Complete dentures: designing occlusal registration blocks to save clinical time and improve accuracy Mark Bishop Tony Johnson Dental Update 2025 42:3, 275-281.
Authors
MarkBishop
BDS, (VU Manc) MMedSci (Sheff)
Clinical Teacher, Academic Unit of Restorative Dentistry, School of Clinical Dentistry, University of Sheffield, Claremont Crescent, Sheffield S10 2TA, UK
Senior Lecturer, Academic Unit of Restorative Dentistry, School of Clinical Dentistry, University of Sheffield, Claremont Crescent, Sheffield S10 2TA, UK
The techniques described in this article are based on facial measurements and an analysis of the patient's existing dentures to provide measurements that will enable registration blocks to be constructed for individual patients rather than the arbitrarily produced block more commonly seen. Employing the methods shown will lead to a saving in clinical time and contribute to a more accurate registration. It is important to remember that the technician can only provide occlusal registration blocks of the appropriate dimensions if the clinician has assessed the patient and existing dentures and then passed this information to the laboratory.
Clinical Relevance: Being able to assess the clinical suitability of a patient's existing dentures and then take measurements from those dentures will allow occlusal registration blocks to be constructed that have the correct dimensions and anatomical features for a particular patient. This will save time during the registration stage and help to improve accuracy.
Article
There are two vertical dimensions in occlusion: one when the teeth are in occlusion, the other when the teeth are separated and the mandible is in the rest position.1 These are referred to as occlusal face height (OFH) and rest face height (RFH), respectively, the difference between the two being free-way space (FWS). The work in this article concerns registering the first position (OFH) and describes how previous dentures and individual patient measurements can be used in the construction of occlusal registration blocks (ORBs) to enable this to be accomplished.
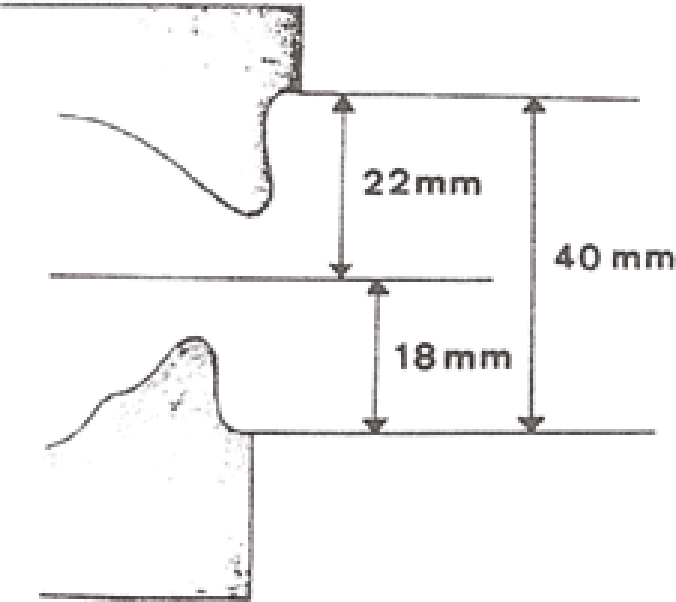
McGrane2 measured many hundreds of adult dentate models and concluded that, provided the mandibular teeth were not worn, they would measure 18 mm from the labial mucosal fold immediately beside the mandibular labial fraenum to the incisal edges of the mandibular centrals (using a model cast from a mucostatic type impression). His maxillary measurement was 22 mm, using corresponding sites, giving a total distance of 40 mm (Figure 1). Such work has been repeated by others.3,4,5,6,7
Figure 1. Mean height measurements of occlusal registration blocks (as recommended in the literature).
Ellinger,8 in a radiographic study of 50 patients, found the height in the maxilla to be 20 mm, with a range of 17.3–23.9 mm. In the mandible the mean measurement was 16.3 mm with a range of 13–19.6 mm. Ellinger et al9 recommended heights of 24 and 20 mm in the maxilla and mandible, respectively, while Stananought10 suggested 20 and 18 mm. Johnson and Winstanley11 examined 414 pairs of ORBs coming into a hospital clinic from both hospital and commercial laboratories. They found that the mean maxillary block height before registration was 21.4 mm (SD 3.5 mm) and 18 mm (SD 3.2 mm) after registration. The mean mandibular block height was found to be 17.6 mm (SD 2.5 mm) before and 14.3 mm (SD 2.8mm) after registration. The heights of these blocks, before registration, were the same as those recommended in the literature.2,3,4,5,6,7 However, these blocks were each found to be 3–4 mm too high.
In the mouth, ORBs are adjusted by the clinician to be parallel to the alar-tragal line or Campers line. This line passes through the inferior border of the ala of the nose and the superior border of the tragus of the ear, and is approximately parallel to the occlusal plane of the natural teeth.12 If the technician is able to produce ORBs which correspond, as much as possible, to these dimensions and anatomical angles, the registration process will be easier, quicker and more accurately carried out.
Occlusal registration block measurement determination and construction
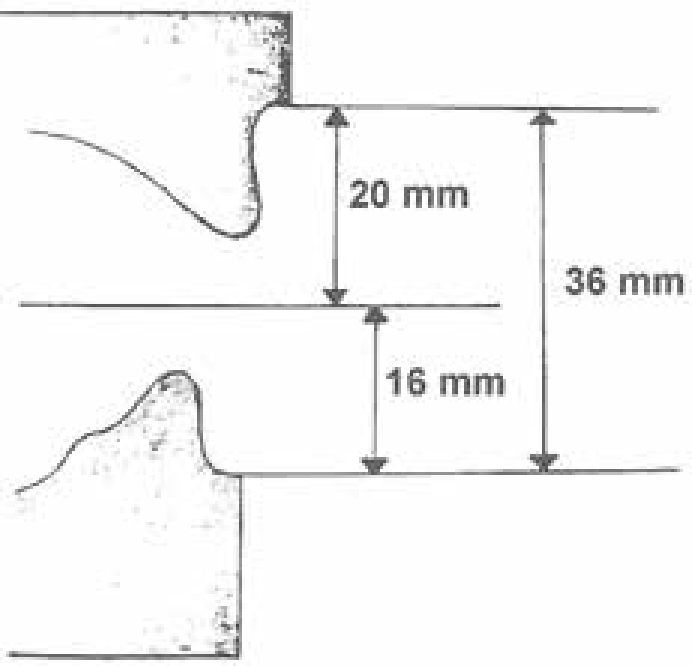
If the patient has no previous dentures then average anterior height measurements can be used to construct the ORBs. These have commonly been 22 mm in the maxilla and 18 mm in the mandible. Based on the findings by Johnson and Winstanley,11 who found that the average anterior heights of ORBs after registration were 18 mm (maxilla) and 14 mm (mandible) and, based on the premise that it is easier to remove wax than to add it, perhaps more realistic average ORB heights should be 20 mm (maxilla) and 16 mm (mandible) (Figure 2).
Figure 2. More realistic anterior height measurements for occlusal registration blocks.
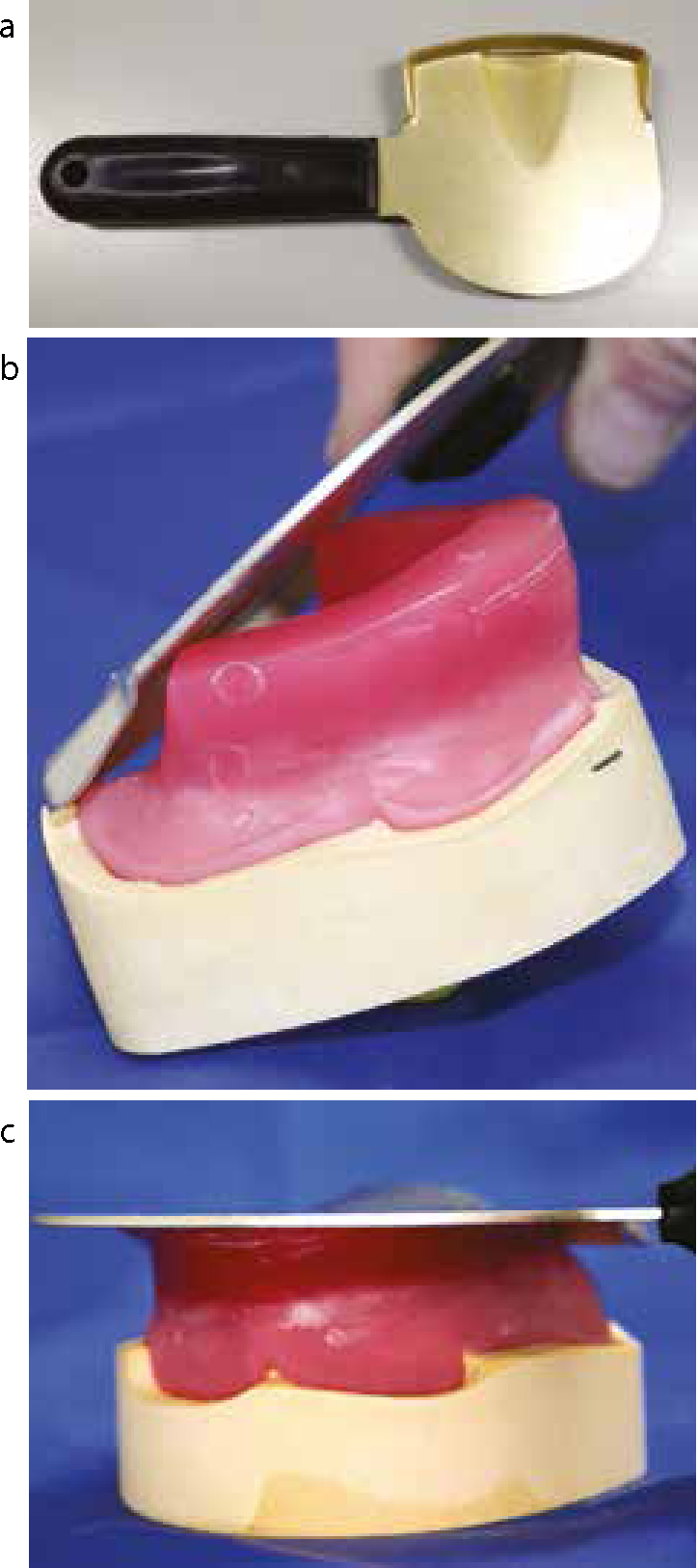
To produce occlusal registration blocks to average dimensions the anterior height of the maxillary block is marked (Figure 3), the use of an occlusal rim inclinator (Figures 4a, b, c) will then create an average alar-tragal slope onto the maxillary block, compared to the usual level block more normally provided (Figure 5). The mandibular block is extended from the 16 mm anterior height at the front to two-thirds of the way up the retromolar pads at the back, this representing the position where most mandibular dentures are extended to (Figure 6). Appropriate freeway space determination (by subtracting occlusal vertical dimension from resting face height (RFH-OVD)) should be carried out before ORBs are constructed, and can assist in more appropriately dimensioned ORBs being constructed. Systems exist, using papillameters, alameters and alma gauges, to enable this information to be used in ORB design and construction.13
Figure 3. The required average height of the maxillary block is measured and marked.Figure 4.
(a) The occlusal rim inclinator. (b) The occlusal rim inclinator is heated and the back edge placed across the hamular notches. (c) The occlusal rim inclinator is then closed onto the wax rim and, keeping the back edge in contact with the hamular notches, is closed onto the wax rim, melting the wax away until the required anterior block height is reached.Figure 5. The block on the right has been constructed using an occlusal rim inclinator and an antero-posterior slope created to be parallel to the ala-tragal line.Figure 6. Excess wax is removed to create the correct anterior height and antero-posterior relationship for the mandibular block. This is from the required anterior height to two-thirds of the way up the retromolar pads. The excess wax can be removed with a hot wax knife or the hot plate of the occlusal rim inclinator.
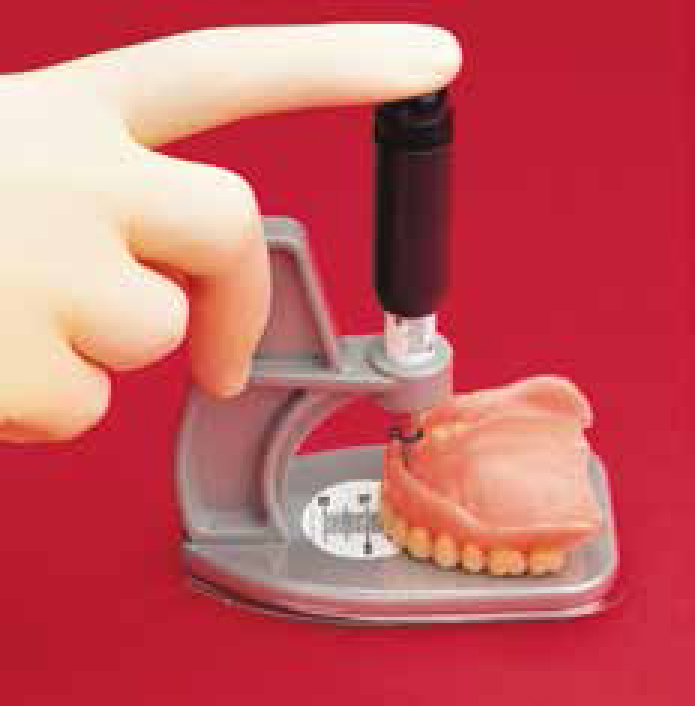
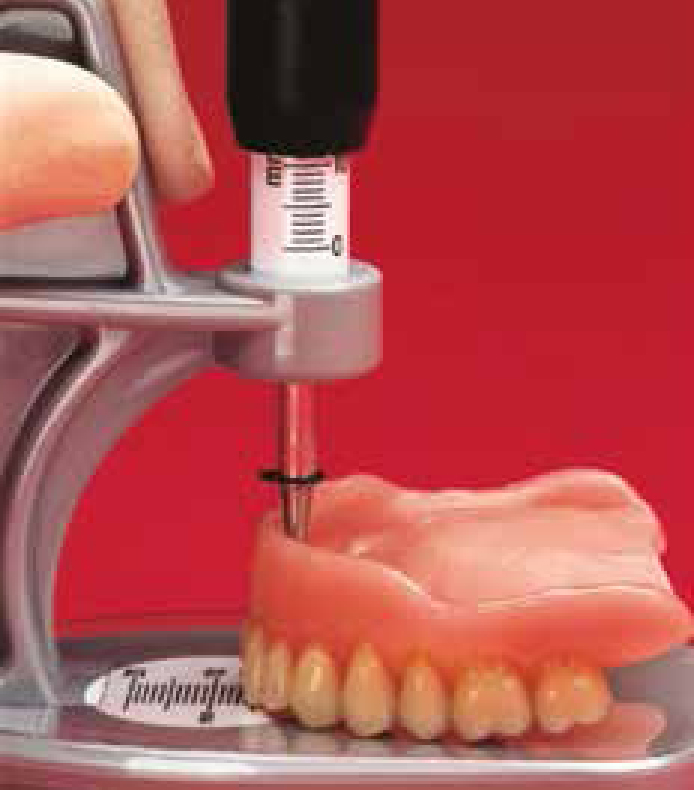
If previous dentures exist, and a thorough clinical assessment of these and the patient has been made, it will be possible to personalize the ORB measurements to that of the particular patient. The use of an alma gauge (Figure 7) will enable the height and labial position of the maxillary anterior denture teeth to be recorded; this can also be carried out on the lower denture. Always ensure the alma gauge is properly calibrated (set to zero when fully pressed down) before making any measurements. The alma gauge is used for the maxillary denture as follows:
Figure 7. The alma gauge measuring the anterior height and labial extension of an existing denture.
Place the disposable shield on the alma gauge base;
Place the denture on the base with the anterior teeth facing towards the vertical arm;
Position the stylus point to be contacting the centre of the incisive papilla in the denture base by pushing down the black stylus handle (Figure 7);
Read the number on the vertical scale below the stylus handle (Figure 8);
Take the horizontal reading where the incisal edge of the incisor teeth rest on the base (Figure 7);
With the stylus point in position draw the outline of the denture onto the shield using a permanent marker pen to record the position of the teeth around the arch. Add the vertical and horizontal readings onto the shield ready for transfer to the laboratory (Figure 9).
Figure 8. Mandibular denture anterior height and labial extension can also be recorded.Figure 9. The labial and buccal extensions of existing dentures can be recorded and copied into the occlusal registration blocks.
For the mandibular denture proceed as for the maxillary denture (Figure 10), with the stylus point of the alma gauge positioned in the centre of the fitting surface of the denture in the midline.
Figure 10. The lower denture dimensions can also be recorded using the alma gauge.
Any increase in vertical dimension and labial support, to take into account any wear on the existing dentures or to decrease/increase the amount of free-way space or lack of lip support, can then be built into the measurements from the alma gauge readings. The technician can then use the alma gauge and any additional increases/decreases to produce an occlusal registration block that should be as near to the correct dimensions as possible (Figure 11). Once again, using an occlusal rim inclinator will create an average alar-tragal slope onto the maxillary block.
Figure 11. The technician can use the alma gauge readings to construct the registration blocks to the dimensions and extensions required for a particular patient.
Other areas that are poorly designed and can cause problems during the registration are the widths of the ORBs. Over wide ORBs can restrict the tongue space and encroach into cheek and lips, creating a distortion of the denture-bearing area and lead to movement of the ORBs and an inaccuracy during the registration. ORB widths are normally chosen arbitrarily by the technician, or sometimes to be in the range of 5–7 mm anteriorly and 7-8 mm posteriorly. A more logical approach would be for the technician to draw onto the model the width of the first molar tooth and a central incisor in their expected positions and then draw ‘tramlines’ down either side to get a reasonable estimation of the required occlusal registration block width (Figures 12 and 13). The ORBs obviously need to meet in the mouth but in general need not be much wider than the teeth that they will eventually carry.
Figure 12. The width of molar and incisor teeth are drawn onto the model and lines drawn down either side to give an indication of occlusal registration block width and position.Figure 13. The ‘tramlines’ can then be used to give guidance as to the position and width of the occlusal registration blocks.
Often, the occlusal aspects of the wax rims extend too far distally. The base of the ORB should extend to cover the retromolar pads. However, the wax rims should only extend as far as the first molar, to a height level of two-thirds of the way up the retromolar pads (Figure 14); any further and the clinician has more wax to adjust than is really necessary, which may pose problems in inexperienced hands. The ‘Manchester rim’, introduced by McCord and Grant,13 reduces the mandibular wax rim even further to extend from the 1st premolar to the 1st molar region only, reducing the amount of first contact area for adjustment.
Figure 14. Mandibular and maxillary registration blocks need not extend further back than the first molar position.
The provision of finger rests in the occlusal/buccal surfaces in the second premolar regions of the mandibular ORB will enable the clinician to control and seat the mandibular ORB more precisely during the registration process (Figure 15 a, b). As the mandibular ORB is usually the more difficult of the two blocks to keep seated, this can be a useful feature for the technician to build into the block during construction.
Figure 15.
(a) Finger rests, built into the occlusal/buccal surfaces of the blocks by the technician (also see Figures 7 and 12), will enable the clinician to have better control over the mandibular block during the registration process. (b) Finger rests allow firm control of the mandibular block with fingers in the rests and under the patient's chin.
Discussion
This basic aspect of ORB production is very often constructed with no anatomical or scientific methodology behind it. This leads to an increase in clinical time and the potential for inaccuracy.
The techniques described will only add a small amount of extra technical time, but with no increase in cost to the construction of the ORBs, and it will require the clinician to spend a small amount of time making the initial OFH-RFH-free-way space determination, taking the alma gauge readings, assessing previous dentures and identifying any increases in height or labial contour increases required. However, this will undoubtedly save the clinician chairside time during the registration stage and lead to higher levels of accuracy.