Nunn JH, Carter NE, Gillgrass TJ The interdisciplinary management of hypodontia: background and role of paediatric dentistry. Br Dent J. 2003; 194:(5)245-251
Carter NE, Gillgrass TJ, Hobson RS The interdisciplinary management of hypodontia: orthodontics. Br Dent J. 2003; 194:(7)361-366
Pjetursson BE, Tan WC, Brágger U A systematic review of the survival and complication rates of resin-bonded bridges after an observation period of at least 5 years. Clin Oral Implants Res. 2008; 19:(2)131-141
Pjetursson BE, Brágger U, Lang NP Comparison of survival and complication rates of tooth-supported fixed dental prostheses (FDPs) and implant-supported FDPs and single crowns (SCs). Clin Oral Implants Res. 2007; 18:97-113
Ibbetson R. Clinical considerations for adhesive bridgework. Dent Update. 2004; 31:(5)254-260
Durey KA, Nixon PJ, Robinson S Resin bonded bridges: techniques for success. Br Dent J. 2011; 211:(3)113-118
Ibrahim AA, Byrne D, Hussey DL Bond strengths of maxillary anterior base metal resin-bonded retainers with different thicknesses. J Prosthet Dent. 1997; 78:(3)281-285
Alani A, Bishop K, Djemal S, Renton T.: RCS Clinical Guidelines; 2012
Fudalej P, Kokich VG, Leroux B. Determining the cessation of vertical growth of the craniofacial structures to facilitate placement of single-tooth implants. Am J Orthod Dentofacial Orthop. 2007; 131:S59-67
Bernard JP, Schatz JP, Christou P Long-term vertical changes of the anterior maxillary teeth adjacent to single implants in young and mature adults. A retrospective study. J Clin Periodontol. 2004; 31:(11)1024-1028
Jepson NJ, Nohl FS, Carter NE The interdisciplinary management of hypodontia: restorative dentistry. Br Dent J. 2003; 194:(6)299-304
Hypodontia: aesthetics and function part 2: management Richard Holliday Nichola Lush Jonathan Chapple Francis Nohl Ben Cole Dental Update 2025 41:10, 891-898.
Authors
RichardHolliday
BDS(Hons), MFDS RCS(Ed)
Academic Clinical Fellow/Specialty Registrar in Restorative Dentistry
Patients with hypodontia present clinical challenges in relation to function and aesthetics. In this two part series we will explore the clinical features of hypodontia (part 1) and will move on to discuss the interdisciplinary management of hypodontia (part 2).
Clinical Relevance: Hypodontia can cause functional and aesthetical concerns. This paper discusses the interdisciplinary management of hypodontia. Dent Update 2014; 41: 891–898
Article
Hypodontia is a complex dental condition that can have significant effects on aesthetics and function, as discussed in the first paper of this series. Hypodontia requires an interdisciplinary management approach. This paper will review the management options.
Interdisciplinary management
In order to provide patients with the most aesthetically pleasing and functional outcome, an interdisciplinary approach to management may be required. The role and aims of the team has been previously described by Nunn et al.1 In summary, the aims are:
Complex cases may involve the expertise of a number of specialties which include orthodontics, paediatric dentistry, restorative dentistry and oral surgery, whereas milder cases may be treatable by a single specialty alone. As a result, patients are treated on a case-by-case basis.
Hypodontia management
The treatment options for patients suffering from hypodontia are essentially the same as those for replacement of any other missing teeth, namely:
Removable prosthesis;
Conventional or adhesive bridgework;
Auto-transplantation; or
Implant-supported prosthesis.
Of course, there are specific considerations in hypodontia cases which we will consider.
Space management
Spacing is often present in hypodontia cases and a midline diastema can be present due to distal movement of the central incisors when lateral incisors are absent or microdont, or because of the diminutive morphology of the central incisors themselves. Spacing is usually managed during the orthodontic phase of treatment but, if a non-orthodontic plan is chosen, this may have to be addressed by restorative options. This would usually involve either resin composite augmentations (Figure 1) or crowns/veneers designed to minimize the spaces. Spacing in the posterior dentition is often of little concern.
Figure 1.
(a–c) A case of hypodontia and spacing restored by restorative means alone. The spaced and microdont maxillary incisor teeth were augmented with resin composite to improve their appearance and reduce the spacing. The final restoration included a partial mandibular and maxillary denture with onlay aspects on the maxillary arch.
When orthodontics is used to manage spacing, a dilemma often faced is that of whether to open or close spaces. Each case should be judged on its own merits, but factors such as patient's age, skeletal relationship, the severity of hypodontia, the degree of crowding and the feasibility of desired tooth movements should be considered.2 It is also important to consider patient expectations and commitment to treatment. Although the ideal age for definitive orthodontic treatment is early adolescence, selected removal of primary teeth may be beneficial at an earlier stage.2 An early orthodontic opinion is desirable, particularly in the more severe cases of hypodontia.
Space closure may be appropriate in mild cases and has the advantage of avoiding the need for tooth replacement and the long-term maintenance associated with this. It may preclude the need for any restorative treatment. Space closure may, however, be slow and full closure difficult to achieve given that this group of patients generally have diminutive teeth.2 Relapse is also a concern.
Missing lateral incisors
A common scenario is the absence of the maxillary lateral incisor and this is worth considering specifically owing to its common nature and aesthetic implications. If hypodontia is limited to the lateral incisors, then general treatment strategies include opening or closing the lateral incisor space.
Space opening
Space opening and redistribution may result in optimal aesthetics and, from a functional aspect, canine guidance is more achievable. However, it should be explained to patients and carers that any prostheses will require a life time of maintenance.2
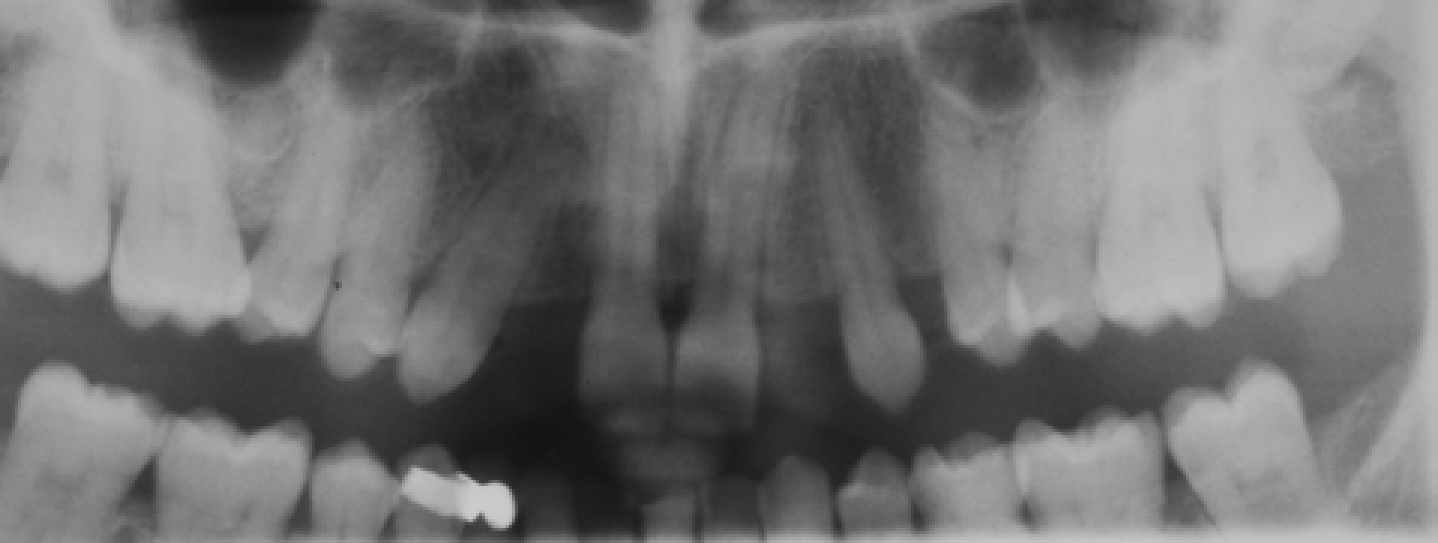
If the lateral incisor space is maintained (or opened if it has partially closed) then restorative options generally include resin-bonded bridges (RBB) or dental implants. If dental implants are to be considered, there should be sufficient inter-root space between the central incisors and canines with correction of any mal-aligned teeth (Figure 2).
Figure 2. Panoramic radiograph demonstrating insufficient inter-radicular space for implant placement in the lateral incisor sites.
Space closure
It may be desired by the patient that the lateral incisor space is closed, leaving the canine adjacent to the central incisor. The aesthetic result achieved from this can vary enormously. Canines are more pointed and often appear darker compared to lateral incisors. The canine can be masked to resemble a lateral incisor, ‘lateralization’. This usually involves modifications in form and colour. Tooth reduction is often completed to remove the incisal tip and proximal enamel to produce more vertical interproximal contacts. Resin composite can be added to the mesial and distal incisal corners to help improve the form. Care should be taken not to expose dentine as this can result in darker shades which can compromise the aesthetics.2 Canines often have a higher chroma than other anterior teeth and localized vital bleaching can help improve this. The smile level and gingival contour should be considered when choosing this treatment option with the gingival position of canines usually being more apically positioned (Figure 3). Excellent results can be achieved with the benefit of little or no long-term maintenance requirements. However, careful planning is required as not all canines are suitable, leading to a less than ideal final result. In summary, the shade, tooth form, gingival level and smile level should all be considered.
Figure 3. Case demonstrating disparity of gingival levels between maxillary canines and central incisors. In this middle-aged patient an adhesive bridge and removable denture have been used to restore the spaces posterior to the canines.
The decision in these cases of whether to open or close spaces relies on combined orthodontic and restorative expertise. There are several factors to consider and this includes the complexity of the orthodontics required and whether this can be treated in primary care by a specialist or hospital-based care. Timing of visits is also important, for example when should the patient be seen jointly by the interdisciplinary team or separately and by which specialties? It can also be useful for the restoring clinician to review the patient prior to orthodontic debond.
An alternative treatment strategy could include a minimal intervention technique, accepting the spacing. Spaces could be partially or completely closed with resin composite augmentations or veneers. A diagnostic wax-up would be particularly useful in this situation.
Interim options in the developing dentition
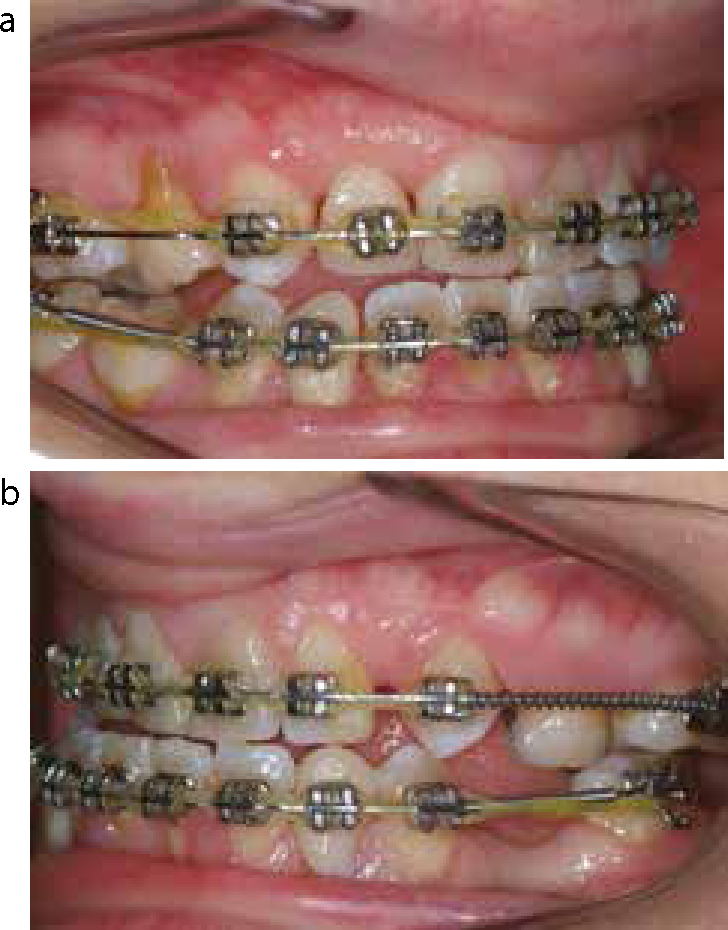
During the teenage years aesthetic issues can be of increasing concern and it is often necessary to provide interim restorations. A removable partial denture can provide the necessary aesthetics and functional requirements when hypodontia is severe. During orthodontic treatment, when spaces are being opened, it is possible to add prosthetic teeth to the fixed appliance and then subsequently to the retainer (Figure 4).
Figure 4.
(a, b) Prosthetic teeth incorporated into fixed orthodontic appliance (UR2, LL3, LR3 positions).
In young children with severe hypodontia and microdont teeth, intervention is often considered for the aims of providing function, maintaining the vertical dimensions and addressing aesthetic concerns. In reality, compliance frequently dictates the treatment provided.
Removable prosthesis
Although often not the treatment option of choice, a removable prosthesis has an important role to play in the restoration of hypodontia patients.
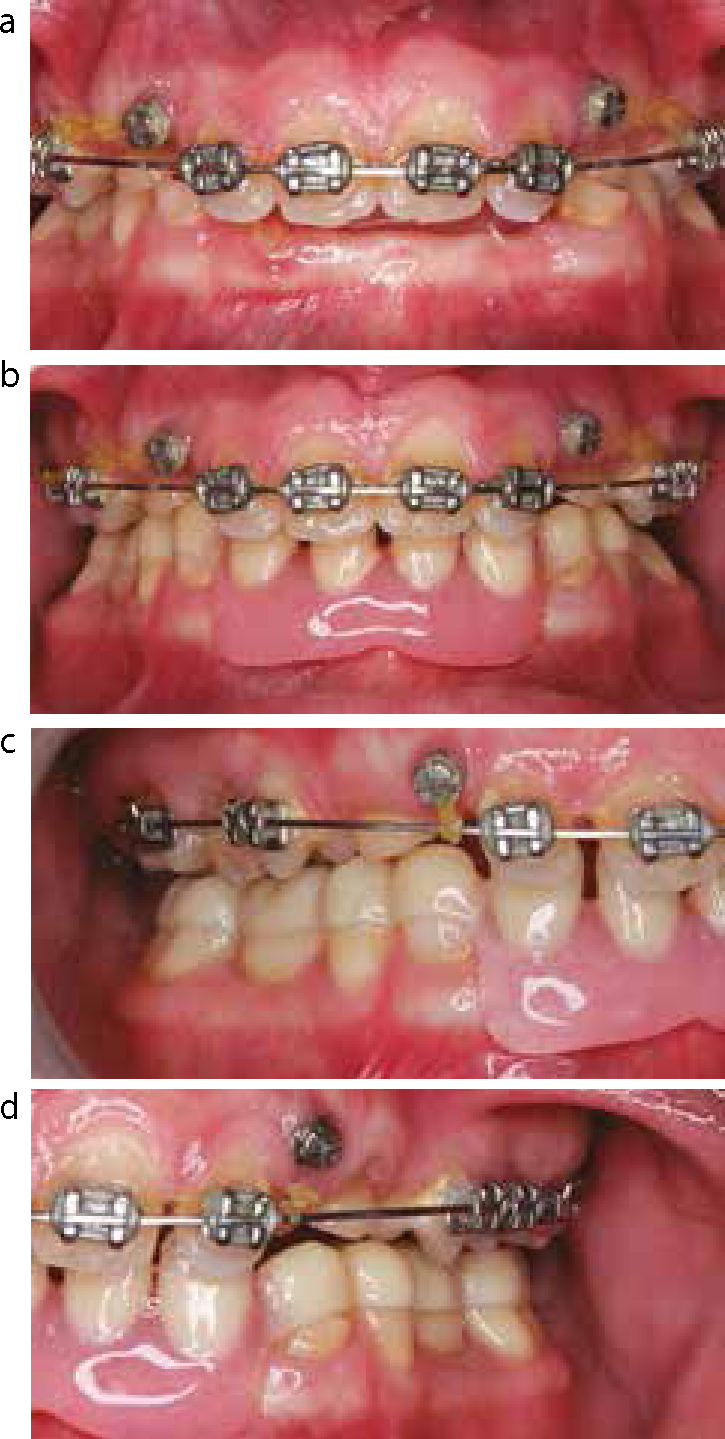
It can provide a simple and relatively quick option for the restoration of function and aesthetics. A simple mucosal borne or overlay partial denture can be used to restore face height and act as a space maintainer. Acrylic allows adjustments as teeth erupt and alveolar growth occurs (Figure 5).
Figure 5.
(a–d) An overlay partial denture to restore aesthetics during orthodontic treatment.
Resin-bonded bridge (RBB)
Resin-bonded bridges provide an excellent treatment option in hypodontia cases owing to their minimally invasive nature, short treatment time and relatively low cost. Younger patients have large pulps and higher risks of loss of vitality during conventional crown preparation and hence minimal or non-preparation RBBs are preferable. Young patients also often have social factors (school, exams, university) which preclude complex and time-consuming treatment options, such as dental implant placement, which can take numerous visits over 12–18 months. In addition, implant placement in younger patients is contra-indicated until alveolar growth is complete.
A recent Cochrane systematic review estimated the five-year survival of resin-bonded bridges to be 87.7%, with the most common complication being ‘loss of retention’ (debonding).3 This compares to 93.8%4 for conventional fixed bridges.
Despite the advantages of resin-bonded bridges, it is important to appreciate that there are specific challenges in their provision in hypodontia patients. These include short clinical crown height or microdont teeth leading to reduced bonding area being available. Crown lengthening surgery can increase the bonding area and can be either conventional periodontal flap surgery or electrosurgery, depending on the anatomy of the periodontium. Electrosurgery can be particularly useful in cases where there has been gingival hyperplasia following orthodontic treatment.
Good framework designs should have several features.5 The retainers should cover as much of the abutment tooth as possible, increasing the surface area for bonding (Figure 6). The retainer should extend into proximal surfaces of the abutment tooth as much as possible to enhance retention and resistance form. Opinions are divided regarding ‘preparation or no preparation’.6 The benefits of preparation are that retainer wings can have adequate thickness without interfering with occlusion. Thicker wings are more rigid with less stress being placed on the cement lute and hence are potentially less likely to debond. Frameworks should have a thickness of at least 0.7 mm7 and connectors should have heights of at least 2 mm.5 Incorporation of occlusal rest seats helps axial loading and adds to framework rigidity. Depending on occlusal space, these may or may not require tooth preparation.
Figure 6. Resin-bonded bridges utilizing all of the bonding area available.
Disadvantages of the preparation technique are that it is irreversibly damaging to the tooth and often exposes dentine, which can lead to sensitivity but also produces a poorer bond strength compared to enamel. In children, there is rarely a need to prepare teeth for bridgework.
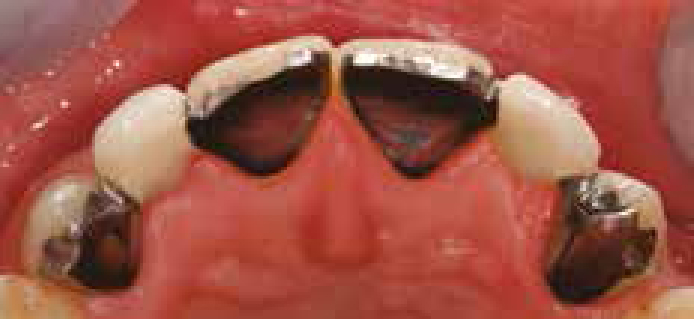
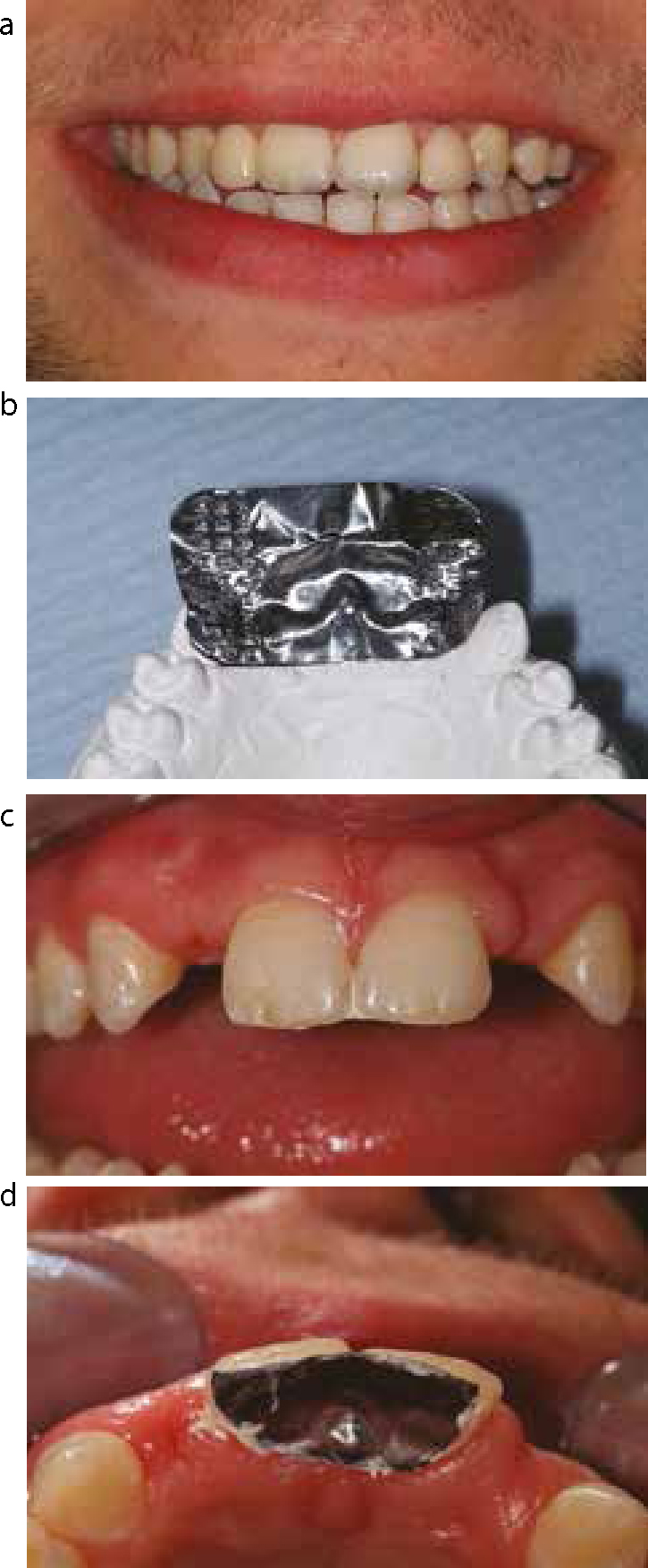
Resin-bonded bridge retainer wings can sometimes subtly alter the shade of the retainer tooth, depending on the transparency/thickness of enamel and dentine (Figure 7). A useful technique to identify potential shade alterations to the patient and aid shade determination of the restoration is to apply a layer of foil (from an x-ray film) carrying a white paste, such as zinc oxide paste, as demonstrated in Figure 8. However, opaquing cements such as Panavia F (Kuraray, Osaka, Japan) can be useful in reducing the metal shine through in some cases.
Figure 7.
(a, b) Grey shine through from bridge retainer wings.Figure 8.
(a–d) Predicting grey shine through using foil technique.
Conventional bridges
Conventional bridgework can be a treatment option for the restoration of missing teeth in hypodontia patients; however, this is often best avoided, especially in young patients, owing to potential pulpal complications. In cases of associated microdontia, however, the diminutive crown may already resemble a crown preparation and a conventional bridge may be the most predictable treatment option. There should also be consideration for maintenance implications. Figure 9 demonstrates a case where conventional bridges have been utilized.
Figure 9.
(a, b) Case demonstrating conventional bridges in a case of severe hypodontia. The preoperative and post-preparation views are shown. A dental implant was placed in the UR3 position and restored as a single unit.
Implants
Dental implants are increasingly becoming the ‘gold standard’ treatment for missing teeth with improvements in biomaterials technology and accessibility. Dental implants are particularly attractive in hypodontia cases, avoiding the use of teeth as bridge abutments, maintaining natural interdental spaces, and can be particularly useful in a spaced and microdont dentition in which adhesive bridgework is challenging.
Patients suffering from hypodontia may qualify for dental implants to be placed by the National Health Service(NHS).8 However, dental implants are not always the best restorative solution. Patients should be fully aware of potential complications which can include osseointegration failure, the need for bone grafting prior to placement, mechanical failure of implants and implant superstructures, as well as longer term complications such as peri-implantitis. Implant treatment also often involves multiple visits over several months. In young adults, the commitment to these appointments can prove challenging, especially if patients are away from home, at university for example. Patients must be fully informed of the need for long-term maintenance and the possible future financial implications of this.
Dental implants are not usually appropriate in adolescence and hence treatment is often postponed until at least the age of 18. Studies of craniofacial growth have shown that the facial skeleton continues to grow after puberty but that after the second decade of life this decreases and is clinically insignificant.9 Another study comparing ‘infraocclusion’ of dental implants in young adults (15.5–21 years old) and mature adults (40–55 years old) found no difference, suggesting that both groups had residual growth potential.10
An implant is effectively ankylosed, and will not travel with the surrounding alveolus during growth. The risk is that an implant placed before completion of alveolar/facial growth could end up relatively malpositioned in comparison to the adjacent teeth; a particular risk in the aesthetic zone.
One of the most challenging aspects of implant provision in these patients is the lack of alveolar bone in the edentulous site. Where primary teeth have been retained, the alveolus often ‘necks in’ apically to these teeth and again may complicate implant placement (Figure 10).
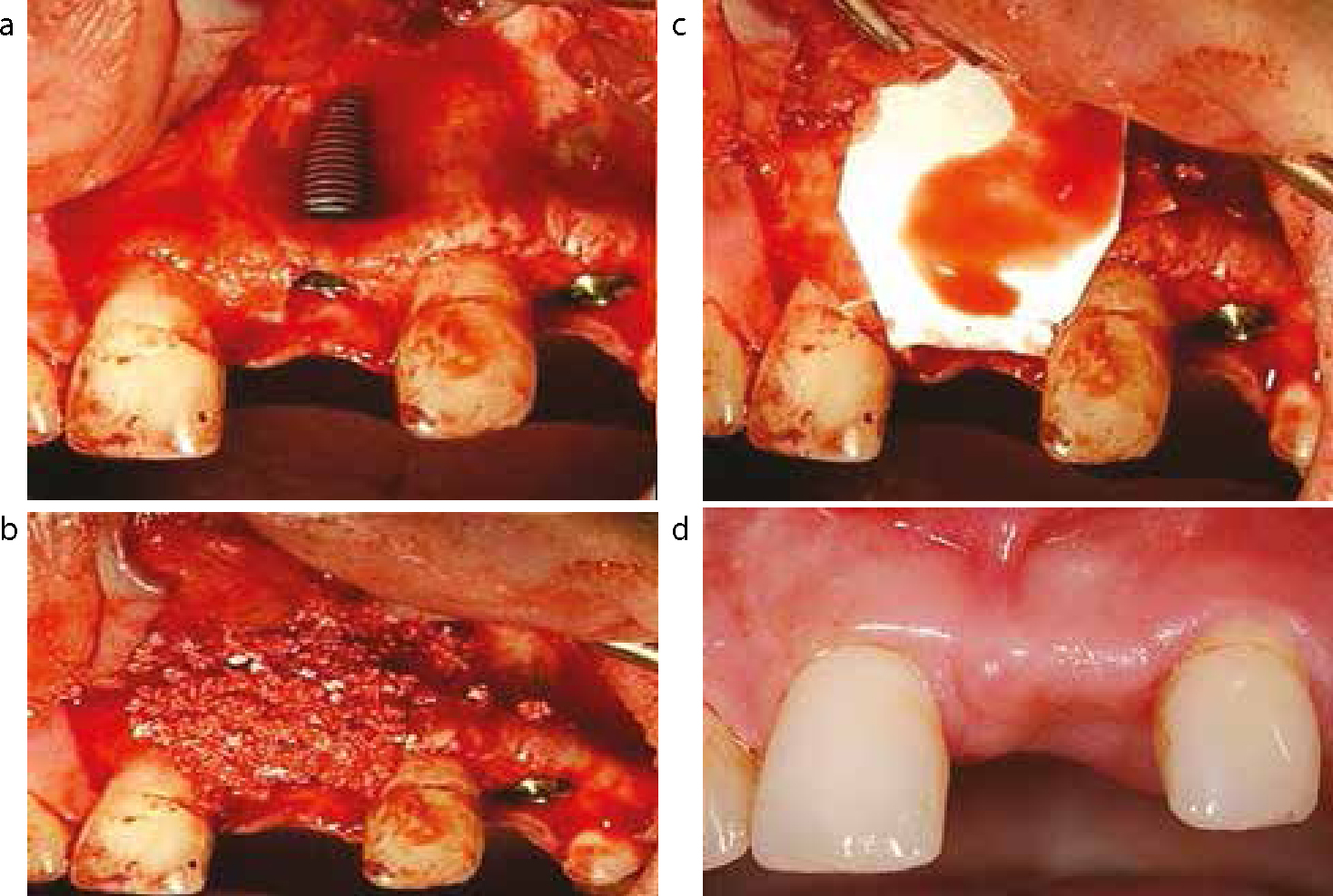
Figure 10.
(a–d) Demonstrates the problem with ‘necking’ of the alveolar ridge. In this case good primary stability was achieved as bone engaged apically and coronally. A standard guided bone regeneration procedure was performed using Bio-Oss and Bio-Gide (Geistlich, Wolhusen, Switzerland) using a double layer technique.
Figure 11 demonstrates a typical thin alveolar ridge seen in a hypodontia patient. Bone augmentation is often required to allow implants to be placed in the optimum prosthodontically driven positions. Ideally, implant diameter should be approximately the diameter of the tooth being replaced but narrow implants can be utilized where necessary.11 The position of adjacent structures such as the maxillary sinuses, nasal aperture and the inferior alveolar neurovascular bundle are further anatomical limiting factors for bone volume and implant placement.
Figure 11. Thin alveolus seen in edentulous regions of hypodontia patients.
With implants being placed in young individuals, the accumulative effects of minor complications should be considered. The predicted life expectancy of an individual born in 1990 in the United Kingdom is 76 years.12 If we place dental implants in patients in their early 20s we may expect them to last for over 50 years. With peri-implant crestal bone loss taking place in the range 0.02–0.1 mm per year,13 a rate of 0.1 mm per year could have significant effects in later life for these patients and long-term studies are required.
Achieving optimal aesthetics with implant restorations requires careful planning and there is often a challenge matching the optimal tooth position with where sufficient alveolar bone is present for the implant. Long clinical crowns can have an unpleasing appearance, but there is no evidence that the high crown-root ratio has a detrimental effect on the implant survival.14 Planning aids such as diagnostic wax-ups and cone beam CT scans with scan appliance in place allows appreciation of these challenges prior to embarking in complex surgery.
Severe hypodontia treatment options
Patients suffering from severe hypodontia have many clinical challenges, such as the lack of alveolar bone and occlusal disturbance. Treatment options include removable prosthesis which might have to be replaced regularly during growth periods. Implant-supported prosthesis may be the optimum definitive treatment option in the long term, but the extent of treatment required may make this goal unachievable or inappropriate.
Figures 12 and 13 show the pre- and post-treatment images of a hypodontia patient, respectively. This patient suffered from severe hypodontia with 22 missing permanent teeth (UR8, UR5, UR4, UR3, UR2, UL2, UL3, UL4, UL5, UL8, LL8, LL5, LL4, LL3, LL2, LL1, LR1, LR2, LR3, LR4, LR5, LR8.)
Figure 12.
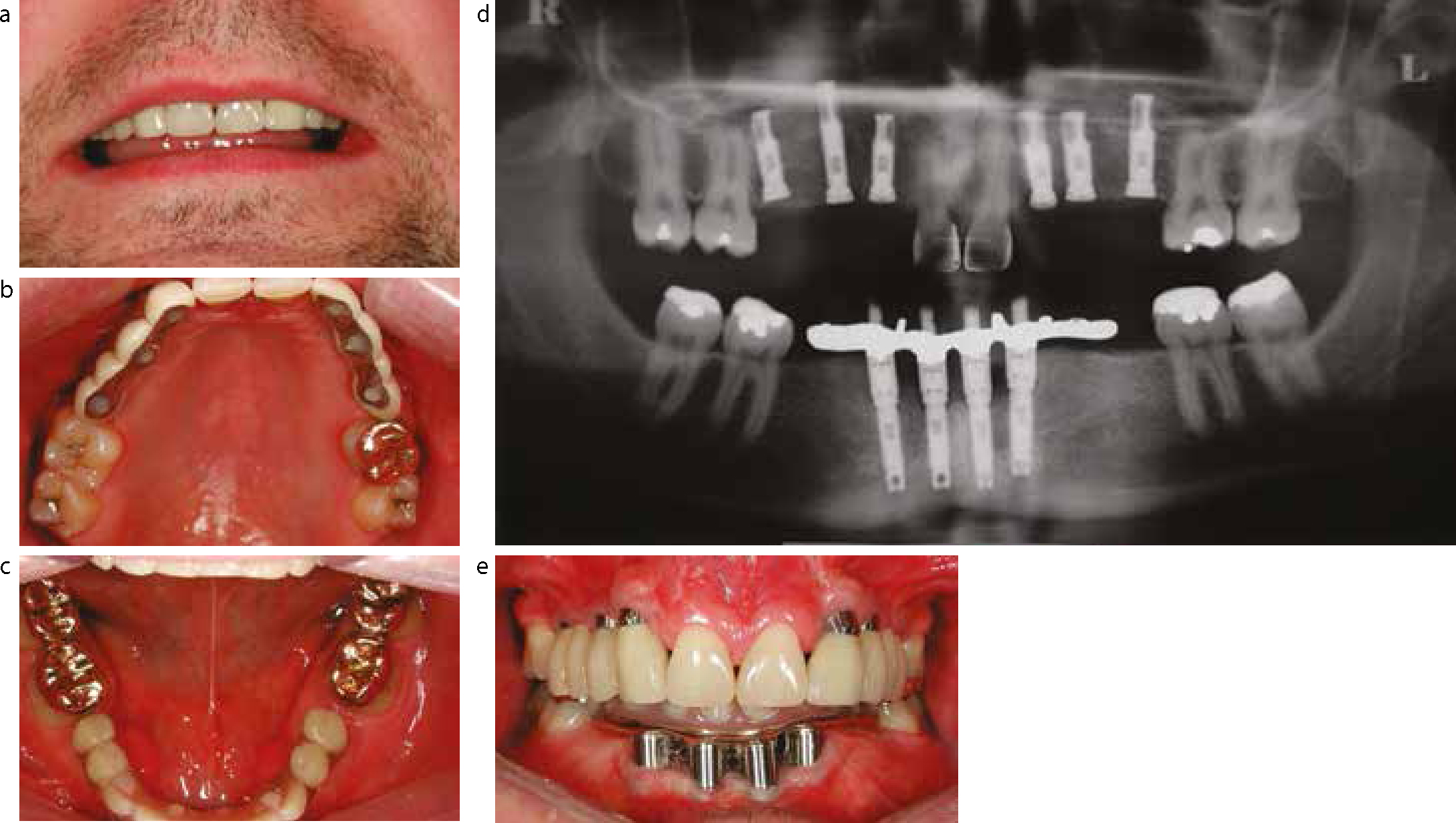
(a–c) Pre-treatment views of severe hypodontia case.Figure 13.
(a–e) Post-treatment views of severe hypodontia case.
Treatment included orthodontics to re-distribute the space, composite augmentations to UR1, UL1, dental implants and gold onlays on the mandibular molars. This case demonstrates the significant improvements that can be made to aesthetics and function for patients with severe hypodontia. However, it also demonstrates how a treatment plan can often be complex and requires multidisciplinary input. Figure 14 shows the acrylic mandibular fixed beam after 7 years. It shows considerable wear and required refurbishment of the acrylic portion, which is shown in Figure 15. This highlights the lifelong maintenance requirements that this complex restorative work necessitates.
Figure 14. Worn mandibular beam after 7 years of clinical wear.Figure 15. Refurbished mandibular beam.
Conclusion
These papers have highlighted the challenge faced by patients and clinicians in the management of hypodontia. Although we have focused on the interdisciplinary management of patients with hypodontia, it is important to highlight the role of the general dental practitioner in early diagnosis, prevention and long-term maintenance. Clinical management can often be complex and span many years. The final result can make a significant difference to a patient's quality of life with regard to function and aesthetics.