Camoes ICG, Salles MR, Fernando MVM, Lilian FF, Gomes CC. Relationship between the size of patency file and apical extrusion of sodium hypochlorite. Ind J Dent Res. 2009; 20:426-430
Fatemah F, Abo-Alhassan F, Sadeq A, Burezq H. Complication of improper management of sodium hypochlorite accident during root canal treatment. J Int Soc Prev Community Dent. 2016; 6:493-496
Al-Sebaei MO, Halabi OA, El-Hakim IE. Sodium hypochlorite accident resulting in life-threatening airway obstruction during root canal treatment: a case report. Clin Cosmet Investig Dent. 2015; 7:41-44
Akhlaghi NM, Mohajeri LB, Fazlyabb M. Tissue necrosis due to chloroform: a case report. Iran Endod J. 2013; 8:208-209
Flaman Z, Pellechia-Clarke S, Bailey B, McGuigan M. Unintentional exposure of young children to camphor and eucalyptus oils. Paediatr Child Health. 2001; 6:80-83
Ribeiro DA, Matsumoto MA, Marques ME, Salvadori DM. Biocompatibility of gutta-percha solvents using in vitro mammalian test-system. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 103:e106-e109
Uemura M, Hata G, Toda T, Weine FS. Effectiveness of eucalyptol and d-limonene as gutta-percha solvents. J Endod. 1997; 23:739-741
Hunter KR, Doblecki W, Pelleu GB. Halothane and eucalyptol as alternatives to chloroform for softening gutta-percha. J Endod. 1991; 17:310-311
Wennberg A, Orstavik SC. Evaluation of alternatives to chloroform in endodontic practice. Endod Dent Traumatol. 1989; 5:234-237
Reuber MD. Carcinogenicity of chloroform. Environ Health Perspect. 1979; 31:171-182
Vajrabhaya LO, Suwannawong SK, Kamolroongwarakul R, Pewklieng L. Cytotoxicity evaluation of gutta-percha solvents: Chloroform and GP-Solvent (limonene). Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004; 98:756-759
Zaccaro Scelza MF, Lima Oliveira LR, Carvalho FB, Côrte-Real Faria S. In vitro evaluation of macrophage viability after incubation in orange oil, eucalyptol, and chloroform. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006; 102:e24-e27
Hansen MG. Relative efficiency of solvents used in endodontics. J Endod. 1998; 24:38-40
Yadav HK, Yadav RK, Chandra A, Thakkar RR. The effectiveness of eucalyptus oil, orange oil, and xylene in dissolving different endodontic sealers. J Conserv Dent. 2016; 19:332-337
Friedman S, Stabholtz A, Tamse A. Endodontic retreatment – case selection and technique. Part 3: retreatment techniques. J Endodont. 1990; 16:543-549
Martos J, Bassotto AP, González-Rodríguez MP, Ferrer-Luque CM. Dissolving efficacy of eucalyptus and orange oil, xylol and chloroform solvents on different root canal sealers. Int Endod J. 2011; 44:1024-1028
Higgins C, Palmer A, Nixon R. Eucalyptus oil: contact allergy and safety. Contact Dermatitis. 2015; 72:344-346
Falcon HC, Richardson P, Shaw MJ, Bulman JS, Smith BGN. Developing an index of restorative dental treatment need. Br Dent J. 2001; 190:479-486
Virdee SS, Thomas SC. A practitioner's guide to gutta-percha removal during endodontic retreatment. Br Dent J. 2017; 222:251-257
Kasam S, Mariswamy SC. Efficacy of different methods for removing root canal filling material in retreatment – an in-vitro study. J Clin Diagn Res. 2016; 10:ZC06-ZC10
Eucalyptus Extrusion Injury: not such an Essential Oil? Zhain Mustufvi Benjamin Veale Karolina Tkacz Aidan Adams Ahmed Al-Khayyat Dental Update 2024 47:3, 707-709.
Authors
ZhainMustufvi
BDS
Consultant and Specialist in Restorative Dentistry and Oral/Facial Rehabilitation, Bradford Teaching Hospitals Foundation Trust, Duckworth Lane, Bradford BD9 6RJ, UK
Consultant and Specialist in Restorative Dentistry and Oral/Facial Rehabilitation, Bradford Teaching Hospitals Foundation Trust, Duckworth Lane, Bradford BD9 6RJ, UK
Consultant and Specialist in Restorative Dentistry and Oral/Facial Rehabilitation, Bradford Teaching Hospitals Foundation Trust, Duckworth Lane, Bradford BD9 6RJ, UK
Consultant and Specialist in Restorative Dentistry and Oral/Facial Rehabilitation, Bradford Teaching Hospitals Foundation Trust, Duckworth Lane, Bradford BD9 6RJ, UK
Consultant and Specialist in Restorative Dentistry and Oral/Facial Rehabilitation, Bradford Teaching Hospitals Foundation Trust, Duckworth Lane, Bradford BD9 6RJ, UK
Eucalyptus oil is an essential oil commonly used as a solvent to remove old gutta-percha when performing endodontic re-treatment procedures. Although commonly used by dentists, evidence for its safety is lacking. This report outlines a previously undocumented case of a 44-year-old male who attended the Oral and Maxillofacial Surgery department with sudden onset facial swelling in response to extrusion of eucalyptus oil through the apex of a tooth during root canal re-treatment by his dentist. The management of this case is discussed and the important safety aspects with regard to the chemicals used in endodontic treatments are reviewed.
CPD/Clinical Relevance: This paper highlights that the risk of extrusion injury during endodontic treatment is not limited to the use of sodium hypochlorite but also to other chemicals such as, and in our case, eucalyptus oil.
Article
Case report
A 44-year-old male was referred to the Oral and Maxillofacial department on an acute basis with a history of a sudden onset of facial swelling. The swelling of the lower right cheek had appeared during root canal re-treatment of the lower right second premolar (LR5) by his general dental practitioner (GDP) earlier that morning. It had worsened over the following few hours. His medical history was unremarkable except for a penicillin allergy.
On discussion with the dentist, it was reported that, during the re-treatment, eucalyptus oil (EO) was used to help dissolve the gutta-percha (GP) root canal filling material, and that this was delivered using an irrigation syringe. Irrigation of the canal with EO had elicited immediate severe pain around the jaw, shortly followed by onset of swelling. It was concluded that this was due to an extrusion injury involving the EO. It was reported that no other irrigants were used. Treatment was discontinued and the tooth was temporized appropriately.
Examination revealed tender right-sided facial swelling involving the lower lip, right periorbital region, buccal and submandibular spaces, and early necrosis of the buccal mucosa adjacent to the LR5 (Figures 1 and 2). The LR5 was tender to percussion. There were no airway concerns and the patient was systemically well, with normal observations. There was no sensory deficit.
Figure 1. Marked right-sided buccal space and periorbital involvement swelling.Figure 2. Intra-oral tissue necrosis in the right buccal sulcus.
The patient was admitted to hospital and given analgesia, intravenous (IV) dexamethasone and IV antibiotics (clarithromycin and metronidazole). On discussion, the patient decided against further endodontic treatment, and the LR5 was extracted the following day under general anaesthesia with copious saline irrigation and limited debridement of the adjacent necrotic buccal mucosa. The patient was discharged 48 hours after admission on oral antibiotics, following improvement in his pain and swelling. He was reviewed 3 weeks post-discharge and all presenting features had resolved.
Discussion
Extrusion injuries in dentistry are relatively rare, and are more commonly associated with the use of sodium hypochlorite (NaOCl) during endodontic treatments when forceable pressure on an engaging and non side-venting irrigation needle is used. This arises from inadvertent application of NaOCl into the peri-radicular tissues, typically through the apical foramen, accessory canals or via perforations of the pulp floor or canal wall. The risk of injury is increased in teeth with immature or over-instrumented apices.1,2
The presence of NaOCl in the tissues results in an intense inflammatory response, causing significant tissue necrosis, and can cause widespread oedematous swelling and contusion.3 Whilst the injury can be localized to the periodontium and surrounding mucosa, it is also frequently reported as more widespread, involving periorbital tissues, neck, and even mediastinum, with airway compromise reported.4 The injury pattern of ecchymosis follows the superficial venous vasculature draining from the teeth and bone into the surrounding veins. In the maxilla, this may be the anterior or posterior superior alveolar veins and, in the mandible, this can include the inferior alveolar vein.1 Interestingly, the above case demonstrated no ecchymosis of the overlying skin.
To the authors' knowledge, this is the first reported extrusion injury involving EO, although it has previously been reported involving chloroform, resulting in localized tissue necrosis5. EO is reported to be a safe and biocompatible material,6 yet is known to cause mucosal irritation,7 a burning sensation within the oral cavity,8 and has been shown to be cytotoxic.9
Eucalyptus oil is an essential oil distilled from the leaf of ‘Eucalyptus’, a plant from the family of Myrtaceae. The main constituent of the oil is the chemical 1,8-cineol, also known as ‘Eucalyptol’. Within dentistry, EO is most commonly used as a solvent in the re-treatment of root canal systems previously obturated with GP, and is considered a safer alternative to chloroform10,11 which, while highly effective,12 remains controversial due to its carcinogenic potential.13,14,15 During re-treatment, it is advised to use a chemo-mechanical approach as root filling materials often resist mechanical instrumentation.16 Various solvents can be used for this purpose, including xylene, halothane, orange oil, rectified turpentine, Endosolv (Septodont) and Ethyl Benzene and ether.6 Orange oil has been demonstrated to be significantly less cytotoxic than EO15 and has comparative effectiveness in removing GP and endodontic sealant.6,17,18
Other uses vary widely. In alternative medicine, it is used as an antibacterial agent, and can also be used in low doses as flavouring in foods and as a fragrant in soaps and perfumes. Documented incidents involving EO are mainly from ingestion, resulting in vomiting, coma, lethargy and seizures, and can be potentially fatal.8,19 Skin reactions have been noted to involve contact dermatitis.20
Endodontic re-treatment can be a complex procedure, and is recognized as such within the Restorative Index of Treatment Need.21 However, each case should be carefully assessed with respect to anticipated complexity, and many are within the scope of practice of appropriately experienced GDPs. The quality of the existing obturation may give an indication as to the complexity of GP removal; for example, poorly-condensed GP with numerous voids will likely allow instruments to pass into the canal more easily, whereas well-condensed GP is likely to be more challenging.22
In re-treatment, solvents should be used sparingly with careful introduction into the root canal system. Virdee details how Gates Glidden burs can be used initially to remove the GP mechanically from the coronal one to two thirds of the canal, alongside copious irrigation to remove the debris.22 The apical GP is then removed using a combination of ISO K files and Hedström files carefully measured to length. Finally, the authors advocate the use of a solvent to retrieve any GP remnants, especially in curved canals. They recommend flushing the canals and aspirating repeatedly and using paper points to absorb the dissolved root filling material. In the context of this case, inappropriate irrigation technique may introduce unnecessary risk.
An alternative technique described in the literature is to remove the first 2−3 mm of GP below the cementoenamel junction thus creating a reservoir for the solvent. This is followed by mechanical instrumentation of the canal to the working length using either Hedström files, rotary files or ultrasonic retreatment tips.23
When irrigants are used within the root canal system, the operator should exercise caution in order to prevent extrusion into the peri-radicular tissues:
Finger pressure, as opposed to thumb pressure, should be used (Figure 3);
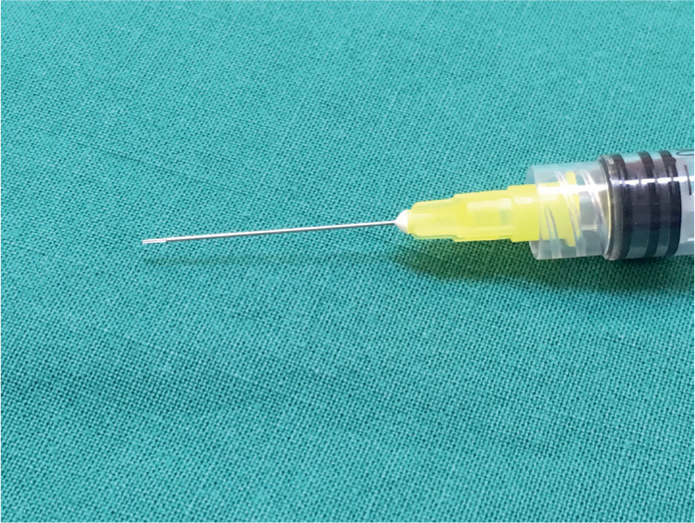
A side-vented syringe passively placed into the canal circulates the irrigant within the canal without undue pressure through the apical constriction (Figure 4);
Over-preparation of the apex should be avoided when possible if instrumenting the canal, and apical patency procedures should be adopted with care;
High quality pre-operative radiographs can help identify potential risk factors for extrusion injury, such as open apices in immature teeth.
Figure 3. Irrigant is applied using finger pressure.Figure 4. Syringe has a side-venting needle.
Given the absence of previously reported cases of extrusion injury involving EO, the case discussed involved management based upon that of hypochlorite injuries, given the clinical similarity on presentation. Removal of the causative agent is the first key step, and typically will involve cessation of endodontic treatment, and dilution of the agent within the root canal system using a neutral and inert irrigant, such as saline. Antibiotics are advised to prevent secondary infection following tissue necrosis, and steroids can reduce swelling. Management is, of course, subjective and dependent on the severity of the injury.
Conclusion
This case highlights the importance of careful use with all chemicals within endodontics, and not just with sodium hypochlorite. Whilst EO is an effective solvent and can be used safely within re-treatment procedures, care must be taken to ensure that delivery techniques complement this. It is unclear if other solvents may produce similar tissue damage, and further research is recommended to highlight the safest options. However, orange oil may be preferable to EO owing to its lower cytotoxicity. All cases must be assessed on an individual basis, and consideration should be given as to whether solvents are necessary at all.