Siqueira JF Endodontic infections: concepts, paradigms, and perspectives. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002; 94:281-293 https://doi.org/10.1067/moe.2002.126163
Barnes IE. Surgical Endodontics – A colour manual. 1984;
Iwu CO. Ludwig's angina: report of seven cases and review of current concepts in management. Br J Oral Maxillofac Surg. 1990; 28:189-193 https://doi.org/10.1016/0266-4356(90)90087-2
Martin SA. Conventional endodontic therapy of upper central incisor combined with cyst decompression: a case report. J Endod. 2007; 33:753-757 https://doi.org/10.1016/j.joen.2007.01.013
Kakehashi S, Stanley HR, Fitzgerald RJ. The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral Surg Oral Med Oral Pathol. 1965; 20:340-349 https://doi.org/10.1016/0030-4220(65)90166-0
Setzer FC, Shah SB, Kohli MR, Karabucak B, Kim S. Outcome of endodontic surgery: a meta-analysis of the literature – part 1: comparison of traditional root-end surgery and endodontic microsurgery. J Endod. 2010; 36:1757-1765 https://doi.org/10.1016/j.joen.2010.08.007
Tucker WM, Pleasants JE, MacComb WS. Decompression and secondary enucleation of a mandibular cyst: report of case. J Oral Surg. 1972; 30:669-673
Regan JD, Witherspoon DE, Foyle D. Surgical repair of root and tooth perforations. Endod Topics. 2005; 11:152-178
Cohenca N, Simon JH, Mathur A, Malfaz JM. Clinical indications for digital imaging in dento-alveolar trauma. Part 2: root resorption. Dent Traumatol. 2007; 23:105-113 https://doi.org/10.1111/j.1600-9657.2006.00546.x
Heithersay GS. Treatment of invasive cervical resorption: an analysis of results using topical application of trichloracetic acid, curettage, and restoration. Quintessence Int. 1999; 30:96-110
Lee SJ, Monsef M, Torabinejad M. Sealing ability of a mineral trioxide aggregate for repair of lateral root perforations. J Endod. 1993; 19:541-544 https://doi.org/10.1016/S0099-2399(06)81282-3
White C, Bryant N. Combined therapy of mineral trioxide aggregate and guided tissue regeneration in the treatment of external root resorption and an associated osseous defect. J Periodontol. 2002; 73:1517-1521 https://doi.org/10.1902/jop.2002.73.12.1517
Tran XV, Gorin C, Willig C Effect of a calcium-silicate-based restorative cement on pulp repair. J Dent Res. 2012; 91:1166-1171 https://doi.org/10.1177/0022034512460833
Torabinejad M, Parirokh M, Dummer PMH. Mineral trioxide aggregate and other bioactive endodontic cements: an updated overview – part II: other clinical applications and complications. Int Endod J. 2018; 51:284-317 https://doi.org/10.1111/iej.12843
Grech L, Mallia B, Camilleri J. Investigation of the physical properties of tricalcium silicate cement-based root-end filling materials. Dent Mater. 2013; 29:e20-28 https://doi.org/10.1016/j.dental.2012.11.007
Everett FG, Kramer GM. The disto-lingual groove in the maxillary lateral incisor; a periodontal hazard. J Periodontol. 1972; 43:352-361 https://doi.org/10.1902/jop.1972.43.6.352
Esposito M, Grusovin MG, Papanikolaou N Enamel matrix derivative (Emdogain) for periodontal tissue regeneration in intrabony defects. Cochrane Database Syst Rev. 2009; 2009:(4) https://doi.org/10.1002/14651858.CD003875.pub3
Darwazeh A, Hamasha AA. Radiographic evidence of enamel pearls in jordanian dental patients. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000; 89:255-258 https://doi.org/10.1067/moe.2000.103524
Chrcanovic BR, Abreu MH, Custódio AL. Prevalence of enamel pearls in teeth from a human teeth bank. J Oral Sci. 2010; 52:257-260 https://doi.org/10.2334/josnusd.52.257
Risnes S. The prevalence and distribution of cervical enamel projections reaching into the bifurcation on human molars. Scand J Dent Res. 1974; 82:413-419 https://doi.org/10.1111/j.1600-0722.1974.tb00395.x
Brook AH, Winter GB. Double teeth. A retrospective study of ‘geminated’ and ‘fused’ teeth in children. Br Dent J. 1970; 129:123-130 https://doi.org/10.1038/sj.bdj.4802533
Carnevale G, Pontoriero R, di Febo G. Long-term effects of root-resective therapy in furcation-involved molars. A 10-year longitudinal study. J Clin Periodontol. 1998; 25:209-214 https://doi.org/10.1111/j.1600-051x.1998.tb02430.x
Basten CH, Ammons WF, Persson R. Long-term evaluation of root-resected molars: a retrospective study. Int J Periodontics Restorative Dent. 1996; 16:206-219
Derks H, Westheide D, Pfefferle T Retention of molars after root-resective therapy: a retrospective evaluation of up to 30 years. Clin Oral Investig. 2018; 22:1327-1335 https://doi.org/10.1007/s00784-017-2220-1
Setzer FC, Shou H, Kulwattanaporn P Outcome of crown and root resection: a systematic review and meta-analysis of the literature. J Endod. 2019; 45:6-19 https://doi.org/10.1016/j.joen.2018.10.003
Gutmann JL. Perspectives on the use of root/tooth resections in the retention of teeth. Endo. 2007; 1:239-255
Fugazzotto PA. A comparison of the success of root resected molars and molar position implants in function in a private practice: results of up to 15-plus years. J Periodontol. 2001; 72:1113-1123 https://doi.org/10.1902/jop.2001.72.8.1113
Peer M. Intentional replantation – a ‘last resort’ treatment or a conventional treatment procedure? Nine case reports. Dent Traumatol. 2004; 20:48-55 https://doi.org/10.1046/j.1600-4469.2003.00218.x
Surgeon Commander (D) Graeme Bryce Royal Navy, Consultant in Restorative Dentistry, Centre for Restorative Dentistry, Defence Primary Health Care (Dental), Evelyn Woods Road, Aldershot, GU11 2LS
Surgical root canal re-treatment (SRCReT) or root-end surgery is the surgical endodontic technique most commonly studied and undertaken in clinical practice. A range of diagnostic, emergency and corrective surgical procedures may be included under the umbrella of endodontic surgery. The first article in this two-part series uses the best available evidence and clinical examples to provide the clinician with an overview of endodontic surgery.
CPD/Clinical Relevance: An updated review of endodontic surgical techniques is of relevance to clinicians.
Article
Endodontic surgery encompasses a broad range of surgical techniques that are aimed at addressing both pulpal and peri-radicular disease. Surgical root canal re-treatment (SRCReT) or root-end surgery is the most extensively researched endodontic surgical technique, and is aimed at treating root canals with persistent apical periodontitis when conventional non-surgical root canal re-treatment (NSRCReT) has failed, or when it is impractical to perform.1 However, surgical techniques that aim to manage endodontic emergencies, facilitate assessment or diagnosis and procedures to correct root or tooth defects are also included within this field (Table 1). Part 1 of this two-part series aims to give a broad overview of the applications of endodontic surgery. Part 2 provides a more in-depth review of the surgical protocol required for root-end surgery.
Emergency procedures
Incision and drainage
Trephination
Diagnostic assessment
Exploratory assessment for fractures and abnormal anatomy
Biopsy
Treatment of apical periodontitis/cysts
Root-end surgery ± regenerative procedures
Decompression and marsupialization
Corrective procedures
Repair of cervical resorption defects and perforations
Management of anatomical defects
Root resection/hemi-section/removal of fractured roots
Other
Intentional replantation
Emergency surgical endodontic procedures
Incision and drainage
Endodontic infections may result in apical abscess formation and the accumulation of both pus and inflammatory exudate within the peri-radicular tissues.2 The effective drainage of pus is one of the cornerstones of management of acute dental infections. Drainage through the root canal alone cannot always be achieved or may be ineffective because of the limited degree to which it can occur. Exudate will flow more freely from a patent unfilled canal compared to a canal that has been previously root canal treated. Therefore, incision and drainage may be required to remove trapped exudate.3
Incision and drainage of a swelling can be performed when there is a collection of pus within the soft tissues indicated by an intra- or extra-oral fluctuant swelling, which is often erythematous and tender to touch. Anaesthesia is achieved using either topical or local anaesthetic that is injected into the tissues adjacent to the swelling, rather than into the swelling itself. A number 11 or 15 scalpel blade can be used to incise the swelling. The incision should be designed so as not to damage important anatomical and nerve structures and to minimize scarring. If pus remains trapped within soft tissue locules, then blunt dissection can be used to release the exudate and promote maximal drainage. Aspiration biopsy using a needle and syringe can collect a sample of the exudate to be sent for microbiological evaluation. The cavity containing the pus should be thoroughly rinsed with saline using a syringe with a wide-bore needle. Following this, a restorability assessment of the tooth/teeth and discussion of treatment options with the patient may result in chemo-mechanical debridement of the root canals of the affected tooth/teeth, extraction or NSRCReT +/- root-end surgery.
The placement of a surgical drain may be indicated, depending on the severity of presenting symptoms (eg in the management of mandibular swellings with risk of lingual, submandibular or pharyngeal space involvement).4 General dental practitioners (GDPs) may consider referral to a specialist or secondary care. In such cases, the use of rubber dam, surgical tubing and other hollow-tubed items (such as fine impression tip nozzles) have been suggested as suitable devices through which to facilitate drainage.5 Drains must be radiopaque to enable them to be located radiographically if they are lost into the defect, or more rarely swallowed or even inhaled. Their dislodgement can be minimized by suturing them into place. Upon achievement of drainage, an appropriate antibiotic regimen should then be prescribed, if indicated. Drains should be reviewed after 48 hours and removed when no longer required. If the patient's condition deteriorates, appropriate referral to hospital should be considered.
Trephination
GDPs may also wish to refer to specialist or secondary care if the exudate is trapped within the alveolus, and where, consequently, trephination may be required to drain the exudate.3 It is important to identify anatomical structures (eg the mental nerve, maxillary sinus and roots of teeth) prior to surgery. Following local anaesthesia, a small horizontal incision is made between the middle to apical third of the root(s) of the affected tooth. A round size 4 or larger bur is used in a surgical handpiece to perforate the cortical plate and remove cortical bone until the inflammatory/infected exudate is reached. The area is enlarged just enough to allow curettage of any tissues and irrigation with saline at the root apex. Soft tissues can then be sutured +/- insertion of a drain if necessary. The drain should be reviewed at 48 hours and removed when no longer required.
Treatment of apical periodontitis/cysts
Diagnostic assessment
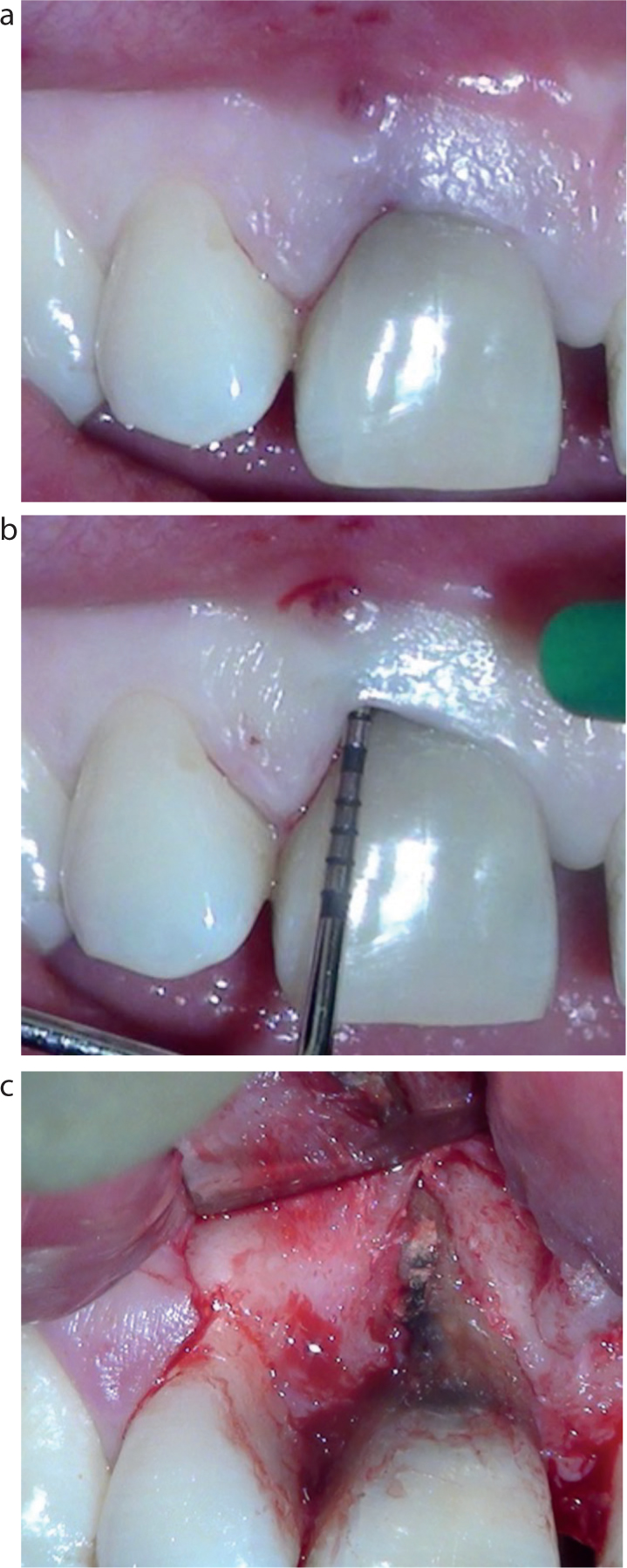
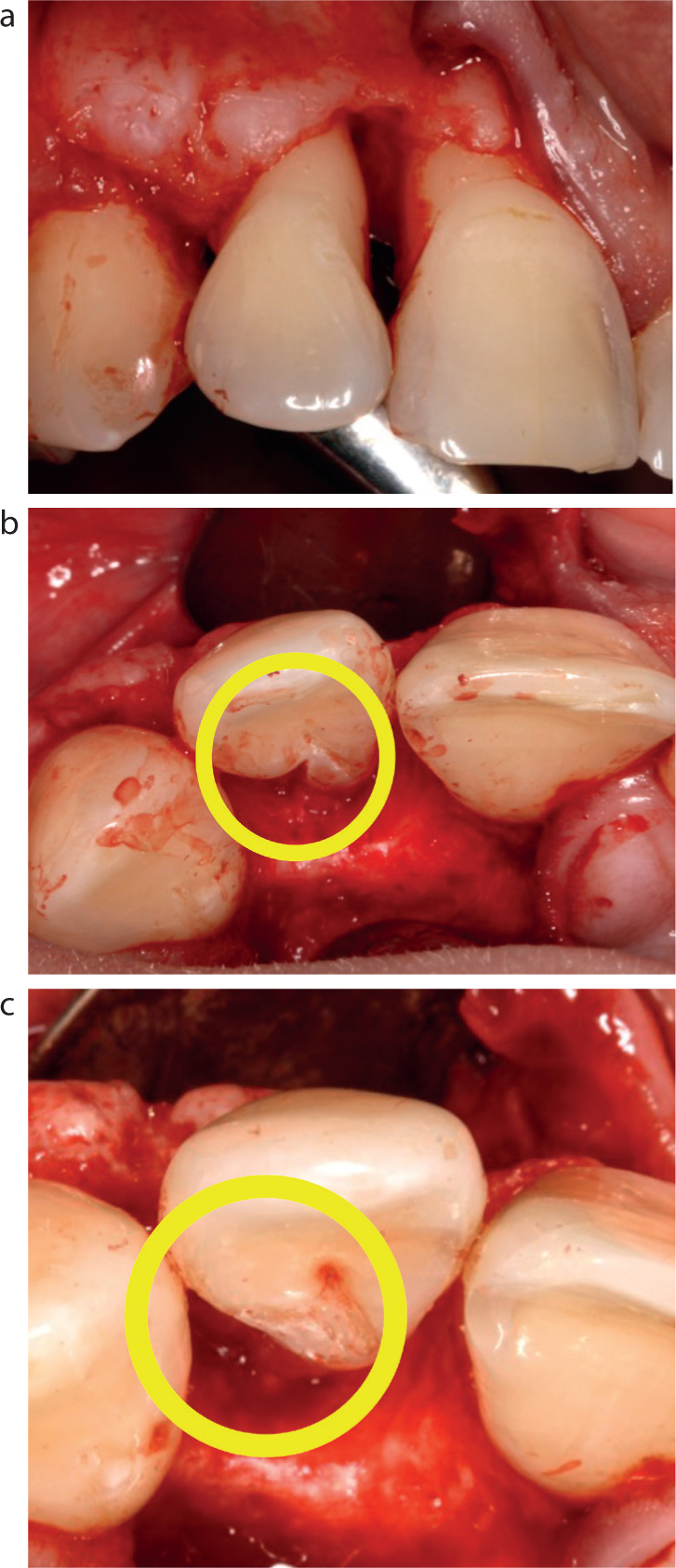
The availability of cone beam computerized tomography (CBCT) facilitating three-dimensional imaging has reduced the need for surgical intervention when conventional radiography has failed to confirm a diagnosis. However, on occasions, surgical access may be necessary for biopsy of non-odontogenic lesions and to confirm or exclude the presence/extent of root fractures, developmental anomalies and perforations (Figure 1).
Figure 1. Surgical assessment and confirmation of a vertical root fracture. (a) Pre-operative assessment of an upper right central incisor and buccal sinus; (b) localized periodontal pocketing defect; and (c) localized bone defect associated with a vertical root fracture.
Root-end surgery ± regenerative procedures
It is well established that infection of the root canal space is the primary causative factor in apical periodontitis, and that apical surgery is an accepted treatment method when NSRCReT has failed or is not feasible.1,6 Historically, apicectomy has been the principal term used to describe root-end surgery. However, this term only describes the apical root resection procedure and fails to highlight the foremost aim of the procedure: eliminating intra-radicular infection. Surgical root canal re-treatment (SRCReT) is therefore a more applicable term. Success rates for SRCReT range from 37% to over 90%, with a multitude of reasons explaining the disparity between studies (Table 2).7 A detailed discussion of an evidence-based surgical protocol for SRCReT, including regeneration, can be found in the second article in this two-part series.
General factors
Local factors
Differences in sample size
Case selection (diagnosis and identification of exacerbating factors, such as root fractures)
Period of follow-up (review)
Tooth type
Criteria used to evaluate success, eg strict vs loose criteria
Number of teeth involved
Extent of bone loss/size of lesion
Quality of the coronal seal
Quality of the root filling
Surgical protocol employed (including type of root-end filling)
Decompression and marsupialization
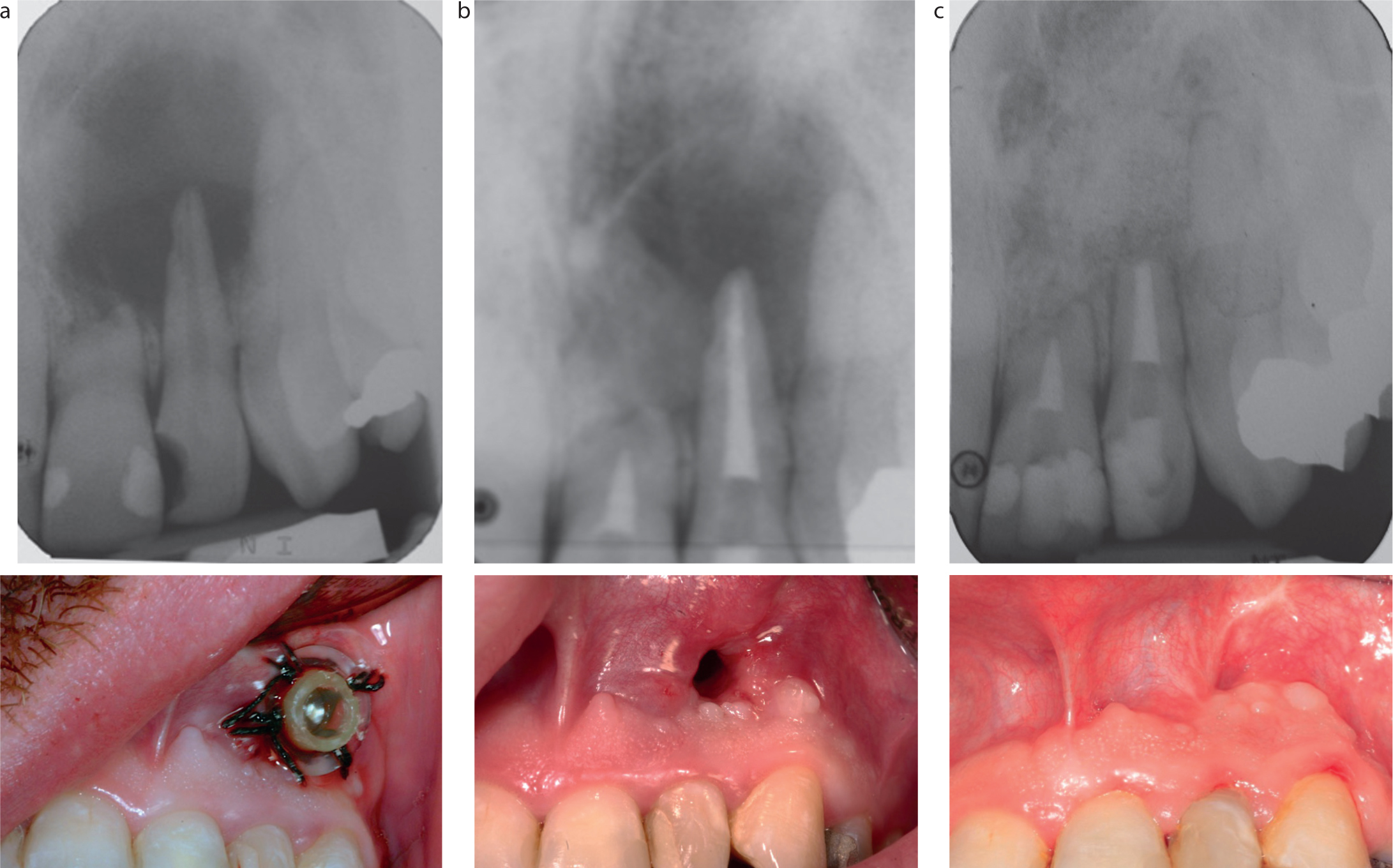
Marsupialization refers to the surgical exteriorization of a large cyst, which often necessitates the provision of a removable appliance, such as an acrylic removable obturator, following surgery. Decompression refers to drainage of a large cyst using a surgical drain secured in-place over a prolonged period and is a more common procedure than marsupialization (Figure 2). The drain acts to reduce the osmotic pressure within the cyst, which encourages collapse of the epithelial lining. This technique has been demonstrated to be an effective way of reducing the size of large lesions to a more manageable size (eg in cases that have not responded to conventional root canal treatment, or in instances where exudation into the canal space cannot be adequately controlled to allow obturation).8 The drain exit should be positioned as coronal as possible to the cyst, and ideally within the attached gingivae, to facilitate irrigation. Given the extended period that the drain will be in position, good oral hygiene is required to prevent infection. This must be demonstrated to the patient at the time of placement, and repeated at follow-up if necessary. This should include the use of a 0.2% chlorhexidine gluconate or saline solution, delivered with syringes to enable lavage of the lesion through the drain.5 Regular clinical review, with 3-monthly radiographic assessment, is recommended so that bony infill of the defect can be monitored. Regular review also facilitates the opportunity to shorten the drain as the lesion shrinks in size, and replace drains that may have become detached. Although decompression may result in complete resolution of the lesion, SRCReT is still required to enucleate any remaining lesion and remove residual micro-organisms that could contribute to a new or persistent lesion.5,8,9
Figure 2. Decompression of a radicular cyst using a modified endodontic syringe as a surgical drain. Clinical photographs and associated radiographs at (a) the start of treatment; (b) at removal 6 months later, prior to enucleation of the remaining lesion and repair of the mucosal defect; and (c) at 3-year review.
Corrective surgical procedures
Corrective surgical procedures are aimed at repairing root surfaces, modifying the anatomy of a root, or resecting either infected or damaged roots (± portion of the clinical crown). The types of problems that corrective surgical procedures can be used for can be classified into host and environmental factors (Table 3). When planning corrective surgical procedures, it is important to consider the range of possible healing outcomes, and potential impact on pulpal and periodontal health, as well as aesthetics within the anterior zone.10
Host factors
Anatomical defects:Root groovesFused teethEnamel pearls that may facilitate progression of periodontal breakdown, and may contain pulp tissue
Cervical resorption
Environmental factors
Perforations:Root canal treatment preparation errorRoot perforation with pinsRoot perforation with posts
Root fractures
Furcation involvement with associated periodontal–endodontic defect
Treatment should aim to provide an environment that facilitates regeneration of damaged periodontal tissues and long-term tooth stability. If surgical treatment is to be attempted, it is critical that a thorough pre-operative assessment is undertaken to provide a provisional diagnosis and to facilitate surgical planning. The history should probe factors that may have contributed to the presence of hard- and soft-tissue defects, such as trauma, previous orthodontic therapy and bleaching. Physical examination should aim to determine the pulpal status of the tooth and whether the defect communicates with the oral cavity.
It is important to record responses to sensitivity testing of teeth (cold/electric pulp testing) and perform a thorough assessment of periodontal pocket depths by walking a periodontal probe around the gingival sulcus of each tooth to determine whether a vertical periodontal defect is present. If deep localized pockets are identified, then a detailed full-mouth six-point pocket chart is required as a pre-treatment record to help determine whether the cause is pulpal or periodontal in aetiology. A minimum of two long-cone peri-apical radiographs should be taken, which should be exposed at different horizontal angulations using parallax. A CBCT scan could be considered when an extensive defect is suspected.11 When a communication between the root canal space and the exterior surface of the root is suspected, this can be confirmed by using an electronic apex locator, which, in the presence of a perforation, will give a ‘zero’ reading when the file passes through the perforation to contact the peri-radicular tissue. Paper points placed in the root canal may also be able to assess any bleeding points, and radiography may assess the extent and position of the defect.
Repair of cervical resorption defects and perforations
Perforations may occur because of iatrogenic damage (eg loss of orientation during access cavity preparation), the instrumentation phase of NSRCT, or poor placement of either dentine pins or posts. The perforation may act as a route for bacterial entry, resulting in both intra-radicular infection and periodontal pocketing. Repair of the defect should be attempted as soon as practicable to prevent this. Small pin-point perforations (less than 0.5 mm) apical to the gingival attachment should be treated as an additional portal of exit via conventional root canal treatment. More extensive perforations, such as post perforations, normally require either surgical intervention or extraction. The prognosis for defects repaired surgically will be dependent on various factors, such as accessibility to the perforation site (labial perforations are easier to access than palatal/lingual defects), diameter of the perforation (smaller defects have a better prognosis), time between perforation and repair (the shorter the time interval the better the prognosis), extent of bacterial contamination (infected sites have a reduced prognosis), and vertical level of perforation (perforations that communicate with the gingival sulcus have a poorer prognosis than those that do not).12 The definitive outcome for the tooth should be considered while planning any root repair, with an aim for a functional, restorable tooth with sound coronal restoration that is devoid of signs or symptoms.
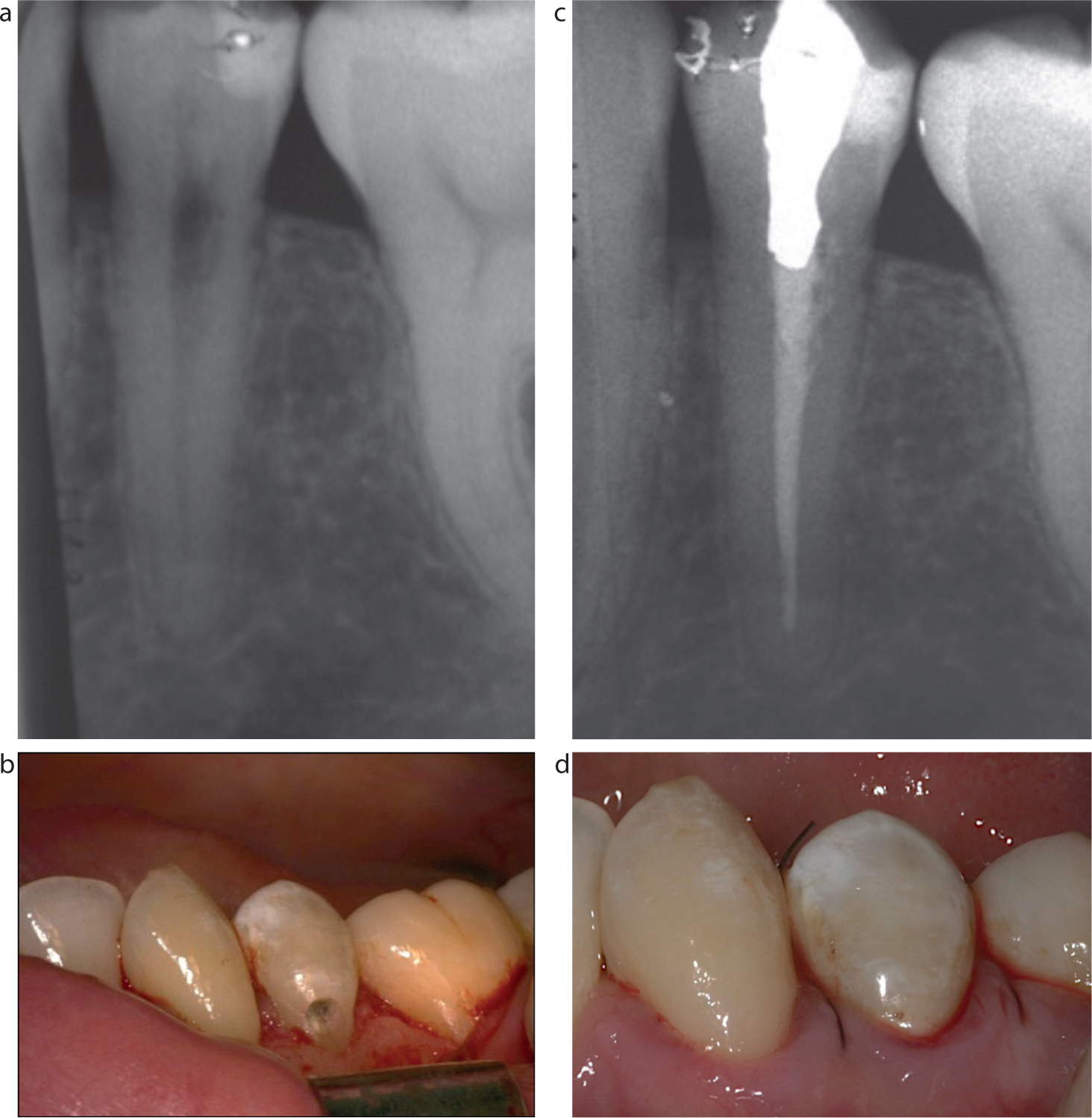
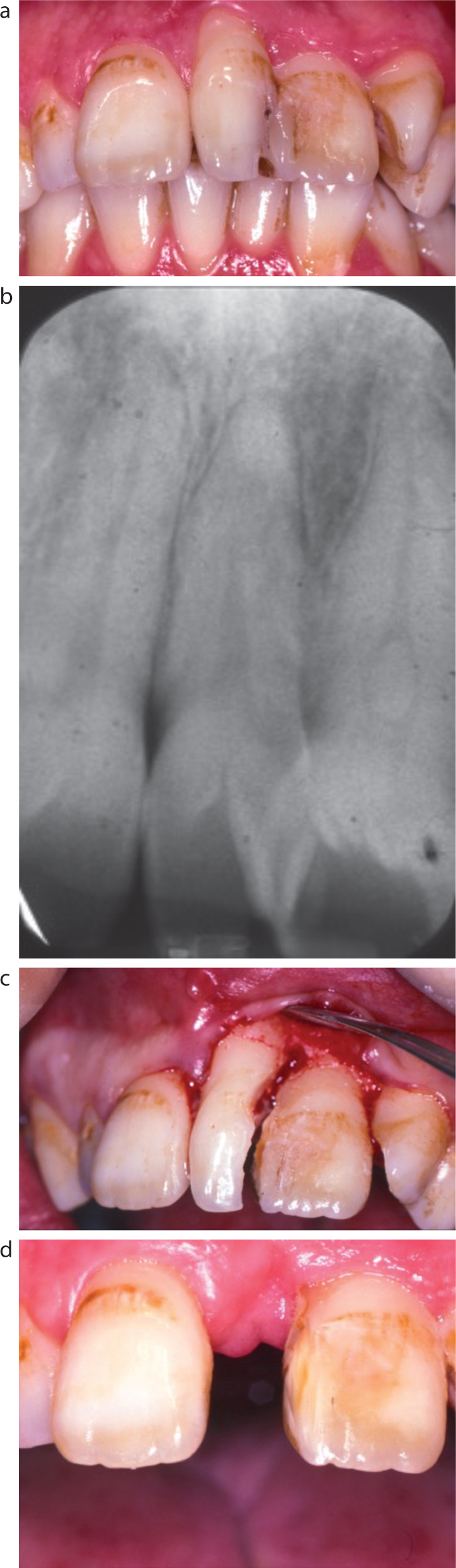
External cervical resorption (ECR) is a process that results from damage to the cementum layer and subsequent osteoclastic-like resorption of the root dentine in the region of the gingival attachment. Although the aetiology of ECR is often unclear, contributory factors may include: orthodontic treatment; dental trauma; intra-coronal bleaching; periodontal treatment; or systemic disease. A pink hue at the neck of the tooth and/or temperature sensitivity may indicate the presence of cervical resorption and should initiate further investigation by the clinician. If caught early, the lesion may be suitable for surgical repair (Figure 3). Surgical treatment should include: the elevation of a full thickness muco-periosteal flap; removal of inflammatory tissue and preparation of the defect site (using hand instruments or ultrasonics); and repair and closure (suturing) of the flap.10
Figure 3.
(a, b) Pre-operative assessment and (c, d) post-operative repair of cervical resorption defect using RMGIC.
Alternatively, inflammatory tissue and resorptive-inducing cells may be eliminated using a caustic agent such as trichloroacetic acid.13 The caustic nature of this solution poses a risk to the adjacent tissues and it is essential that adequate protection of these tissues (using glycerol) is provided during surgery.
In cases where a communication exists between the root canal and the oral cavity, repair of the defect and NSRCT are required. Sealing the perforation (to prevent irrigant leakage into the mouth and bacterial ingress during root canal treatment) non-surgically may be challenging due to the absence of any support to apply the material within the canal lumen space. This problem may be addressed by raising a muco-periosteal flap, removing any granulation tissue present, then filling the defect temporarily with a material such as IRM (Dentsply Caulk, Milford, CT, USA) or Cavit (3M, Bracknell, UK). The flap can then be repositioned and held in place with several interrupted sutures and the access cavity prepared in the tooth under rubber dam isolation. Following chemo-mechanical debridement and obturation of the root canal, the access cavity can then be sealed and the rubber dam removed. The muco-periosteal flap is raised a second time, removing the temporary restoration from the defect and completing a definitive restoration (Table 4). Cervical resorption may present late, often resulting in extensive destruction where repair is not feasible. If the lesion is level with the gingival attachment, extends over one-third of the root width or over half of the root length, the prognosis for the tooth is guarded, and extraction is often the only predictable management option.10,12 A host of materials have been studied for their use in root perforation repairs and a brief summary of their properties can be seen in Table 4.
Material
Advantages
Disadvantages
Recommended for perforation repair
Amalgam
InexpensiveEase of placement
Poor biocompatibilityPoor aestheticsDoes not bond to tooth tissue
No
Glass ionomer cement (GIC)
InexpensiveBonds to tooth tissueAcceptable biocompatibility
Susceptible to moisture loss/gain unless its surface is protected with unfilled resinLong setting time
Yes – if perforation communicates with oral cavity
Resin-modified glass ionomer (RMGIC)
InexpensiveBonds to tooth structureAcceptable biocompatibilityLong-term stability within oral cavityDual-cured
Biocompatibility inferior to MTA/tricalcium silicate cements
Yes – if perforation communicates with oral cavity
Composite
InexpensiveCommand cure
Poor biocompatibilityUnpredictable bond to tooth tissue unless optimal moisture controlPolymerization shrinkage on setting
ExpensiveNo bond to tooth structureOnly suitable for use when no communication with the oral cavity
Yes – if no communication with oral cavity
Tricalcium silicate cement (eg Biodentine)
Evidence to support biocompatibilityImproved handling characteristics compared to MTA
ExpensiveOnly suitable for use when no communication with the oral cavityUnproven long term
Yes – if no communication with oral cavity
Gutta percha
InexpensiveBiocompatible
Additional equipment required, eg a heat sourceOnly suitable for use when no communication with the oral cavityRisk of heat damage to periodontal ligament
Can be used for small perforation repairs accessible from within the root canal.Not recommended for external root repairs.
In the absence of communication between the defect and the oral cavity, mineral trioxide aggregate (MTA) promotes cementogenesis and its biocompatibility offers optimal healing when used as a root-end filling and perforation repair.7,8,14,15,16 Biodentine (Septodent, Saint-Maur-des-Fossés, France) is a tricalcium silicate cement that has shown promise as a repair material, dentine replacement and temporary restorative material due to similar biocompatibility properties as MTA.17,18 Biodentine should be covered with a definitive restoration, if exposed to the oral cavity.19
When the repair site communicates with the gingival sulcus, which commonly occurs with external cervical resorption, the material needs to be both biocompatible and resistant to the mechanical wear that may be encountered in the oral cavity. Conventional glass ionomer (protected with an unfilled composite resin layer), or resin-modified glass ionomer cement (RMGIC) are recommended in such cases because of their ability to bond directly to tooth structure, minimal leakage and adequate biocompatibility (Figure 3). RMGICs may be useful in repairing deep and narrow defects such as those encountered within developmental grooves.
Anatomical defects
Anatomical defects such as palato-gingival grooves, fused teeth or enamel pearls may require surgical access for recontouring, repair or resection. Palato-gingival grooves are rare dental developmental anomalies of the external surface of the root. They usually extend from the cingulum in an apical direction along the root surface and are most commonly associated with maxillary lateral incisors.20,21 Although the aetiology of these grooves is not fully understood, it has been suggested that the groove may represent an incomplete form of dens invaginatus, caused by in-folding of the Hertwig's epithelial root sheath.22
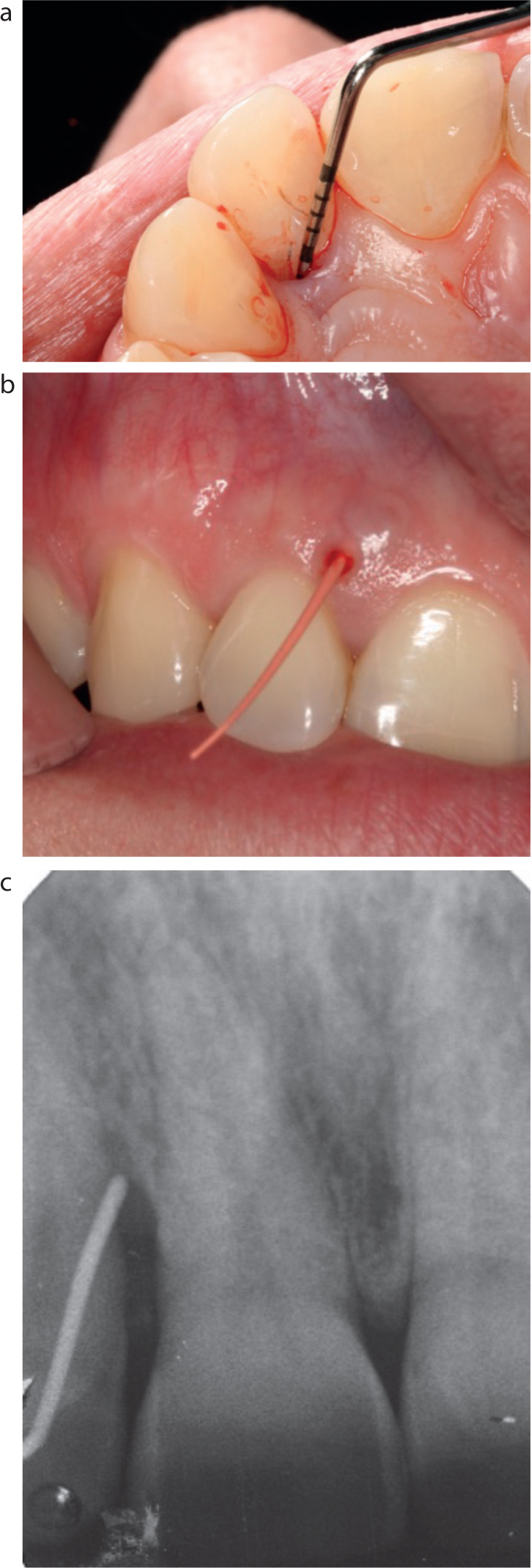
Palato-gingival grooves are rare, but may act as a pathway for bacterial ingress, potentially leading to pulpal necrosis and periodontal defects that extend to the depth of the groove. The raising of a full thickness muco-periosteal flap facilitates assessment and treatment of the groove. Treatment involves either root recontouring (the elimination of the groove using a surgical high-speed handpiece) or, in the case of deeper defects, restorative infill using GIC or RMGIC (Figures 4 and 5). Guided tissue regeneration using a membrane/bone substitute or Emdogain (Straumann, Andover, MA, USA) (porcine-derived enamel matrix derivative), may be used to regenerate periodontal defects.23 If there is pulpal involvement, NSRCT should be undertaken. Late presentation with extensive periodontal destruction may make treatment difficult or unfavourable.
Figure 4. Pre-operative photographs and radiographs of a palato-gingival groove associated with UR2 but not extending to the root apex. (a) Localized periodontal pocketing associated with the palato-gingival groove defect; (b) labial fistula with GP cone tracer and (c) radiograph demonstrating tracer in situ and base of defect.Figure 5. Intra-operative photographs illustrating the periodontal defect and groove during surgical access. (a) Full thickness flap raised with infra-bony defect UR2; (b) evidence of palato-gingival groove and (c) subsequent restorative repair with RMGIC. Periodontal probing defect reduced to 3 mm at 6-month review.
Enamel pearls and cervical enamel projections
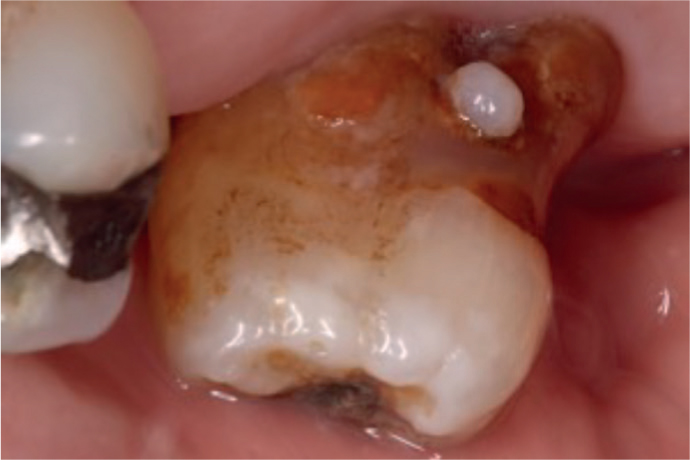
Enamel pearls are relatively rare (2–3% of permanent molars) and may be left if not associated with pathology.24 They are ectopic enamel formations that may contain dentine and pulp (composite enamel pearls), usually located in the furcation region of teeth (Figure 6).25 Enamel pearls may present clinically adjacent to isolated probing defects and are often confirmed radiographically. If exposed to the oral environment, they act as a plaque retentive feature and can predispose to periodontal breakdown. Surgical treatment aims to access the site and recontour the surface (via a surgical high-speed handpiece) until the enamel pearl is eliminated. If pulp tissue is exposed, then either vital pulp capping or root canal treatment may be required. Cervical enamel projections are most common on mandibular molar buccal surfaces and are an extension of enamel onto the root surface.26
Figure 6. Enamel pearl located at the furcation of a maxillary molar tooth.
Fused teeth
The union of two or more teeth can occur by fusion (the union of two separate tooth germs), gemination (partial division of a single enamel organ into two separate joined teeth) and concrescence (the union of two developing teeth by their cementum), though it is often difficult to distinguish between the three types. Fusion and gemination occur most commonly in the anterior regions of the jaw, with a prevalence of less than 1%.27 Division of the fused teeth will only be practical if only the crowns are fused. A CBCT scan may aid the assessment of the level of tooth fusion and help influence the decision whether to leave the teeth, recontour the clinical crowns but leave the teeth joined together, separate the teeth completely, or extract one or both of the teeth (Figure 7). Pulp therapy (capping) is often required because the pulps in the fused teeth are joined across the site of surgical division. Root canal and other treatment, such as orthodontic realignment, may also need to be employed.28
Figure 7.
(a) Pre-operative clinical photograph and (b) radiograph of two fused upper left central incisors. (c) Intra-operative photograph demonstrating complete tooth separation, resection and extraction of one of one fused central incisor.(d) Post-operative healing resulting in a midline diastema, but improved tooth
Alternatives to surgical repair of root defects
In cases of sub-gingival perforation, orthodontics may be used to extrude the tooth and perforation supra-gingivally and facilitate repair via a non-surgical approach.29 Orthodontic extrusion will result in the entire dento-alveolar complex being extruded and may require localized crown-lengthening surgery to improve aesthetics. Aesthetics in the anterior zone may be compromised by this approach, because of a reduced root width present at the cervical margin, following extrusion.
Hemi-section/root resection
Hemi-section is the vertical, surgical separation of a multi-rooted mandibular tooth into two parts through the furcation to allow removal of one root, or roots, with the associated part of the crown (Figure 8). Root section or amputation is the surgical removal of all or a portion of the root before or after endodontic treatment with the crown and tooth remaining in-situ. Dividing a tooth into three parts is termed tri-section. The main indications and contraindications for hemi-section, tri-section or root resection are detailed in Table 5. Contraindications include fused roots, bruxism, poor oral hygiene and if the remaining root/tooth is not suitable to serve as a prosthetic abutment.30
Treatment of Class II or III horizontal periodontal furcation defects
Vertical bone loss along one root of a multi-rooted tooth that is not amenable to periodontal regeneration
Severe dehiscence, clinical attachment loss or recession
Fracture or unrepairable root perforation of a multi-rooted tooth.
Unrestorable caries or a resorptive defect of one root of a multi-rooted tooth that is not amenable to non-surgical or surgical repair.
Root canal treatment not possible or has been unsuccessful on one root of a multi-rooted tooth and is not amenable to non-surgical treatment.
Figures 8. Hemi-section of a first mandibular molar tooth, leaving the mesial root intact. (a) Pre-operative clinical photograph and (b) radiograph of a molar tooth with a very severe localized infra-bony defect of the distal root and (c) following completion of NSRCT. Clinical photographs demonstrating (d) intra-sulcular incisions and (e) sectioning of the tooth through its furcation. (f) Post-operative clinical photograph of the mesial root coronal preparation and (g) post-operative radiograph prior to restoration with (h) an indirect crown.
Success rates for root resection are varied, with 10–12-year survival outcomes ranging between 32% and 92%.31,32,33,34 Meta-analysis of 19 studies showed a cumulative survival of hemi-section and root section procedures of 85.6%.35 Causes of subsequent failure include caries, root fracture, coronal restoration fracture, periodontal disease, endodontic failure and poor surgical technique.31,32,33,34,35,36,37
As with all types of surgery, thorough pre-operative assessment is required with specific examination to include: prognosis of individual roots (endodontic/periodontal), access for cleaning, occlusal loading, definitive restoration and importance of the tooth within the dentition. Root resection of the distal root of a terminal mandibular tooth leaving the mesial root intact may have a lower success rate (75% at 15 years) when compared to other molar teeth.37 Tri-section can be performed on maxillary molars, when furcation involvement is present, leaving the portion of the tooth that offers the best restorative prognosis.
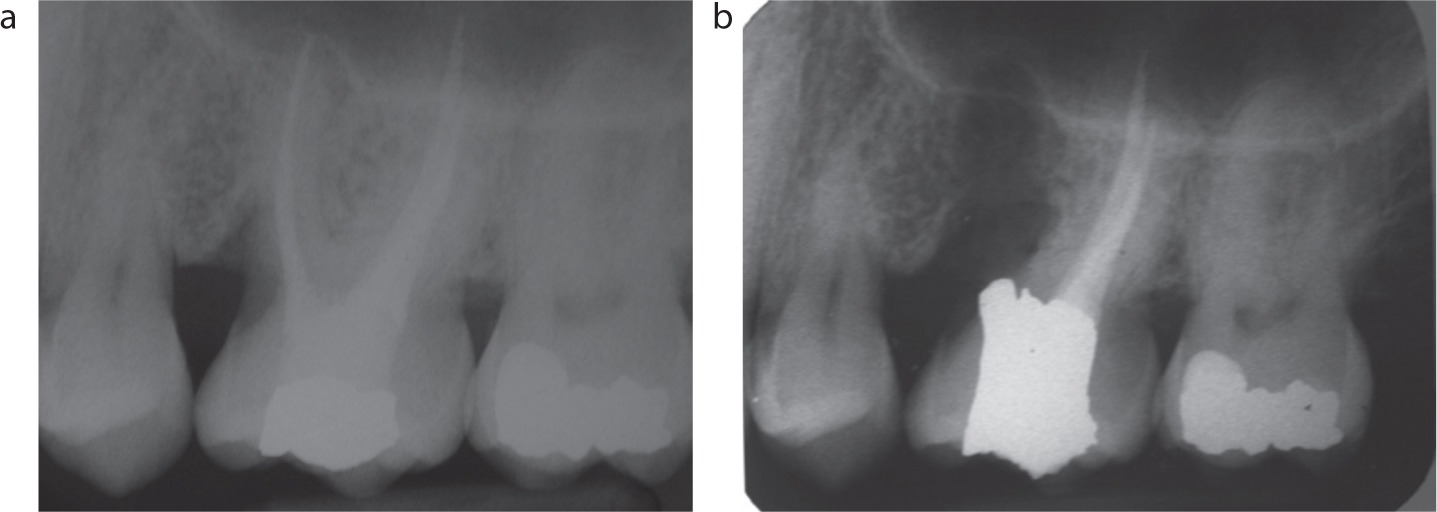
Root resection adopts a similar approach, removing one or more roots, but leaving the crown of the tooth intact. NSRCT is required prior to resection, even in the presence of a viable pulp, to prevent root canal contamination. In root-treated teeth, the technical quality of the root filling determines whether root canal re-treatment is required as a precursor to surgery (Figure 9). The core material (amalgam or composite resin) should extend into the whole pulp chamber in the case of hemi-section or tri-section, and into the root canal when planning for resection (apical to the proposed level of root resection). Proceeding in this way ensures that an amalgam or composite resin seal is present following tooth/root division. No overhangs of dentine that may impair plaque control, should be present.36 Cutting through roots should be undertaken using a high-speed fissure bur, with sufficient cooling to avoid overheating of the dentine and bone, followed by polishing to remove any surface roughness.36 Following surgery, the patient should be given oral hygiene instruction using interproximal brushes, and advised to clean between the teeth/accessible root surfaces on a daily basis to prevent periodontal disease. The patient should also be advised to use a toothpaste with a high fluoride content to prevent root surface caries.
Figure 9. Example of a mesio-buccal root resection of a maxillary first permanent molar tooth with crown left intact. (a) Pre-operative and (b) post-operative radiographs.
Intentional replantation
Intentional replantation is the extraction and surgical treatment of a tooth such as root-end surgery or perforation repair, followed by re-insertion into its socket. It is only performed when conventional surgery is not possible and other restorative options are not feasible (eg the roots are in close proximity to important anatomical structures, access is poor or dental implant placement is not possible due to the age of the patient). Although high success rates are reported for intentional transplantation,38 the patient should be informed that failure, due to resorption, is possible.39 The development of better surgical protocols has allowed replantation to be more widely considered.38 Successful replantation relies on extracting a tooth with minimal force using periotomes so that periodontal ligament damage is minimized. Although curettage of any apical lesion is advised, there should be minimal instrument contact with the socket walls. Following extraction, the tooth root should be protected with saline-soaked gauze to prevent the dehydration and death of periodontal ligament cells while the corrective procedure is undertaken. Root-end or perforation repair procedures should follow conventional protocols discussed within these papers. Well-planned treatment that results in fast replantation and flexible splinting of the tooth, with a minimum of time spent extra-orally (ideally under 10 minutes), undertaken by an appropriately trained dentist, is essential in reducing complications, such as the risk of resorption.40
Summary
The scope of endodontic surgery is broad, including techniques for both emergency and definitive treatment. The majority of the endodontic surgery literature relates to the management of peri-radicular infection, while there is less in the way of evidence/guidelines for practitioners in terms of other surgical protocols for those techniques mentioned. In Part 2 of this two-part series, root-end surgery is reviewed with suggestions for best practice for SRCReT, with inferences drawn to assist with other endodontic surgical procedures.