Ghotane SG, Al-Haboubi M, Kendall N Dentists with enhanced skills (special interest) in endodontics: gatekeepers views in London. BMC Oral Health. 2015; 15
Al-Haboubi M, Newton P, Gallagher JE Meeting patient and professional needs: views of stakeholders on a training initiative for DwSIs in endodontics in London. Prim Dent J. 2016; 5:54-65
Pennington MW, Vernazza CR, Shackley P Evaluation of the cost-effectiveness of root canal treatment using conventional approaches versus replacement with an implant. Int Endod J. 2009; 42:874-883
Zitzmann NU, Krastl G, Hecker H Endodontics or implants? A review of decisive criteria and guidelines for single tooth restorations and full arch reconstructions. Int Endod J. 2009; 42:757-774
Kim SG, Solomon C Cost-effectiveness of endodontic molar retreatment compared with fixed partial dentures and single-tooth implant alternatives. J Endod. 2011; 37:321-325
Torabinejad M, White SN Endodontic treatment options after unsuccessful initial root canal treatment: alternatives to single-tooth implants. J Am Dent Assoc. 2016; 147:214-220
Esposito M, Trullenque-Eriksson A, Tallarico M Endodontic retreatment versus dental implants of teeth with an uncertain endodontic prognosis: 3-year results from a randomised controlled trial. Eur J Oral Implantol. 2018; 11:423-438
Byström A, Sundqvist G Bacteriologic evaluation of the efficacy of mechanical root canal instrumentation in endodontic therapy. Scand J Dent Res. 1981; 89:321-328
Byström A, Sundqvist G Bacteriologic evaluation of the effect of 0.5 percent sodium hypochlorite in endodontic therapy. Oral Surg Oral Med Oral Pathol. 1983; 55:307-312
Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K Outcome of primary root canal treatment: systematic review of the literature – Part 2. Influence of clinical factors. Int Endod J. 2008; 41:6-31
Ng YL, Mann V, Gulabivala K Outcome of secondary root canal treatment: a systematic review of the literature. Int Endod J. 2008; 41:1026-1046
Peters LB, Lindeboom JA, Elst ME, Wesselink PR Prevalence of apical periodontitis relative to endodontic treatment in an adult Dutch population: a repeated cross-sectional study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011; 111:523-528
López-López J, Jané-Salas E, Estrugo-Devesa A Frequency and distribution of root-filled teeth and apical periodontitis in an adult population of Barcelona, Spain. Int Dent J. 2012; 62:40-46
Di Filippo G, Sidhu SK, Chong BS Apical periodontitis and the technical quality of root canal treatment in an adult sub-population in London. Br Dent J. 2014; 216
Huumonen S, Suominen AL, Vehkalahti MM Prevalence of apical periodontitis in root filled teeth: findings from a nationwide survey in Finland. Int Endod J. 2017; 50:229-236
Van der Veken D, Curvers F, Fieuws S, Lambrechts P Prevalence of apical periodontitis and root filled teeth in a Belgian subpopulation found on CBCT images. Int Endod J. 2017; 50:317-329
Friedman S Considerations and concepts of case selection in the management of post-treatment endodontic disease (treatment failure). Endod Topics. 2002; 1:54-78
Patel S, Brown J, Pimentel T Cone beam computed tomography in endodontics – a review of the literature. Int Endod J. 2019; 52:1138-1152
Patel S, Dawood A, Ford TP, Whaites E The potential applications of cone beam computed tomography in the management of endodontic problems. Int Endod J. 2007; 40:818-830
Patel S, Wilson R, Dawood A, Mannocci F The detection of periapical pathosis using periapical radiography and cone beam computed tomography – part 1: pre-operative status. Int Endod J. 2012; 45:702-710
Rohlin M, Akesson L, Hakansson J Comparison between panoramic and periapical radiography in the diagnosis of periodontal bone loss. Dentomaxillofac Radiol. 1989; 18:72-76
Velvart P, Hecker H, Tillinger G Detection of the apical lesion and the mandibular canal in conventional radiography and computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001; 92:682-688
Nakata K, Naitoh M, Izumi M Effectiveness of dental computed tomography in diagnostic imaging of periradicular lesion of each root of a multirooted tooth: a case report. J Endod. 2006; 32:583-587
Estrela C, Bueno MR, Leles CR Accuracy of cone beam computed tomography and panoramic and periapical radiography for detection of apical periodontitis. J Endod. 2008; 34:273-279
Low KM, Dula K, Bürgin W, von Arx T Comparison of periapical radiography and limited cone-beam tomography in posterior maxillary teeth referred for apical surgery. J Endod. 2008; 34:557-562
Patel S, Dawood A, Whaites E, Pitt Ford T New dimensions in endodontic imaging: part 1. Conventional and alternative radiographic systems. Int Endod J. 2009; 42:447-462
Patel S, Kanagasingam S, Mannocci F Cone beam computed tomography (CBCT) in endodontics. Dent Update. 2010; 37:373-379
Patel S, Durack C, Abella F Cone beam computed tomography in endodontics – a review. Int Endod J. 2015; 48:3-15
Patel S, Patel R, Foschi F, Mannocci F The impact of different diagnostic imaging modalities on the evaluation of root canal anatomy and endodontic residents' stress levels: a clinical study. J Endod. 2019; 45:406-413
Use of cone-beam computed tomography in endodontics joint position statement of the American Association of Endodontists and the American Academy of Oral and Maxillofacial Radiology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011; 111:234-237
AAE and AAOMR joint position statement: use of cone beam computed tomography in endodontics 2015 update. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015; 120:508-512
Patel S, Saunders WP Radiographs in endodontics.(eds). London: Faculty of General Dental Practice (UK); 2013
Patel S, Brown J, Semper M European Society of Endodontology position statement: use of cone beam computed tomography in endodontics. Int Endod J. 2019; 52:1675-1678
ICRP publication 103. Ann ICRP. 2007; 37:1-332
Grant GT Direct digital manufacturing.(eds). Oxford: Wiley-Blackwell; 2015
Gambarini G, Ropini P, Piasecki L A preliminary assessment of a new dedicated endodontic software for use with CBCT images to evaluate the canal complexity of mandibular molars. Int Endod J. 2018; 51:259-268
Segato AVK, Piasecki L, Felipe Iparraguirre Nuñovero M The accuracy of a new cone-beam computed tomographic software in the preoperative working length determination ex vivo. J Endod. 2018; 44:1024-1029
Schäfer E Preparation of the root canal system.(ed). Edinburgh: Churchill Livingstone; 2017
Clark D, Khademi J Modern molar endodontic access and directed dentin conservation. Dent Clin North Am. 2010; 54:249-273
Gluskin AH, Peters CI, Peters OA Minimally invasive endodontics: challenging prevailing paradigms. Br Dent J. 2014; 216:347-353
Plotino G, Grande NM, Isufi A Fracture strength of endodontically treated teeth with different access cavity designs. J Endod. 2017; 43:995-1000
McCabe PS, Dummer PM Pulp canal obliteration: an endodontic diagnosis and treatment challenge. Int Endod J. 2012; 45:177-197
Byun C, Kim C, Cho S Endodontic treatment of an anomalous anterior tooth with the aid of a 3-dimensional printed physical tooth model. J Endod. 2015; 41:961-965
Zubizarreta Macho Á, Ferreiroa A, Rico-Romano C Diagnosis and endodontic treatment of type II dens invaginatus by using cone-beam computed tomography and splint guides for cavity access: a case report. J Am Dent Assoc. 2015; 146:266-270
Ng YL, Mann V, Gulabivala K A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: part 1: periapical health. Int Endod J. 2011; 44:583-609
Krastl G, Zehnder MS, Connert T Guided endodontics: a novel treatment approach for teeth with pulp canal calcification and apical pathology. Dent Traumatol. 2016; 32:240-246
Schilder H Cleaning and shaping the root canal. Dent Clin North Am. 1974; 18:269-296
van der Meer WJ, Vissink A, Ng YL, Gulabivala K 3D Computer aided treatment planning in endodontics. J Dent. 2016; 45:67-72
Strbac GD, Schnappauf A, Giannis K Guided modern endodontic surgery: a novel approach for guided osteotomy and root resection. J Endod. 2017; 43:496-501
Ahn SY, Kim NH, Kim S Computer-aided design/computer-aided manufacturing-guided endodontic surgery: guided osteotomy and apex localization in a mandibular molar with a thick buccal bone plate. J Endod. 2018; 44:665-670
Giacomino CM, Ray JJ, Wealleans JA Targeted endodontic microsurgery: a novel approach to anatomically challenging scenarios using 3-dimensional-printed guides and trephine burs – a report of 3 cases. J Endod. 2018; 44:671-677
Lara-Mendes STO, Barbosa CFM, Santa-Rosa CC, Machado VC Guided endodontic access in maxillary molars using cone-beam computed tomography and computer-aided design/computer-aided manufacturing system: a case report. J Endod. 2018; 44:875-879
Buchgreitz J, Buchgreitz M, Bjørndal L Guided root canal preparation using cone beam computed tomography and optical surface scans – an observational study of pulp space obliteration and drill path depth in 50 patients. Int Endod J. 2019; 52:559-568
Hawkins TK, Wealleans JA, Pratt AM, Ray JJ Targeted endodontic microsurgery and endodontic microsurgery: a surgical simulation comparison. Int Endod J. 2020; 53:715-722
Chong BS, Dhesi M, Makdissi J Computer-aided dynamic navigation: a novel method for guided endodontics. Quintessence Int. 2019; 50:196-202
Block MS, Emery RW Static or dynamic navigation for implant placement-choosing the method of guidance. J Oral Maxillofac Surg. 2016; 74:269-277
Block MS, Emery RW, Cullum DR, Sheikh A Implant placement is more accurate using dynamic navigation. J Oral Maxillofac Surg. 2017; 75:1377-1386
Gambarini G, Galli M, Stefanelli LV Endodontic microsurgery using dynamic navigation system: a case report. J Endod. 2019; 45:1397-1402.e6
Dhesi M, Chong BS Dynamic navigation for guided endodontics – a case report. ENDO (Lond Engl). 2020; 14:327-333
Get smart – technological innovations in endodontics. Part 1: 3D imaging, 3D treatment planning and guided endodontics Pratik Kamalkant Shah Qianni Zhang Bun San Chong Dental Update 2024 48:6, 707-709.
Authors
Pratik KamalkantShah
BDS, MJDF RCS Eng, MSc, MEndo RCS Edin, FHEA
Clinical Lecturer in Endodontics, Institute of Dentistry, Barts and The London School of Medicine and Dentistry, Queen Mary University of London.
Professor of Restorative Dentistry/Honorary Consultant, Academic Endodontic Lead, Institute of Dentistry, Barts and The London School of Medicine and Dentistry.
Endodontic treatment can be technically challenging, requiring a high level of clinical precision and skill to avoid mishaps, to achieve a quality result and to ensure a favourable outcome. Understandably, dentists vary in competency and ability to manage challenging endodontic cases. Coupled with patients' desire to retain their natural dentition, the demand for endodontic treatment exceeds service provision. Secondary and tertiary care providers are inundated with referrals. Access to privately funded services may also be restricted due to availability and locality. The scientific and technological revolution in healthcare has benefited many medical and dental disciplines, including endodontics: solutions may be found within these technological innovations to improve and facilitate the delivery of endodontic care.
CPD/Clinical Relevance: Technological innovations can contribute and facilitate the assessment, management and treatment of challenging endodontic cases in everyday clinical practice.
Article
Endodontics has long been considered the ‘Cinderella’ of dentistry.1 To many, including the dental profession, endodontics is a difficult discipline to master, and not held in as high regard or as appreciated as other restorative specialties and, hence, often relegated in terms of importance. In the 2009 report published after the independent review into UK's National Health Service (NHS) dentistry led by the late Professor Jimmy Steele is the following very apt description: ‘The technical challenges of, for example, providing root treatment in a molar tooth involve preparation to tenths of millimetres of accuracy in a root canal narrower than a pin and in a place the dentist cannot see’.2
As life expectancy increases, the need for endodontic services also increases. The demand for endodontic services remains unabated and is actually rising;3,4 it is also driven by individuals' desire to retain their natural teeth. In addition, endodontic treatments to salvage natural teeth are often less expensive, take less overall time, and enjoy a high survival rate.5,6,7,8,9
The most common procedure in endodontics, non-surgical root canal treatment, basically involves the thorough chemo-mechanical preparation and disinfection of the root canal system,10,11 followed by the complete three-dimensional obturation of the root canal space.12,13 Non-surgical root canal treatment can be relatively straightforward for teeth where the pulp space is not reduced or altered significantly because the location and negotiation of the root canal/s are not hampered. However, pulp canal obliteration, developmental abnormalities and patient management issues may present procedural challenges during non-surgical root canal treatment.
Epidemiological studies have shown that the technical quality of non-surgical root canal treatment remains poor: a favourable treatment outcome is not always achieved and as a result there is persistence of disease.14,15,16,17,18 In the absence of a favourable treatment outcome and the presence of persistent or secondary infection,19 remedial treatment, including non-surgical or surgical retreatment, may be needed if the tooth is to be retained.
Recent technological developments in 3D imaging, 3D treatment planning and guided endodontics can help in the management of complex endodontic cases, and help foster operator skill development. These technological developments are discussed in Part 1 of this two-part series.
3D radiographic imaging
Dental radiography, commonly in the form of peri-apical and dental panoramic radiographs, has limitations, such as anatomical noise from superimposition of orofacial structures, compression of three-dimensional (3D) objects into a two-dimensional (2D) image, and geometric distortion due to variation in angulation and position of films/sensors.20 Thus, small lesions, confined to cancellous bone and hidden by the overlying cortical plate, may escape detection.20,21,22
Cone beam computed tomography (CBCT), a relatively new digital imaging modality, may be used to overcome these limitations by providing 3D imaging across multiple planes.20,22 Several studies have highlighted the accuracy and sensitivity of CBCT compared with 2D radiography at detecting endodontic disease.20,22,23,24,25,26 CBCT, by providing visual guidance in 3D, has enhanced the understanding and interpretation of complex anatomical structures, benefiting diagnosis and treatment planning.20,22,26,27,28,29,30,31
Various guidelines have been published to assist clinicians in case selection and to promote the safe use of CBCT in endodontics.32,33,34,35,36
CBCT should always be used on a case-by-case basis, justified, and the potential benefits should outweigh the risks.33,34,36,37 When a CBCT scan is prescribed, the radiation dose should be kept ‘as low as reasonably achievable (ALARA)’ by limiting the field of view, adjusting the voxel size, current, and exposure time, allowing a pulsed and restricted arc of exposure.33,34,36
While there are significant advantages with 3D imaging, it is the use and application of the data, for example 3D treatment planning and guided endodontics (see later), that make this technological innovation a game changer in patient management. As the source of 3D imaging data, CBCT scans underpin the accuracy and function of secondary devices or software that may be used for planning and/or performing treatment. These volumetric data exist in a Digital Imaging and Communications in Medicine (DICOM) format to facilitate exchange between the different manufacturers and platforms.38
3D treatment planning
3D virtual planning software, such as SICAT Endo (Dentsply Sirona, Salzburg, Austria), have been specifically designed for the assessment of root canal anatomy and pre-operative root canal working length determination. Relying on data from CBCT scans, the precursor software 3D Endo (Dentsply Sirona) is able to accurately determine the working length of root canals by tracing and computing the measurement in 3D, thereby accounting for canal curvatures and complexities.39 Data from 3D radiographic imaging processed by 3D planning software can assist clinicians in treatment planning, for example in complex cases requiring endodontic treatment, through identification of root canal anatomy and determination of root canal working lengths.20,31 A study demonstrated the usefulness of 3D planning software and CBCT for the evaluation of the root canal anatomy and working length determination.31 The use of these digital technologies was reported to reduce stress levels for operators during treatment.31 Another study compared the accuracy between root canal working length readings measured using 3D Endo (Dentsply Sirona) software, pre-operatively, and an electronic apex locator, intra-operatively, in human extracted single-rooted teeth.40 This study found no statistical difference between the measurements and suggested that, for cases with a pre-operative CBCT scan available, 3D Endo software could be used to accurately determine the working length of root canals.40
An earlier study by Segato et al41 supported the combined use of measurements from 3D Endo (Dentsply Sirona) software and electronic apex locators for accurate determination of the root canal terminus. Further research is required involving multi-rooted teeth and different CBCT image settings that may influence the accuracy of these measurements. In the future, incorporation of artificial intelligence (see Part 2) software may permit automated detection of features pertinent to treatment planning and management, such as the presence of untreated or additional canals, pre-operative working length, apical size diameter, and apical pathosis.
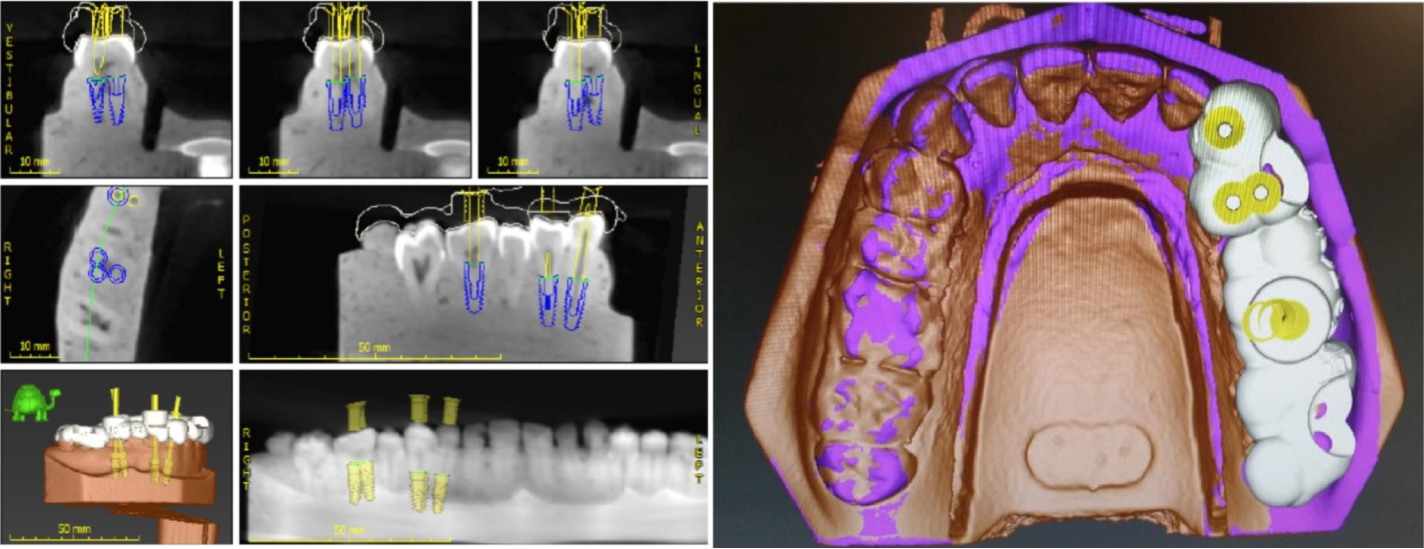
Matched data from CBCT scans and optical (intra-oral/plaster model) scans can also be used with implant planning software, for example, coDiagnostiX (Dental Wings Inc, Montreal, Canada) for treatment planning and to help clinicians visualize root canal treatment complexities (Figure 1). 3D planning software, depending on equipment and treatment option chosen, can subsequently be used in guided endodontics (see later) for designing 3D printed guides for static guidance, or set parameters for dynamic guidance.
Figure 1. Virtual planning of access cavities using coDiagnostiX (Dental Wings Inc, Montreal, Canada). The yellow lines on the radiographic images represent straight-line access pathways to the root canal system of the mandibular right canine, first premolar and first molar. The occlusal view of the 3D-rendered model showing corresponding positions of the access cavities on a virtual guidance stent. Please note the overlapping access cavity positions for the mandibular right first molar.32
Guided endodontics
During non-surgical root canal treatment, the access cavity should be prepared according to access requirements while avoiding unnecessary and destructive tooth tissue removal.42 The advent of the ‘minimally invasive endodontics’,43,44 in line with the ‘minimal invasive dentistry’ concept, means that access cavities should be kept as conservative as possible. Instead of the traditional endodontic cavity, conservative/contracted endodontic cavity and ultraconservative ‘ninja’ endodontic cavities have been advocated.45 However, there are a number of clinical scenarios that hamper the desire to be conservative. For example, in order to locate the root canal system of teeth with a calcified root canal system (pulp canal obliteration), dens invaginatus or dilacerated roots,46,47,48 increasing amounts of tooth tissue may need to be removed, compromising structural integrity, risking perforation and a negative treatment outcome.49 Thus, any strategy or technique that allows for the preparation of minimal access cavities, preserving tooth structural integrity with reduced risk of procedural errors and still meets ideal shaping and preparation objectives50 would be extremely beneficial. Similarly, for apical surgery, where access to the root-end is constrained due to tooth position, a thick cortical bone plate, and/or close proximity to critical anatomical structures, any method or technique that permits minimally invasive osteotomies, safe removal of lesions and accurate resection of root-ends would be equally helpful.
In dental implant surgery, the use of some form of guidance system, to ensure placement at the desired location, depth and angulation, has been an area of interest for some time. The advent of 3D imaging has led to the development of techniques to improve the accuracy of dental implant surgery by using guidance based on CBCT-acquired data. The guided implant placement concept has been adopted and adapted to endodontics. Guided endodontics mean that challenging cases requiring endodontic treatment may be managed with greater accuracy, reduced risk of procedural errors and iatrogenic injuries. Guided endodontics relies on careful pre-operative treatment planning software and matched data acquired from CBCT and optical scans, and depending on the treatment modality, may be classified as static or dynamic.
Static guidance
Static guidance refers to use of a removable stent (Figure 2), for example fabricated using 3D printing involving computer-aided design/computer-assisted manufacture (CAD/CAM) and additive manufacturing techniques, based on the matched data from pre-operative CBCT and optical scans. 3D printed stents, designed on 3D planning software, may be tooth-, mucosa-or bone-supported, and encode the depth and angulation required to accurately perform treatment procedures.
Figure 2. 3D-printed stents to provide static guidance for the location of the root canal system of the mandibular right canine, first premolar and first molar. Due to the angulations and overlapping positions of access cavities for the mandibular right first molar (see Figure 1), three guides were necessary.
Several case reports and studies have been published documenting the transfer of 3D imaging data to implant planning software and 3D printers for the design and production of printed stents in endodontic treatment.47,48,51,52,53,54,55,56,57,58 The use of guidance stents has been reported to be minimally invasive, reducing operating time, allowing greater accuracy, better patient comfort and facilitating operator skill development. Thus, challenging endodontic cases where there is increased risk of procedural errors may be treated safely without compromising outcome. However, the use of 3D printed stents has several drawbacks that limit its wider adoption. These include additional treatment planning time, production cost of the stents, access difficulties for patients with limited mouth opening and in the molar tooth regions.59,60 Most importantly, unchangeable (static) operational parameters, such as angle and size of guide sleeves, may afford no or very limited leeway for intra-operative corrections and the requirement for multiple stents for each canal in a multi-rooted tooth (Figure 2).56,59,61,62
Dynamic navigation
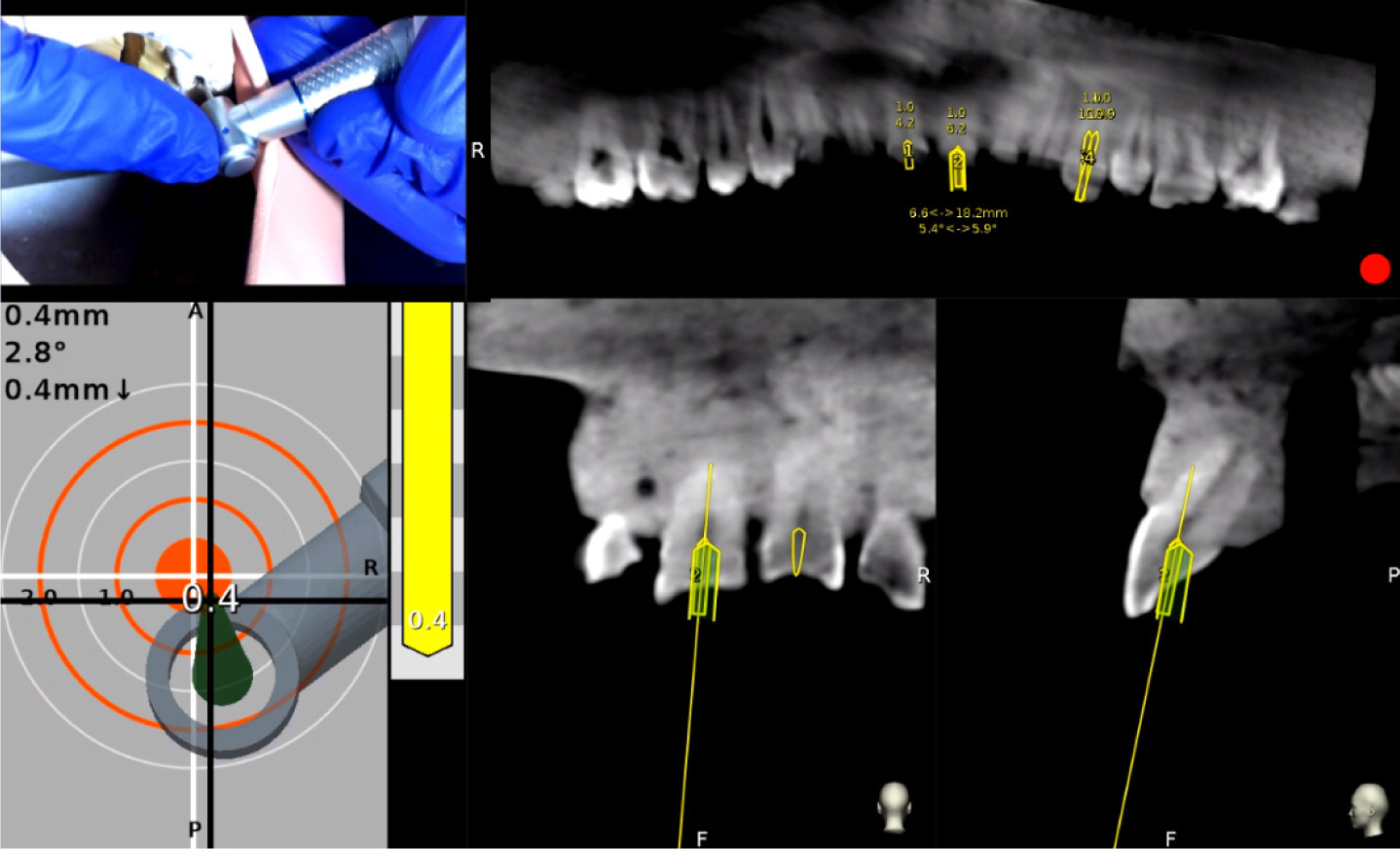
Dynamic guidance, based on computer-aided surgical navigation technology and analogous to global positioning systems or satellite navigation, has been used in an attempt to overcome the limitations of static guidance in dental implant surgery. Dynamic guidance uses matched 3D imaging data to provide real-time visual feedback to the operator with the help of optical motion tracking cameras. Chong et al59 demonstrated the potential of Navident (ClaroNav Technology Inc, Toronto, Canada), a dynamic guidance system designed for implant placement, in non-surgical root canal treatment for minimally invasive access cavity preparation and canal location (Figure 3). Recent case reports documented the application of dynamic guidance in facilitating precise performance of a minimally invasive osteotomy and root-end resection during apical surgery,63 and conservative access cavity preparation, with canal location, during non-surgical root canal treatment.64
Figure 3.
A dynamic navigation implant system (Navident; ClaroNav Technology Inc, Toronto, Canada) used for the virtual planning and location of the root canal systems. The real-time position of the handpiece bur (upper left image) is displayed on a computer screen over the CBCT image (upper and lower right images) as the user guides the procedure for maxillary right central incisor and the maxillary left canine by following a target rendering (lower left image).
Unlike static guidance, dynamic guidance relies on meticulous treatment planning and there are still, albeit lower, cost and time considerations. Although proof-of-concept has been demonstrated63 there are a number of issues to consider before the technology can be fully used in everyday endodontic practice. The treatment planned virtually has to be transferred to the actual patient; visualization and real-time guidance of the treatment plan and real-time monitoring of procedural steps are still displayed on 2D computer monitors. Therefore, having to concentrate on the 2D display monitor forces the clinician to look away from the patient and even from their own hands, contrary to normal in which the operator directly faces the patient. Apart from being unnatural, this working position hampers hand-eye co-ordination; it is also inefficient and risks mishaps. A possible solution to this problem may be the use of augmented or mixed reality (see Part 2) to complement dynamic guidance.
Conclusions
Technological developments, such as 3D imaging, 3D treatment planning and guided endodontics, may help manage complex endodontic cases and can play an important role in dental education.