severe conditions, such as viral or bacterial infection. Clinically, it is not easy to differentiate between reactive nodes or metastatic nodes secondary to malignancy. Reactive (infectious) lymph nodes are soft, tender, fluctuant and with overlying erythema. However, firm, non-tender, fixed lymph nodes for more than two weeks are possible clinical findings for malignancy.
Further investigation includes fine needle aspiration (cytology)8 and full blood count as the red blood cells, platelets, other white blood cells (ie low level of neutrophils) will be low if lymphoma has spread to the bone marrow. Other tests to assist diagnosis are computed tomography (CT) scans, fluorodeoxyglucose positron-emission tomography (FDG PET),9 whole-body magnetic resonance imaging (WB-MRI) and ultrasound scans.10 Bone marrow biopsy from the iliac bone detects bone marrow involvement but does not add diagnostic value alone, especially in the early stages of lymphoma.11 Once lymphoma is diagnosed, the site and stage is used to decide the treatment modality.
Types of lymphoma
There are two main types of lymphoma: Hodgkin's lymphoma (HL) and non-Hodgkin's lymphoma (NHL), which require histopathology to confirm the definitive diagnosis.12 Most types of lymphoma have the same signs and symptoms of non-tender swollen lymph nodes, fever, night sweats and unexplained weight loss.13
Dr Thomas Hodgkin first described Hodgkin's lymphoma in 1832.14 It develops from B-cell lymphocytes. Reed-Sternberg cells (large bi-nuclear cells) are seen histologically and confirm the diagnosis of HL,15, 16 while they are absent in NHL. The Revised European-American classification system recognizes two main types of Hodgkin's lymphoma: classical types and nodular lymphocyte-predominant types (Table 1). The types of classical HL are named after the different appearances of the lymphoma cells and the cells in the tissue surrounding them. The Ann Arbor staging system is used to stage Hodgkin's lymphoma (Table 2). On the other hand, non-Hodgkin's lymphoma is classified by the types of lymphocyte, either B-lymphocyte (major type) or T-lymphocyte. However, it is the behaviour of a non-Hodgkin (low grade or high grade) that will determine the treatment (Table 3). To some extent, both types of lymphoma have the same medical management and approaches.
| Types | Classification |
|---|---|
| I. Classical Hodgkin's lymphoma (main type of Hodgkin's lymphoma) |
|
|
|
|
|
|
|
|
|
|
| II. Nodular lymphocyte-predominant Hodgkin's lymphoma (NLPHL) |
|
| Stage | Description |
|---|---|
| Stage I |
|
| Stage II |
|
| Stage III |
|
| Stage IV |
|
| I. Low-grade lymphoma (indolent lymphoma): in this type the cells appear to be dividing slowly. Some patients do not require early treatment, but they need a regular monitoring until treatment is needed and this is called the ‘watch and wait’ approach |
|
| II. High-grade lymphoma (aggressive lymphoma): in this type the cells appear to be dividing quickly |
B-cell high grade non-Hodgkin's lymphomas
|
|
T-cell high grade non-Hodgkin's lymphomas
|
Treatment of lymphoma
Treatment depends on the type and stage of lymphoma, signs and symptoms of the disease, availability of treatment, and the age and general health of the patient. The main aim of treatment is to achieve complete remission from the lymphoma.17 Different types of lymphoma respond differently, and therefore a variety of treatment options is necessary. Hodgkin's lymphoma responds well to chemotherapeutic agents.17 On the other hand, low-grade non-Hodgkin's lymphoma is considered to be one of the most radiosensitive tumours,18, 19 therefore it is usually treated with a low dose of radiotherapy (typically 36.6 Gray).20 Chemotherapy can also be added during the treatment of high-grade NHL. In both types of lymphoma, monoclonal antibodies may be added to chemotherapy cycles and can also be used for radioimmunotherapy. Other types of treatments might be considered, which will be detailed later in the paper.
Treatment types
The main treatment modalities for patients with lymphoma are:
Monoclonal antibodies (MABs)
Monoclonal antibodies (MABs) or biological agents/targeted drug therapy are antibodies/agents that are developed identical to immune cells. They work by finding specific proteins on cancer cells. Treatment of lymphoma with antibody therapy (immunotherapy/targeted therapy) targets an antigen on the lymphoma cells.21 It works by either binding to the antigen CD20 (an activated-glycosylated phosphoprotein expressed on B-cells which helps to identify it) or by activating the immune system to damage the cancer cells. For example, rituximab (MabThera®),22 ofatumumab (Arzerra®),23 and obinutuzumab (Gazyvaro®)24 are anti-CD20 agents. Pembrolizumab (Keytruda®) and nivolumab (Opdivo®) stimulate the body's immune system and block a protein called PD-1 on the surface of T-cells to target and kill cancer cells.25 Monoclonal antibodies may be added to chemotherapy cycles to help sensitize the cancer cells to the chemotherapeutic agents. They can also be used for radioimmunotherapy,21 such as 90Y-ibritumomab tiuxetan (Zevalin®), to help target the radiotherapy to abnormal cells. Use of MABs reduces the side-effects that arise from conventional radiotherapy and chemotherapy.
Rituximab (MabThera®) is commonly used for the treatment of B-cell lymphoma.21 It does not affect T-lymphocytes as it only binds to CD20 on B-lymphocytes. It can also be used in maintenance therapy during the remission phase of lymphoma,26 where it is typically given every two to three months for a period of two-years.27 Currently, there are many monoclonal antibodies in clinical trials aiming to target lymphoma cells and reduce adverse effects to normal cells.27
Dental recommendations: A dental assessment by the general dental practitioner (GDP) prior to starting a monoclonal antibody (generally rituximab) therapy is recommended to ensure that they are dentally fit prior to starting lymphoma treatment. This may involve extraction of infected or unrestorable teeth, or teeth with advanced periodontal disease. This should be carried out as soon as possible, and in liaison with a special care dentist or oral surgeon and the haemato-oncologist.
It is rare for patients who are being treated with rituximab to develop medication-related osteonecrosis of the jaw (MRONJ), however it has been reported in the literature. In 2017, a case report of MRONJ (stage III) has been reported in a 52-year-old female diagnosed with NHL who had been treated with rituximab and prednisone.28 Another paper reported a 69-year-old male kidney transplant recipient who presented with MRONJ 5 years post-transplantation.29 The patient presented with an oral ulcer related to post-transplantation lymphoproliferative disorder, which was treated with rituximab; subsequently, osteonecrosis of the jaw developed. There may be an association but causality cannot be proven on the basis of two case reports. It is important to explain to patients that the risk of (MRONJ) is very low and they should not be discouraged from taking their medication or avoid receiving dental treatment.30 Ideally, a written information sheet that includes the definition of MRONJ, signs and symptoms, incidence, risk factors and preventive advice should be given.31Table 4 presents the three advanced stages of MRONJ.
| MRONJ Staging | Description | Recommended Treatment |
|---|---|---|
| Patients at risk of developing MRONJ | Patients who have been treated with anti-resorptive and/or anti-angiogenic and/or anti-neoplastic medication, but no evidence of exposed necrotic bone of symptoms of pain or non-specific clinical findings |
|
| Stage 0 | Patients present with non-specific clinical symptoms and radiographic changes, but no apparent necrotic bone |
|
| Stage 1 | Asymptomatic exposed necrotic bone, or fistulae, that probes to bone without any signs of infection |
|
| Stage 2 | Symptomatic exposed necrotic bone, or fistulae that probes to bone without any signs of infection |
|
| Stage 3 | Exposed necrotic bone extending beyond the region of alveolar bone or with pathological fracture |
|
Chemotherapy
Lymphomas are relatively sensitive to chemotherapy. Chemotherapeutic agents destroy rapidly dividing cancer cells but work non-specifically and damage normal rapidly dividing cells such as in the bone marrow. These include white blood cells (WBCs), red blood cells (RBCs) and platelets (Table 5).32
| Type of Progenitor Cells | Type of Cells |
|---|---|
| I. Erythroid progenitor cells |
|
| II. Lymphoid progenitor cells |
|
| III. Myeloid progenitor cells |
|
The type of chemotherapy regimen depends on several factors, such as the type of lymphoma, location of lymphoma in the body, age of the patient and the general health and fitness of the patients. For older patients, a conservative (low doses) and straightforward approach is usually the first choice; while younger patients receive a less conservative plan (higher doses) to prepare them for a haematopoietic stem cell transplant (HSCT). The most common chemotherapy regimens used are ABVD (doxorubicin (Adriamycin®), bleomycin, vinblastine and dacarbazine), BEACOPP (bleomycin, etoposide, doxorubicin (Adriamycin©), cyclophosphamide, vincristine (Oncovin®), procarbazine and prednisolone, and CHOP (cyclophosphamide, doxorubicin (or hydroxydaunorubicin), vincristine (Oncovin®) and prednisolone. A monoclonal antibody could be added to the chemotherapy regimen, such as rituximab (MabThera®). In such cases, an ‘R’ is added to the name (ie R-CHOP).27Table 6 presents common side-effects of chemotherapy regimens with some dental considerations.
| Common Side-effects of Chemotherapy Regimens | Dental Considerations |
|---|---|
| Bruising and prolonged bleeding | Patients may be on a daily dose of low weigh molecular heparin (LWMH) injection to reduce risk of deep vein thrombosis (DVT). Therefore, liaison with the patient haemato-oncology team is recommended prior to invasive dental treatment1 |
| Vomiting or nausea | Postpone dental treatment if necessary. Severe vomiting can lead to tooth wear |
| Generalized fatigue, frequent headache, flu-like symptoms and tiredness | Dental team should ensure that the patient is well on day of the treatment and consider postponing if necessary |
| Brown marking on the skin, hair loss, brittle and chipped nails | If patient shaved or lost hair during chemotherapy, they may be wearing a wig, scarf or hat. It is important to be sensitive to this and ensure that patient is not asked to remove any hat/scarf unless absolutely necessary |
| Feeling very cold and tingling hands or feet | Use of blankets and warm water for hands if cannulation is necessary, eg for treatment under sedation |
| Conjunctivitis, blurred vision and photosensitivity | Dental team should adjust dental chair's light carefully and avoid light shining directly on patient's eyes. Some new dental chairs can reduce light brightness. Consider use of accessible information such as large print for patients with visual impairment. Ensure patient can read consent forms, dental information sheets |
| Raise in blood uric acid | High level of uric acid in the blood increases risk of gout, which can affect fingers and joints. If this effects patient's manual dexterity and ability to carry out good oral hygiene, simple adjustments may help, such as using silicon-based material or a rubber ball to amend the patient's toothbrush handle. Alternatively, some patients may find an electric toothbrush easier to use |
| Altered kidney and liver functions | Drug metabolism is affected. For example, a sedative drug (ie midazolam) may produce exaggerated effects due to increased levels of free drug.2 Dental team should be aware that drug metabolism may be slow and recovery prolonged because of altered kidney function. Additionally, due to liver damage, the patient could be anaemic, conscious sedation should not usually be carried out when the haemoglobin level is less than 10g/dL.3 Liver damage can also lead to problems with clotting and therefore risk of prolonged bleeding |
| Breathless, inflammation of the lung and damage of the heart muscle in some patients | Liaison with the haemato-oncology team prior to dental treatment and especially treatment under conscious sedation to check patient's cardiorespiratory function |
Dental recommendations: Normally, 6 cycles are administered every 3 weeks continuously, but can vary from patient to patient. For example, one cycle may start in the first week of the month, and then the patient will have a rest period of 3 weeks prior to starting the second cycle (first week of the following month). The lifespan of platelets is 10 days, while the lifespan for white blood cells is 4 weeks.33 If pre-treatment extractions have not been possible, any necessary extractions should be planned in liaison with a patient's haemato-oncologist to determine the right time so as to reduce the risk of infection and aid haemostasis.33 It is important to ensure that there is sufficient time post-extraction (typically 10−14 days) to allow adequate healing prior to the next cycle of chemotherapy. Therefore, if the extraction is not urgent, it would be better to wait until after chemotherapy cycles are complete, and manage any dental infection through pulp extirpation and/or antibiotics.
Dental extractions or regional block injection (ie inferior alveolar nerve block) should be avoided for patients with platelet counts below 50 x 109/L and 30 x 109/L, respectively.1 GDPs should liaise with the haemato-oncologist prior to any invasive procedure to check the platelet counts. Patients with platelet counts below 50 x 109/L requiring any minor oral surgery, such as extractions, will need platelet transfusions to be organized via the haemato-oncology team.1 One unit of platelets should raise the count by around 10 x 109/L. Platelets can last up to a week post-transfusion but, in cancer patients, they may be broken down quickly. Therefore, ideally, dental treatment should be carried out within 24 hours from when the platelet transfusion has been given. A post-transfusion blood test is recommended to check that the platelets are at the required level as some patients do not increment as well as others. Table 7 describes the management of patients at different levels of thrombocytopenia undergoing dental treatment. Local haemostatic measures are recommended, such as the use of haemostatic agents (Surgicel®) suturing the socket, as well as written and verbal post-operative instructions and the provision of an emergency contact.33
| Platelets Counts | Dental Considerations |
|---|---|
| <30 x 109/L |
|
| 30–50 x 109/L |
|
| >50 x 109/L |
|
Scully et al recommend antibiotic prophylaxis for patients with neutrophil counts below 2 x 109/L to reduce possible septicaemia.1 The haemato-oncologist may also advise granulocyte colony-stimulating factor (G-CSF) prior to dental procedures. G-CSF is a glycoprotein that stimulates the bone marrow to produce granulocytes and stem cells and release them into the bloodstream.34, 35 Subcutaneous or intravenous administration of G-CSF 0.5 x 106 units/kg/day over 3−5 days has been recommended.1 However, after two days from the last dose of G-CSF, there is a significant reduction in the circulating neutrophils and it takes up to 7 days to reach optimal level of neutrophil counts. Therefore, one week after the last dose of G-CSF is usually the most appropriate time for dental treatment. This decision is made in liaison with the haemato-oncology team and full blood counts (FBCs) checked prior to invasive treatment to check response to G-CSF.1
Management of invasive procedures other than extractions, such as scaling and root surface debridement (RSD), might increase bleeding episodes and therefore the dental team needs to liaise with haemato-oncology and obtain FBCs prior to treatment. Local application of tranexamic acid, if available, should be considered, the patient is asked to bite on gauze soaked in tranexamic acid for 15−20 minutes to act as a local antifibrinolytic agent.
In the event of needing conscious sedation, lymphoma patients require careful assessment as they could be anaemic; conscious sedation should not usually be carried out when the haemoglobin level is less than 10g/dL.36 The haemato-oncology team can help to raise the level of haemoglobin either by erythropoietin injection or blood plasma transfusion.
Chemotherapy-related mucositis is one of the most common complications following chemotherapy, affecting 50% of adults.1 It usually develops after 7−14 days and appears as a sloughing erythematous area. It affects mucosal areas, including oral mucosa and gastrointestinal tract, and can compromise oral intake. Ice-chips for 30 minutes prior to chemotherapy cycles can help reduce the severity of the developing mucositis (Figure 1).37 The haemato-oncology team may consider the use of biological response modifiers (cytokines or stimulating growth factors) prior to chemotherapy cycles to help reduce mucositis development.1

In general, dietitians, dentists and haemato-oncology teams advise patients to follow a soft diet and avoid rough and spicy food, acidic fruit and salt. In severe cases, tube feeding may have to be considered. It is important to discuss avoiding smoking and alcohol as this can increase the severity of mucositis. Where good oral hygiene is difficult to maintain due to mucositis, a soft toothbrush or sponge toothbrush with alcohol-free mouthrinse can be used.38 Topical gel (lidocaine) or 15% of benzydamine hydrochloride (15 ml three times per day during the chemotherapy cycles) may be prescribed to reduce discomfort and pain.
Oral infections can present more commonly in patients on chemotherapy due to their immunosuppressed state. To prevent fungal infections (eg oral candidiasis), topical anti-fungal agents (ie Nystatin suspension 100,000 U/ml) may be prescribed 4 times per day for 2 weeks.1 Viral infections are also common (mainly herpes simplex), and anti-viral agents may be prescribed (200 mg aciclovir three times per day).1 Both anti-viral and anti-fungal agents are usually prescribed by the haemato-oncology team as prophylaxis to reduce the development of candidal and viral infections.
Radiotherapy
Radiation therapy is defined as ‘the use of high-energy radiation from x-rays, gamma x-rays, protons, neutrons and other sources, which destroy cancer cells and reduce the size of the tumour'.39 The effects of radiation are generated through direct damage to the nucleic part of any cell (DNA) or indirectly as a result of the interaction between the water and radiation (free radicals).40
Radiation is used significantly in the treatment of patients with lymphoma, particularly in early and advanced stages of HL, NLPHL, high grade NHL and occasionally with low-grade types of NHL. These types of lymphoma are very sensitive to radiation. Two types of radiotherapy are considered: involved-field radiotherapy (IFRT) and involved-node radiotherapy (INRT).41 Radiotherapy to a lymphoma in the head and neck region is usually a much lower volume than that used for other cancers in this region (typically 36.6.Gray).
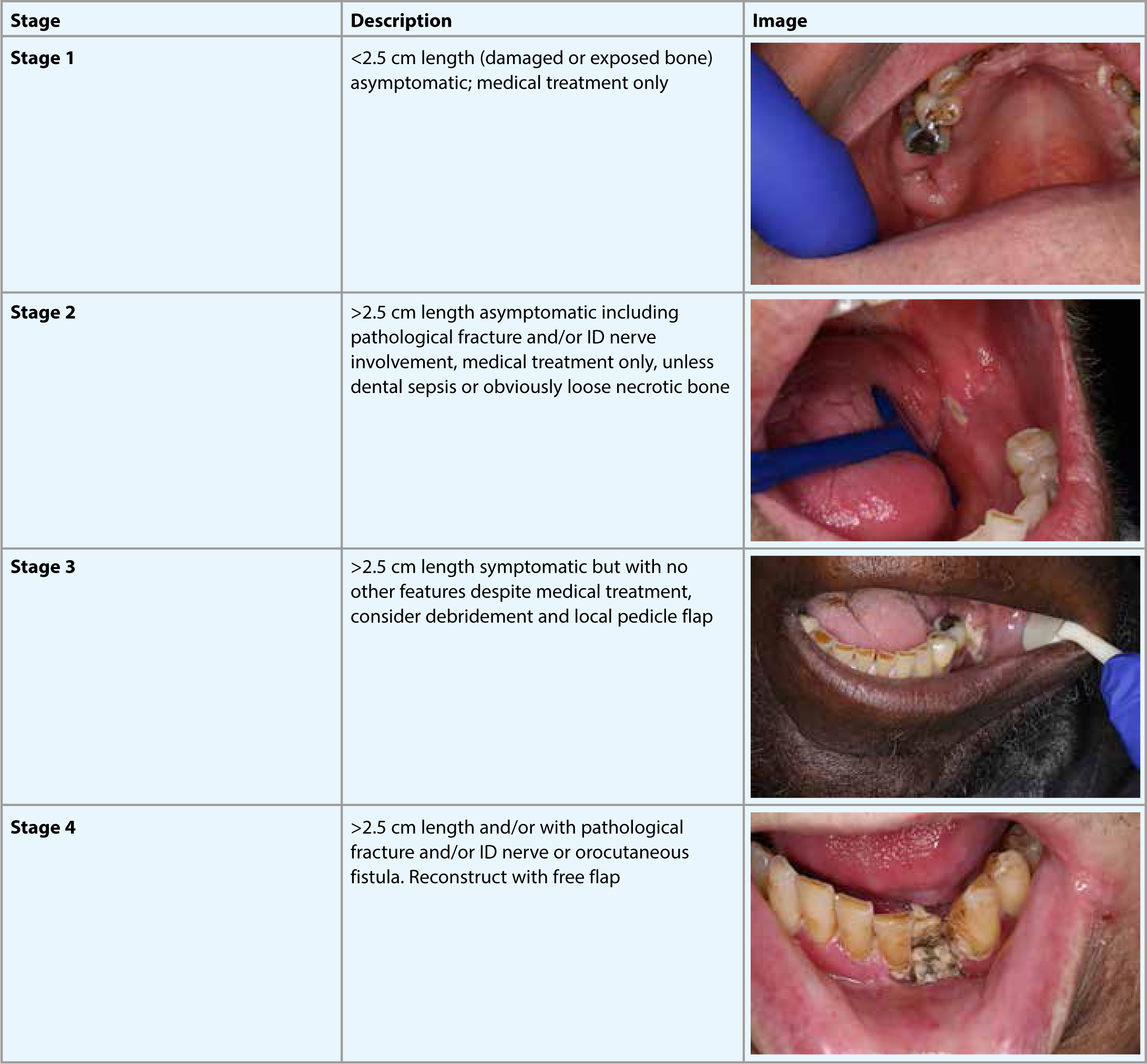
Dental recommendations: The toxic effects of radiotherapy increase with volume of the radiation and are dependent upon the field irradiated.42 Unfortunately, ionizing radiation has the ability to damage many parts of the body's cells. The toxicity-associated effects of radiotherapy could be divided into early forms toxicity, such as mucositis, taste disturbance, xerostomia and trismus, or late forms of toxicity, such as irradiation caries and osteoradionecrosis (ORN).
Since radiotherapy volumes are lower for lymphoma (typically 36.6 Gray) than that for other head and neck cancers, the side-effects are generally less severe. Instead, patients are expected to have mild acute side-effects, such as dry mouth, mucositis and loss of taste, with low risk of developing ORN (Figure 2).43 It is advisable that patients have a pre-treatment dental assessment similar to patients with other head and neck cancers receiving higher doses of radiation.
The aim of this assessment is to eliminate any foci of infection, extract poor prognosis teeth, and carry out supragingival and subgingival scaling. The dental team may advise on management of dry mouth and mucositis. For dry mouth, patients could take sips of water frequently, and use sugar-free chewing gum to stimulate unaffected salivary cells.44 The natural mucin-based saliva substitute (AS Pharma Saliva Orthana) and Biotene® Oral Balance Moisturizing Gel or Spray (GlaxoSmith Kline, Brentford) could be prescribed to help reduce the feeling of dryness and lubricate the oral cavity.45 However, there is little evidence of its efficacy, and it is best for patients to try samples. Difflam (15% benzydamine oral rinse, 15 ml every 8 hours and up to 3 weeks post-radiotherapy treatment) is usually prescribed by the patient's haemato-oncology team and acts effectively as an analgesic and anti-inflammatory for oral mucositis.46
Corticosteroid
Synthetic corticosteroids, such as prednisolone, methylprednisolone, and dexamethasone, are used alone or as part of a lymphoma treatment regimen.47 They help by increasing the overall effectiveness of chemotherapy and therefore reducing the number of cycles needed and the negative side-effects. There are many reported side-effects to long-term use of corticosteroids, such as fluid retention (Cushing syndrome), reduced immunity, impaired healing, raised blood glucose and osteoporosis.48 Prescription of oral bisphosphonate (alendronic acid 70 mg − Fosamax®) is important to protect bone from the development of osteoporosis. It is one of most widely used bone modifying agents to reduce osteoclast function and protect bone.49 Additionally, longer-term adrenal insufficiency could lead to adrenal crisis during episodes of infection and stress, including dental treatment.
Dental recommendations: A serious oral complication can develop following treatment with bisphosphonate called bisphosphonate-related osteonecrosis of the jaw (BRONJ). Recently, the name BRONJ has been changed to medication-related osteonecrosis of the jaw (MRONJ) since now several drugs have been recognized as a cause of jaw necrosis.45, 46 The accurate incidence of BRONJ is still unknown.50 Studies show that there is a significant difference in developing MRONJ in patients prescribed oral bisphosphonate versus intravenous bisphosphonate for bone metastatic cancer; MRONJ mainly develops with intravenous bisphosphonate. Some medical reports have estimated the incidence of BRONJ to be 1 in 10,000 (for intravenous bisphosphonates) to 1 in 100,000 (for oral bisphosphonates) people per year's exposure.14, 15 Therefore, a dental assessment by the GDP prior to starting the therapy with a drug with a risk of MRONJ is recommended to ensure that patients are dentally fit. This may involve extraction of infected or unrestorable teeth, or teeth with advanced periodontal disease. This should be carried out as soon as possible, and in liaison with a special care dentist or oral surgeon and the haemato-oncologist.
Adrenocortical insufficiency is likely to develop if the patient has received daily doses of 10 mg or more of prednisolone (or equivalent) in the previous 3 months.1 Dental procedures can increase patient anxiety, which theoretically could lead to adrenal crisis. Steroid supplement is not recommended for non-invasive dental procedures (restorative treatment, root canal treatment, supragingival and subgingival scaling).51 For surgical dental procedures under local anaesthesia, steroid supplement is sometimes advised. A double dose of prednisolone or equivalent is recommended one hour before dental treatment, up to a maximum dose of 20 mg hydrocortisone (or equivalent glucocorticoid) or intravenous hydrocortisone may be given.51 However, steroid cover is assessed case by case and with liaison with a patient's haemato-oncology team. Table 8 describes the management of patients with a history of systemic corticosteroid therapy recommended by Gibson and Ferguson.52
| Amount of Steroid Taken by the Patients Within Three Months | Recommendations |
|---|---|
| <10 mg of prednisolone or equivalent |
|
| 10 mg−50 mg of prednisolone or equivalent |
|
Haematopoietic stem cell transplant
Haematopoietic stem cell transplant (HSCT) is selected as a part of lymphoma treatment for fit younger patients <65 years with good general health and also for people with relapsed or a refractory form of lymphoma.27 There are two types of stem cells transplant: autologous and allogeneic.53 For the autologous type, stem cells are collected from the affected patient, and the collected sample given back to the same patient after high-dose chemotherapy.53 In allogeneic stem cell transplants, patients receive donor stem cells after high-dose of chemotherapy. Patients receiving allogeneic stem cells have a higher risk of autoimmune rejection of the donor cells and developing graft-versus host disease (GVHD).54 The donor cells are best harvested from a close relative who is also HLA-matched as much as possible to reduce the risk of graft rejection.1 Most transplants are made between HLA identical siblings, first degree relative members, or matched volunteers.
Dental recommendations: Prior to haematopoietic stem cell transplant (HSCT), patients have reduced platelets and neutrophils due to a high dose of chemotherapy received in preparation for the transplant. This will increase the risk of bleeding episodes and infection.55 Therefore, pre-treatment dental assessment for patients undergoing HSCT is crucial to eliminate any foci of infection.56, 57 Extraction of teeth with poor prognosis and supragingival and subgingival scaling is recommended.58 Liaison with the haemato-oncology at this stage prior to dental treatment is important. A minimum of 10−14 days is recommended for healing after extraction prior to the start of chemotherapy to prevent serious infections while a patient is very immunocompromised.59 Patients with platelet counts below 50 x 109/L and neutrophil counts below 2 x 109/L may need pre-operative platelet transfusions and G-CSF plus antibiotic cover to prevent post-operative infections. These patients are better managed in a secondary care centre.
During the first six months following HSCT, elective dental treatment is not recommended. Where possible, urgent dental problems are better managed through tooth extirpation and/or antibiotics and should be carried out at a secondary care centre. Six months post-HSCT, patients can be discharged to primary care for routine follow-up and dental treatment. General dental practitioners are advised to consult with a patient's haemato-oncology team or general physician (GP) regarding platelet and neutrophil counts prior to invasive dental treatment.
Graft-versus-host disease (GVHD) is a severe complication following allogeneic HSCT. The acute form is a syndrome of dermatitis, painful rash, hepatitis, enteritis and bone marrow suppression leading to thrombocytopenia and haemolytic-anaemia.1 It develops soon post-HSCT (typically 100 days).60 Chronic graft-versus-host disease (cGVHD) (more than 100 days) is considered one of the most common late side-effects post-HSCT.58 It has a similar presentation to the acute form but with a less aggressive appearance. cGVHD usually develops after the acute form, however, it may develop alone. Haemato-oncology teams aim to treat the acute form of GVHD with an intravenous methotrexate for 14 days, while oral steroid (prednisone) with/without ciclosporin can be considered for the treatment of the chronic form.1 The pathophysiology of GVHD is explained by the body's low immunity developed by high doses of chemotherapy followed by the transferred lymphocytes that destroy the host's body tissues. Oral manifestations can range from mild signs, such as mouth dryness, lichenoid reaction, fungal and herpetic gingival infections, to severe forms, such as severe oral pain with a high possibility to develop squamous cell carcinoma.61, 62 The most frequent symptoms reported are dry mouth and pain on swallowing that may limit oral intake,59 and patients might require referral to the nutrition team.
Elective dental treatment should be avoided during the acute form; only antibiotics and analgesics are recommended. Patients with cGVHD can receive dental treatment in a hospital setting or primary care, depending on the severity of the GVHD. Liaison with the haemato-oncology team prior to dental treatment or conscious sedation is required to check blood levels and pulmonary function.
Patients with HSCT usually receive an immunosuppressive agent (ciclosporin or tacrolimus) in combination with steroids to reduce possible rejection of the donor cells and developing graft-versus-host disease (GVHD). Ciclosporin affects oral and dental health negatively and leads to gingival hyperplasia.19, 20 Gingival enlargement complicates oral hygiene, may lead to halitosis, and can also affect oral function. Genetic predilection,21 and the presence of plaque and calculus with poor oral hygiene will increase the risk of the development of ciclosporin-related gingival hyperplasia. Other studies found that tacrolimus has no adverse effects on the gingival tissues and may be considered as an alternative to ciclosporin, with minimal risk of allograft dysfunction or rejection.24, 25 Treatment of this type of gingival hyperplasia will require liaison with a patient's haemato-oncology consultant as it responds very well to medication dose adjustment. Severe cases of gingival enlargement may need a surgical gingivectomy. This will require a multidisciplinary approach with a periodontologist and the haemato-oncology team.
Post-HSCT, patients are more susceptible to oral infections similar to infections developed during chemotherapy and therefore may require prescription of anti-viral and anti-fungal agents. Ciclosporin and tacrolimus are sensitive to drug interaction with anti-fungal agents, and especially the azole group, which interact with cytochrome P450 enzymes and inhibit ciclosporin and tacrolimus metabolism, which will then increase the drug serum level.63 Although topical miconazole has been shown to be safe, the topical gel might be swallowed and enter the systemic circulation.64 Therefore, liaison with the haemato-oncology team or patient GP is necessary prior to prescribing antifungal or anti-viral agents. Frequent oral ulcers can be an indication of a high plasma concentration of ciclosporin or tacrolimus, and the haemato-oncology team should be informed.64
Discharge and follow-up
Ideally, after treatment for lymphoma, patients remain under the care of their GDP who is informed of the patient's medical history, medication, treatment received for lymphoma and radiation dose, if applicable. The importance of reviews every 3−6 months, with the provision of an intensive preventive programme, should be stressed. Although it is uncommon, a lesion in the oral mucosa or jaws (long-standing oral swelling, multifocal ulcers, spontaneous oral bleeding, pain without pathological findings and unexplained tooth mobility) could be indicative of a relapsing lymphoma.65, 66, 67 In most cases reported, presentation was in Waldeyer's ring.68, 69, 70, 71 Waldeyer's ring consists of the pharyngeal tonsils on the roof of the nasopharynx, tubal tonsil on each side, palatine tonsils in the oropharynx and lingual tonsils on the posterior part of the tongue.72 This ring acts as a first line of defence in the immune system against pathogens that enter the oropharynx routes. Therefore, any patients with suspicious oral lesions should be referred urgently to a specialist centre for early investigation and management.38 Six months post-HSCT, patients can receive dental treatment in primary care. HSCT patients are at high risk of developing oral squamous cell carcinoma.57, 73 Thereby, early referral is essential for any suspicious oral lesions.
The Lymphoma Association in the United Kingdom have developed a double-sided credit card size card with space for details of the responsible healthcare professionals which people diagnosed with lymphoma may like to carry for easy reference. It also has contact details for the Lymphoma Association on the back of the card for any further information (Figure 3).27Table 9 summarizes dental recommendations for people with pre-lymphoma treatment, during lymphoma treatment, pre-HSCT, post-HSCT, and post-lymphoma treatment long term.
| Type of Treatment | Dental Recommendations |
|---|---|
| Pre-lymphoma treatment assessment (pre-chemotherapy cycles, monoclonal antibodies and pre-radiotherapy) |
|
| During chemotherapy cycles or radiotherapy |
|
| Pre-HSCT treatment |
|
| Post-HSCT |
|
| Long-term follow-up |
|
Conclusion
A holistic approach is required to manage people with lymphoma. Following treatment of lymphoma, patients remain under the care of their GDPs. However, GDPs should always consider a ‘shared care approach’, when necessary, with a multidisciplinary team including a patient's haemato-oncologist and clinical nurse specialist, special care dentist, oral surgeon, dental hygienist and nutrition team, along with other relevant healthcare professionals.
Recommendation
It is recommended that dental care providers keep up-to-date on lymphoma management and can refer to Lymphoma Association UK for further information and to encourage people diagnosed with lymphoma and their carers to access the information and support at https://www.lymphomas.org.uk. The Royal College of Surgeons of England/The British Society for Disability and Oral Health (RCS/BSDH) (2012) provide clear strategies and a clinical guideline for the oral management of oncology patients requiring radiotherapy, chemotherapy and/or bone marrow transplantation. Studies show that oral healthcare is best delivered in these patients as an integral part of the general health assessment.74 However, this is not always possible. Hence the importance of a ‘shared care approach’, with GDPs, secondary dental care setting and haemato-oncology teams providing the best management and treatment outcomes for the patient, is essential.