British Society of Periodontology and British Society of Paediatric Dentistry guidelines for periodontal screening and management of children and adolescents under 18 years of age. 2012. https://tinyurl.com/e55pyymhf (accessed May 2021)
Miller K, Treloar T, Guelmann M Clinical characteristics of localized aggressive periodontitis in primary dentition. J Clin Pediatr Dent. 2018; 42:95-102 https://doi.org/10.17796/1053-4628-42.2.3
Khandeparker RV, Khandeparker PV, Virginkar A, Savant K Bilateral Maxillary dentigerous cysts in a nonsyndromic child: a rare presentation and review of the literature. Case Rep Dent. 2018; 2018 https://doi.org/10.1155/2018/7583082
Freitas DQ, Tempest LM, Sicoli E, Lopes-Neto FC Bilateral dentigerous cysts: review of the literature and report of an unusual case. Dentomaxillofac Radiol. 2006; 35:464-468 https://doi.org/10.1259/dmfr/26194891
Tamgadge A, Tamgadge S, Bhatt D Bilateral dentigerous cyst in a non-syndromic patient: report of an unusual case with review of the literature. J Oral Maxillofac Pathol. 2011; 15:91-95 https://doi.org/10.4103/0973-029X.80017
Shear M, Speight P, 4th edn. Copenhagen: Blackwell Munksgaard; 2007
Dhupar A, Yadav S, Dhupar V Bi-maxillary dentigerous cyst in a non-syndromic child – review of literature with a case presentation. J Stomatol Oral Maxillofac Surg. 2017; 118:45-48 https://doi.org/10.1016/j.jormas.2016.12.001
Benn A, Altini M Dentigerous cysts of inflammatory origin. A clinicopathologic study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996; 81:203-209 https://doi.org/10.1016/s1079-2104(96)80416-1
Benn DK Spontaneous regression of bilateral dentigerous cysts. Br Dent J. 2002; 192
Neville BW, Damm DD, Allen CM, Bouquot JE Odontogenic cysts and tumors, 2nd edn. (ed.). Philadelphia, PA: WB Saunders; 2002
Morawala A, Shirol D, Chunawala Y Bismuth subnitrate iodoform parafin paste used in the management of inflammatory follicular cyst. Report of two cases. J Indian Soc Pedod Prev Dent. 2017; 35:269-274 https://doi.org/10.4103/JISPPD.JISPPD_328_16
Agrawal R, Sangle A, Vyawahare Bismuth iodoform and paraffin paste: a boon in treatment of keratocystic odontogenic tumour. A case report. Int J Dent Med Res. 2014; 1:32-35
The British Society of Periodontology, in collaboration with the British Society of Paediatric Dentistry, published guidelines in 2012 for the periodontal screening of children and adolescents. The guidelines recommended a simplified Basic Periodontal Examination (BPE) of six teeth for children aged 7–17 years. This is further modified for ages 7–11, using codes 0–2 from the 0–4 BPE adult chart. An unusual case of an 11-year-old boy who attended his general dental practitioner for a check-up is reported. Periodontal screening led to the detection of 13-mm pockets associated with the two mandibular first permanent molars that required surgical intervention and multidisciplinary care.
CPD/Clinical Relevance: This case report highlights the importance of paediatric periodontal screening in both primary and secondary care.
Article
Periodontal screening is recommended by the British Society of Periodontology for both children and adults, with screening to commence once a child has reached their 7th birthday. A simplified Basic Periodontal Examination (BPE), using six index teeth (UR1, UR3, UL6, LL1, LL6 and LR6) has been described for paediatric patients aged 7–17 years. The BPE is further modified for 7–11 year-olds, including codes 0–2 only, to avoid the recording of false pockets.1 The BPE is recorded in sextants, in the same manner that it is carried out for adults.
Alongside the detection of periodontal disease, periodontal probing can identify other abnormalities including: unexpected pus or cystic fluid secretion on probing; or isolated deep pockets that may be associated with cysts or bone pathology, as demonstrated in this clinical case.
This case highlights the detection of a rare incidence of non-syndromic large bilateral dentigerous cysts detected through routine periodontal screening within general dental practice. The differential diagnosis included false pocketing, or a periodontal anomaly. Following the radiographic examination, the differential diagnosis included keratocyst lesions or ameloblastomas.
Case report
A fit and well 11-year-old boy attended his general dental practitioner for his routine dental check-up. He complained of occasional bilateral pain in the lower molar region, of roughly 12-months duration, which had previously been diagnosed as growing pains. The pain was reported to be worse on eating, and he often experienced a strange taste in his mouth.
On examination, mild enamel hypomineralization of the permanent incisors and first permanent molars was noted, but overall, he had a healthy caries-free dentition. During a routine Modified Basic Periodontal Exam, pockets of 13 mm were detected at the mesio-buccal and disto-buccal aspect of LL6, and the disto-buccal surface of LR6. Pus was expressed from the pockets on probing. Both teeth gave positive responses to sensibility testing.
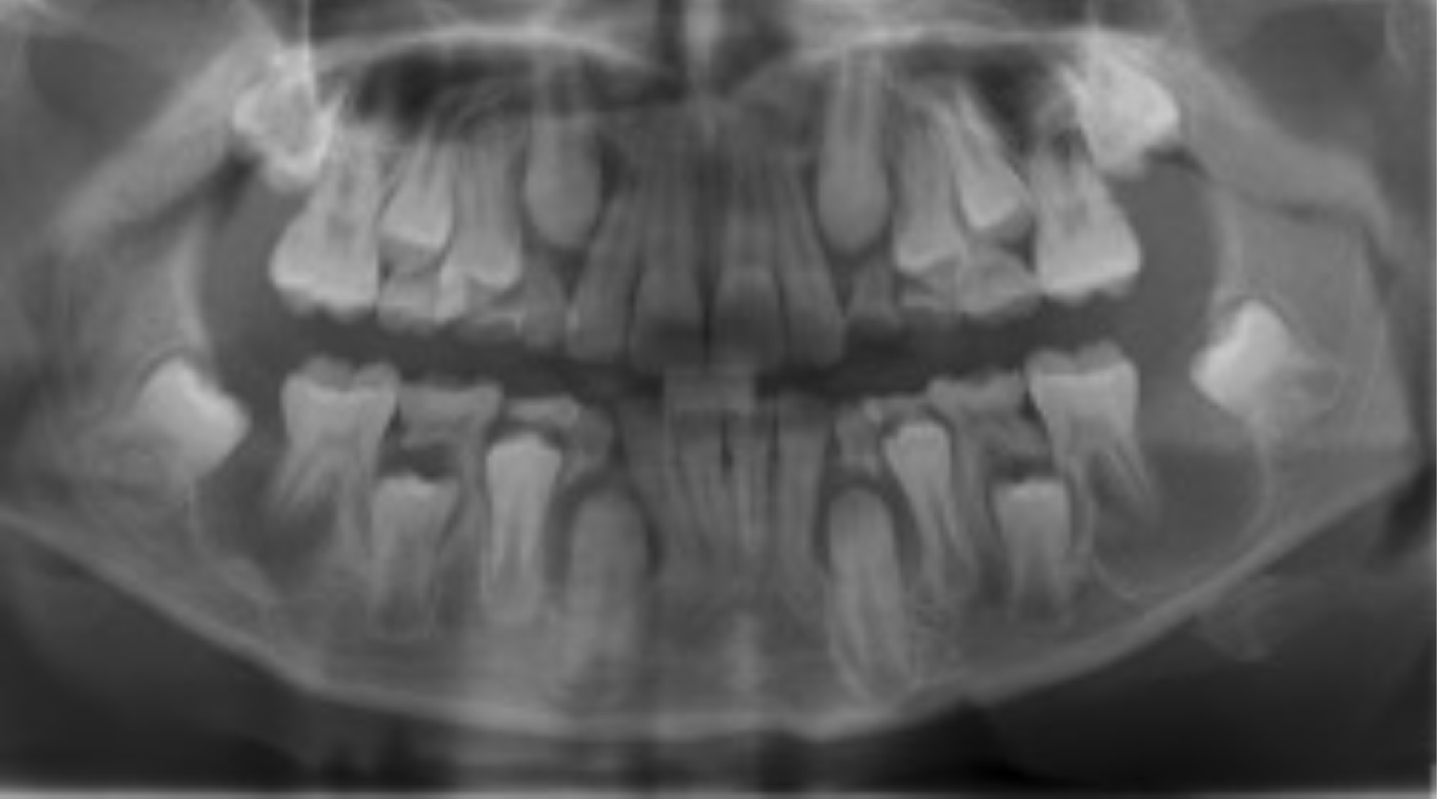
The pockets were deep and required further investigation. The patient was referred to the paediatric department at the local dental hospital where a dental panoramic radiograph was taken (Figure 1). This highlighted large radiolucencies distal to LL6 and LR6.
Figure 1. Initial dental panoramic radiograph.
Treatment
The lesions on the left and right mandible were marsupialized under general anaesthetic and the tissue was sent for histopathological examination. The presence of active infection resulted in the cavities being packed with bismuth subnitrate gauze swabs that were removed 1 week post-operatively.
Pathology, diagnosis and ongoing care
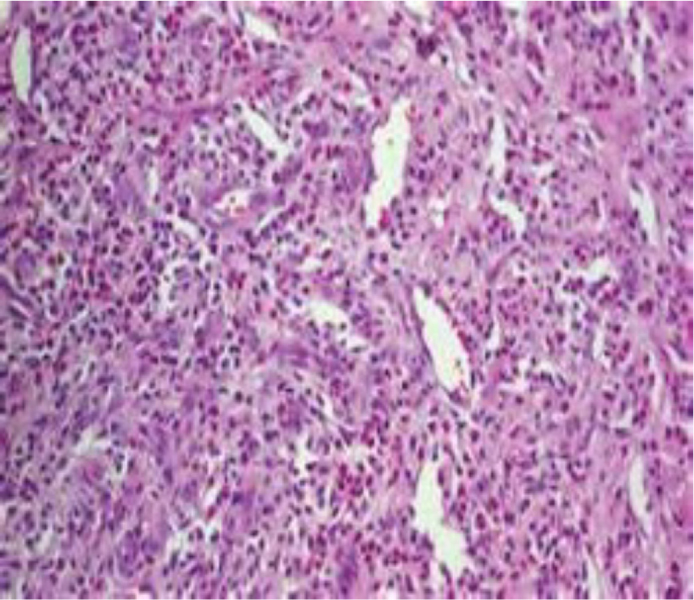
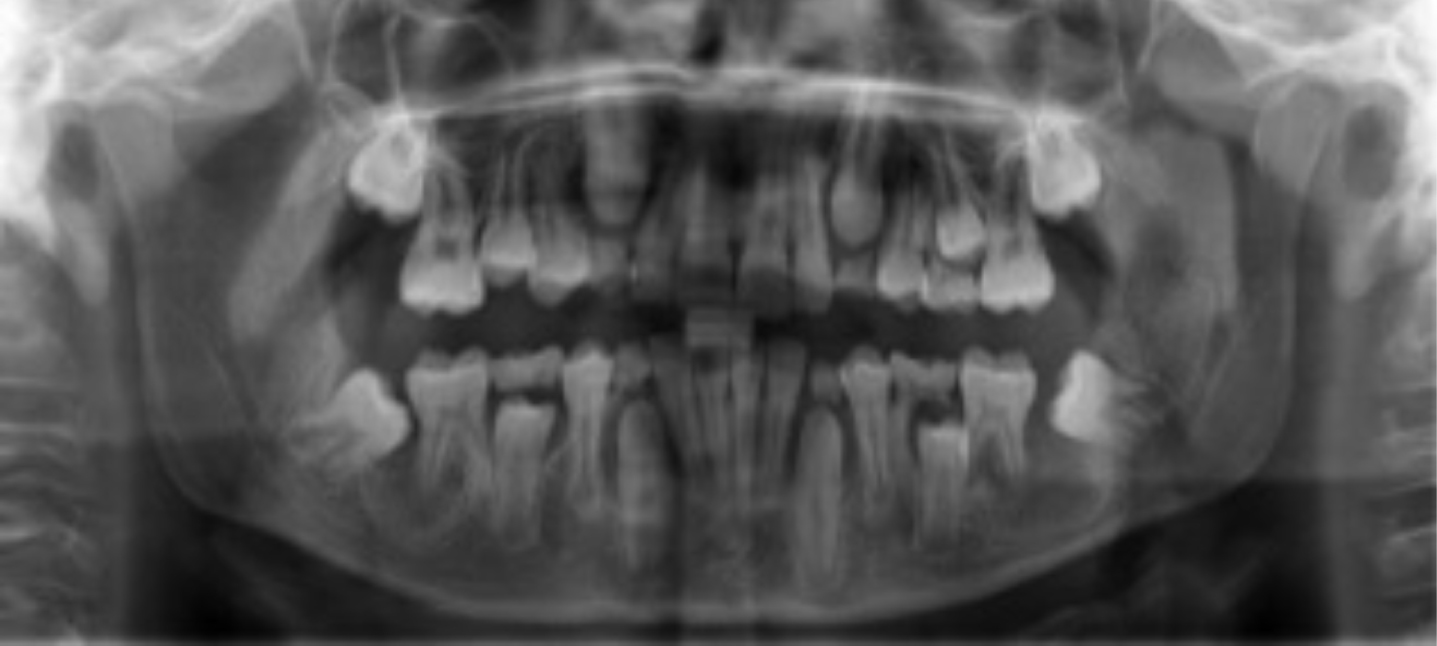
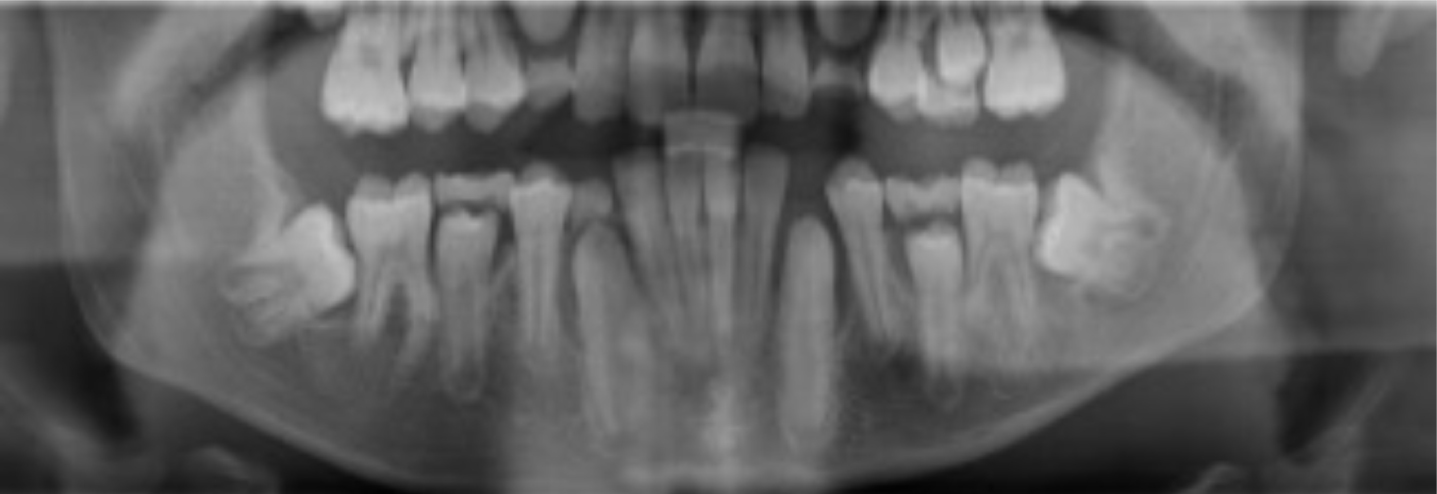
The two soft tissue specimens showed similar features, with significant active chronic inflammation and hyperplastic epithelial changes (Figure 2). Some dental follicle was found in one of the specimens. This favoured the diagnosis of bilateral inflamed dentigerous cysts. The dental panoramic radiographs were repeated at 1 year, then at 18 months following the surgery (Figures 3 and 4), demonstrating progressive bony infill. The lower first permanent molars have maintained positive sensibility test results at review appointments.
There is mesial impaction of LL7 and LR7. An orthodontic assessment was carried out and the patient had LL7 and LR7 exposed under sedation, to enable orthodontic realignment.
Discussion: how important is periodontal screening in children?
Although periodontal disease predominantly affects adults, children can also be affected. When children are affected, attachment loss can be rapid, and therefore, prompt referral to a specialist centre is necessary to facilitate early treatment and halt disease progression.2
Early onset of periodontitis can also be a manifestation of systemic diseases, for example Papillon-Lefèvre syndrome.3 This syndrome can lead to the early loss of primary or permanent teeth at a young age.
There is no evidence in the literature linking the diagnosis of cystic lesions or other bone pathology through periodontal screening; however, this case highlights how dental anomalies can be detected through this form of screening. In this case, the patient was diagnosed with, and surgically treated for, bilateral dentigerous cysts. This is a rare presentation in a patient without syndromic involvement.4,5,6,7,8
Accounting for 24% of cysts of the jaw, dentigerous cysts are the most common odontogenic developmental cyst associated with unerupted teeth. They are the second most common type of cyst, behind radicular cysts, when found alone. As they are usually painless, they are often found incidentally, unless they become infected. On a radiograph, they generally present around the crown of an unerupted tooth. The aetiology and pathogenesis of dentigerous cysts is controversial. The literature explores inflammatory and developmental origins.9 There is a proposed link between a non-vital predecessor, with a radicular cyst on this tooth, infecting the erupting permanent successor. This theory suggests that infection from the primary tooth spreads to the follicle of the erupting tooth, resulting in an infected dentigerous cyst. It is also suggested that the cyst formation is developmental in nature, with the cyst forming from the reduced enamel epithelium during the development cycle of the permanent tooth. In this clinical case, there was no caries or signs of vitality loss in the primary dentition.
Large dentigerous cysts often require surgical management, with a common treatment option being enucleation or marsupialization of the cysts, dependent on the size, age of the patient, proximity to important structures, for example the inferior dental canal, and the stage of root formation. There are a small number of reported cases that show dentigerous cyst regression without surgical intervention.10,11,12 However, this is a more common approach when the patient is asymptomatic, there is a clear diagnosis based on the radiological and clinical presentation, or there are medical contraindications to a surgical approach. The patient reported in this case report was fit for surgery, was symptomatic and a definitive diagnosis was required. This led to surgical intervention. The decision was made to marsupialize the cysts over the option to enucleate. This was due to the size of the cysts, the proximity to the inferior dental canal and the presence of active infection. The cysts on the left and right side of the mandible were marsupialized and packed with bismuth subnitrate iodoform paraffin paste (BIPP). The use of BIPP was introduced in 1916 by Rutherford Morrison.13 It has topical antiseptic properties, which are helpful in the management of active infection. Several cases have been reported in the literature, showing successful use of this technique, for managing infected cysts in paediatric patients.13,14
Although benign in nature, dentigerous cysts can cause destruction locally, resulting in bone loss, displacement of teeth and the requirement for extraction of affected teeth. Early detection and prompt treatment can help to reduce the detrimental consequences of the cyst formation.
Conclusion
This case highlights the importance of periodontal screening in all children from the age of 7 in both primary and secondary care. Although the primary role of the screening is aimed at early detection of periodontal disease, other abnormalities can be identified, as highlighted in this case.