Baniwal S, Paudel KR, Pyakurel U Prevalence of complications of simple tooth extractions and its comparison between a tertiary centre and peripheral centres: a study conducted over 8,455 tooth extractions. JNMA J Nepal Med Assoc. 2007; 46:20-24
Kandasamy S, Rinchuse DJ, Rinchuse DJ. The wisdom behind third molar extractions. Aust Dent J. 2009; 54:284-292
Goshtasby P, Miremadi R, Warwar R. Retrobulbar hematoma after third molar extraction: case report and review. J Oral Maxillofac Surg. 2010; 68:461-464
Bertram A, Rao A, Akbiyik K Maxillary tuberosity fracture: a life-threatening haemorrhage following simple exodontia. Aust Dent J. 2011; 56:212-215
Shah N, Bridgman JB. An extraction complicated by lateral and medial pterygoid tethering of a fractured maxillary tuberosity. Br Dent J. 2005; 198:543-544
Chrcanovic BR, Freire-Maia B. Considerations of maxillary tuberosity fractures during extraction of upper molars: a literature review. Dent Traumatol. 2011; 27:393-398
Saund D, Deitrich T. Minimally invasive tooth extraction: doorknobs and strings revisited!. Dent Update. 2013; 40:325-330
Awang M. Closure of oroantral fistula. Int J Oral Maxillofac Surg. 1988; 17:110-115
Javed F, Al-Askar M, Almas K Tissue reactions to various suture materials used in oral surgical interventions. ISRN Dent. 2012; 2012
Visscher S, van Minnen B, Bos R. Closure of oroantral communications: a review of the literature. J Oral Maxillofac Surg. 2010; 68:1384-1391
Assad M, Bitar W, Alhajj MN. Closure of oroantral communication using platelet-rich fibrin: a report of two cases. Ann Maxillofac Surg. 2017; 7:117-119
Bell G. Oro-antral fistulae and fractured tuberosities. Br Dent J. 2011; 211:119-123
Khandelwal P, Hajira N. Management of oro-antral communication and fistula: various surgical options. World J Plast Surg. 2017; 6:3-8
Fracture of the maxillary tuberosity: Troubleshooting in general dental practice and a proposed fracture classification Fiona Wright Colin Ritchie Nicholas J Malden Eleni Besi Dental Update 2024 48:2, 707-709.
Authors
FionaWright
BDS, MFDS (RCSEd), PGDip
DCT in Oral Surgery, Edinburgh Dental Institute, Lauriston Building, Lauriston Place, Edinburgh EH3 9HA, UK
A tuberosity fracture can prevent or delay the timely delivery of the most appropriate treatment option for a maxillary molar. This is a relatively common complication, but should not prevent treatment in general practice provided the clinician has adequately risk assessed, planned and obtained informed consent. Should a fracture occur, its initial management in general practice is encouraged. This article aims to improve patient outcomes by providing a troubleshooting guide. A fracture classification is suggested to aid assessment, recognition and management. Should referral to secondary care be required, a classification system will provide a basis for discussion and clarity on further management.
CPD/Clinical Relevance: This article provides a tuberosity fracture classification to guide clinicians in the management of patients who have sustained such a fracture.
Article
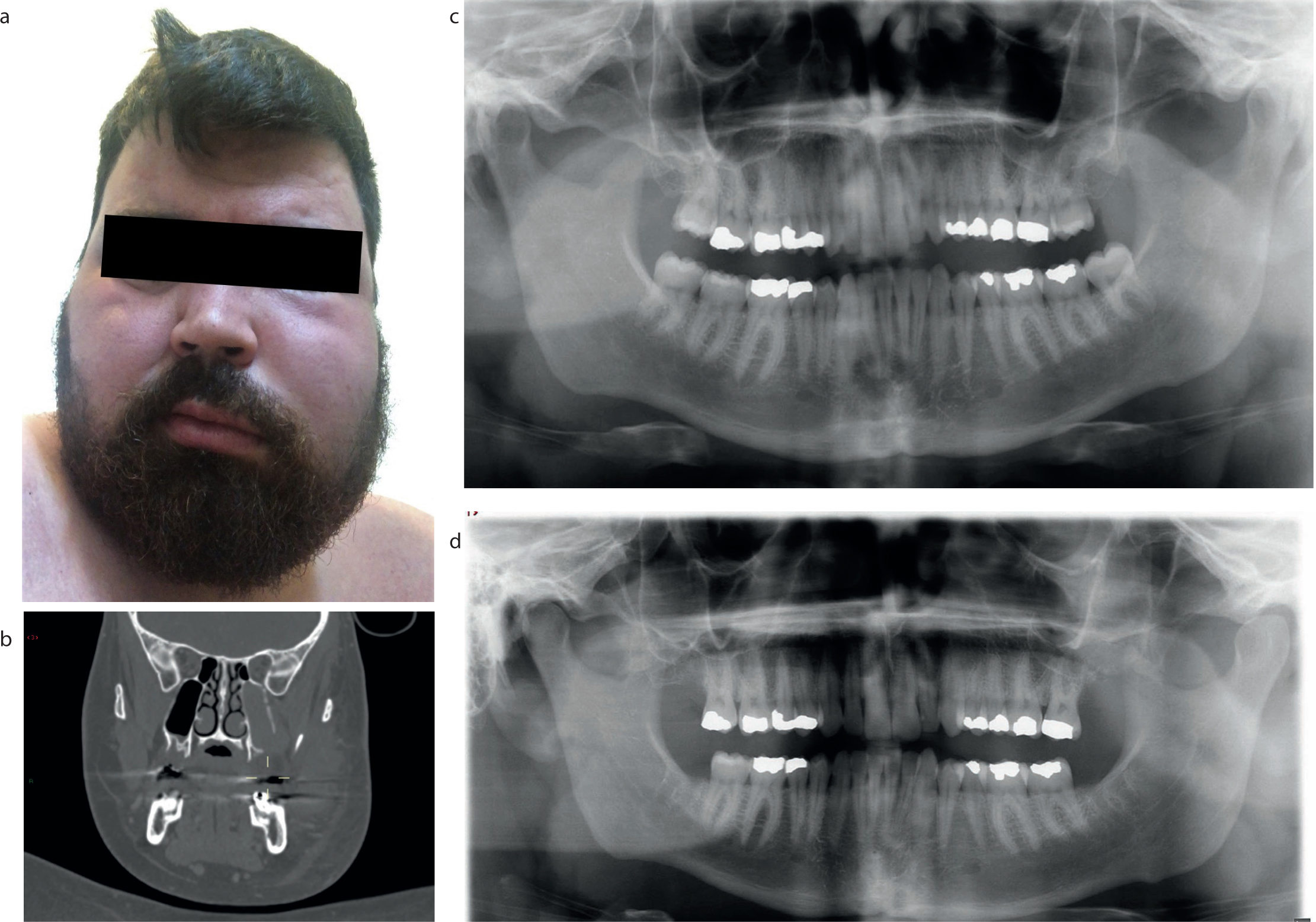
Tooth extraction can introduce a wide range of complications and risks. A complication of maxillary extractions is the fracture of the tuberosity with incidence documented at approximately 0.15–0.6%.1,2 Despite not being well documented in the literature, this type of complication can have a significant morbidity for patients3 and, in a few case reports, has been life threatening.4, 5Figure 1 shows a patient who experienced a tuberosity fracture during third molar removal and developed a lateral pharyngeal haematoma, presenting with severe facial swelling and dysphagia. The patient required urgent admission and emergency treatment to evacuate the haematoma and achieve haemostasis.
Figure 1. (a) Patient who had experienced a tuberosity fracture, resulting in facial swelling and dysphagia. He required urgent hospital treatment. (b) CT scan, coronal view, demonstrating OAC in area of previous UL8 and sinus opacified with haematoma. (c) Pre-operative OPT demonstrating large tuberosity with long narrow roots of UL8. (d) Post-operative OPT demonstrating loss of tuberosity and OAC in the UL8 area.
To assist with the diagnosis and management of a fracture, a classification system would be beneficial. To date such a system does not appear to be available. The aim of this article is to provide a troubleshooting guide for diagnosing and managing tuberosity fractures and propose a system of classification to facilitate discussion, consent process, management and referral of these fractures.
Consent for oral surgery procedures
In order to provide safe and effective treatment, meticulous planning and discussion is important for valid and informed consent. Previously considered uncommon events may need to be discussed with the patient if clinicians deem it of importance to gain valid consent. This is exemplified by the case of Montgomery v. Lanarkshire (SC 11 [2015] 1 AC 1430).
Clinicians should consider the following in their consent discussion regarding the risks associated with upper molar extraction, depending on their assessment of the tooth:
Tuberosity fracture;
Retained roots;
Oro-antral communication (OAC);
Roots into antrum;
Palatal soft tissue tear.
Patients should be made aware that if any of these situations were to occur, then further surgical treatment might be required, and in some cases, can pose a problem for future prosthetic replacement.
Risk factors for tuberosity fracture
Careful clinical and radiographic pre-operative assessment can highlight the associated risk factors6 and allow appropriate treatment planning.
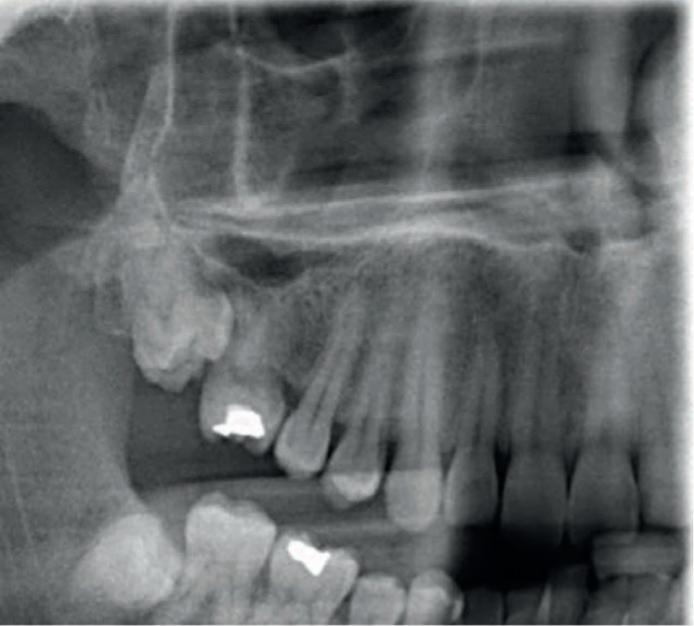
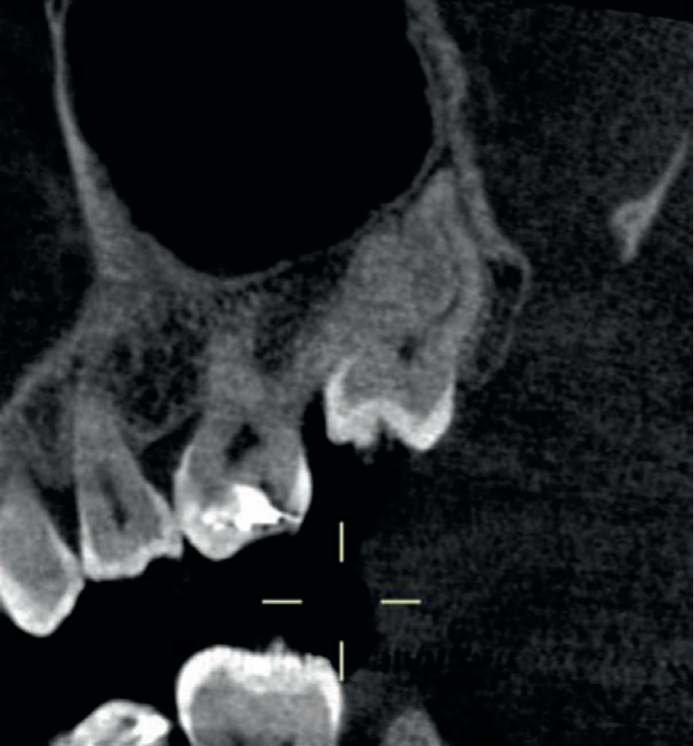
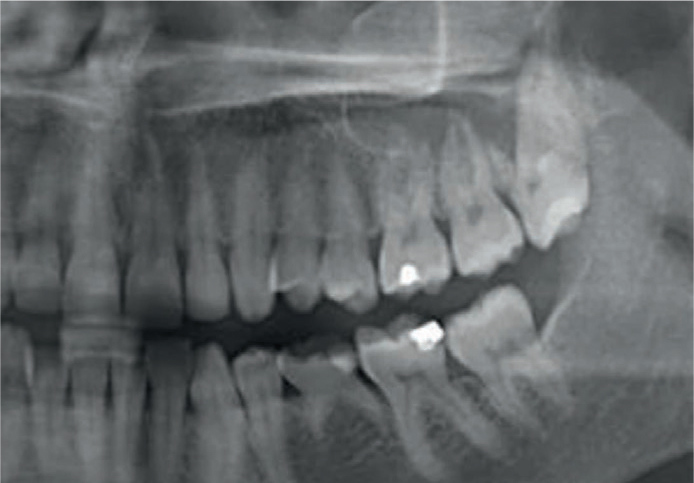
Figure 2. OPT demonstrating bulbous roots of UR8 and a submerged UR7.Figure 3. OPT demonstrates an impacted UR8, in close proximity to UR7.Figure 4. CBCT scan of Figure 3. Sagittal view demonstrates the UR8 fused to UR7. This required a surgical approach to remove the UR8, with root canal treatment and distal root amputation of the UR7 to maintain the tooth in function.Figure 5. CBCT scan in sagittal plane demonstrating multirooted UR8 seen in Figure 2.
Surrounding anatomy:
Large sinus
Expanding to extent of tuberosity Roots extending into sinus (Figure 6)
Resorbed maxilla (especially following premature loss of first molar)
Sclerotic tuberosity
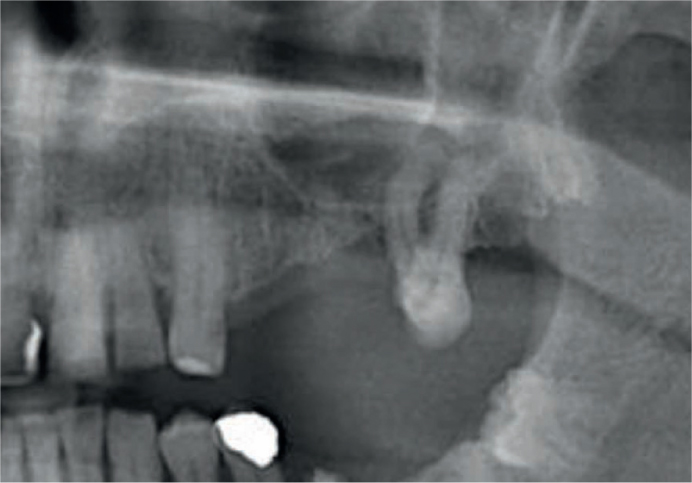
Figure 6. OPT demonstrating lone standing upper left second molar with low lying sinus floor and roots into sinus.
Figure 7. OPT demonstrating large cystic area affecting UL8, extending into the maxillary sinus.
Procedure related:
Unsupported extraction technique
Removal of multiple teeth in the maxilla, leaving distal tooth to last
Excessive force application
Despite the potential risks, the extraction of appropriate third molars can, and should be, performed in the general dental setting. Clinicians may want to consider the use of a luxator on all aspects of the tooth during these types extractions to reduce the risk of tuberosity fracture; however, should a fracture occur it is recommended the operator stop treatment, assess the severity of fracture and construct a management plan.
Classification
Table 1 details the proposed classification system for fractures.
Fracture type
Definition
Diagnosis
1
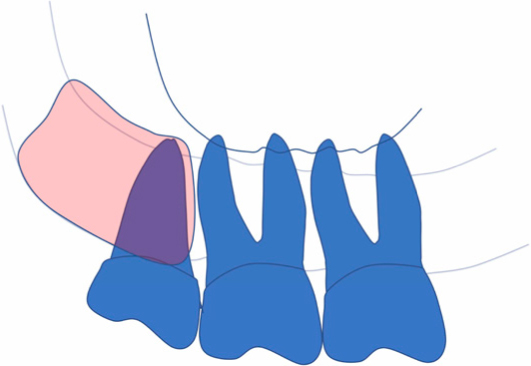
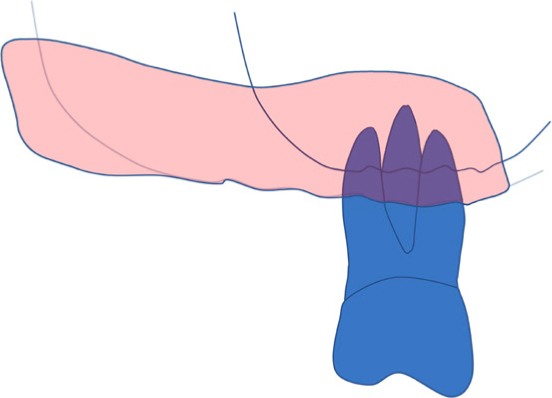
Small bony tuberosity, firmly attached to the last standing molar (usually the third molar) (Figure 8)
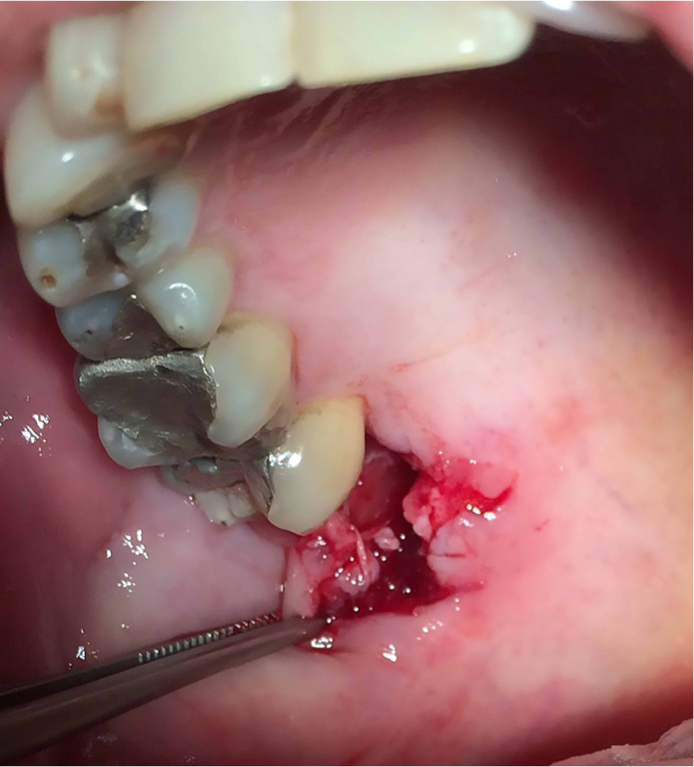
During the removal of an upper erupted third molar, the distal portion of bone remains firmly attached to the tooth root (Figure 9). This usually fractures on elevation and makes its presence known once the tooth has been delivered, or when the adherent soft tissue restricts delivery of the tooth. Sometimes a palatal tear may be noted (Figure 10)
2
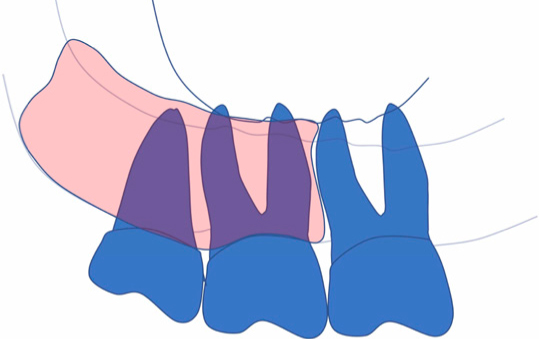
A fracture involving another tooth, which was not planned for removal, bearing a portion of bone (Figure 11)
During the extraction of an upper molar in a dentate arch, the adjacent tooth moves as one with the tooth planned for extraction during elevation and/or delivery. At this point, it is sensible to assume that a fracture has occurred or is imminent if you continue. As a consequence, the additional tooth could be lost inadvertently with the supporting bone
3
A fracture involving a significant portion of the edentulous bony floor of the antrum in the absence of adjacent teeth (Figure 12)
Removal of an upper permanent molar from an otherwise edentulous maxillary quadrant can result in this fracture, which includes all the bone distal to the tooth and including a variable amount of the antral floor. The clinician may notice movement of the full alveolar ridge with the tooth but failing this, a later sign of a palatal soft tissue tear may occur
Figure 8. Type 1 fracture. Small bony tuberosity, firmly attached to the last standing molar (usually the third molar).Figure 9. Tuberosity bone attached to extracted upper third molar as seen in Type 1 fracture.Figure 10. Palatal tear following upper third molar extracted as seen in Type 1 fracture.Figure 11. Type 2 fracture. A fracture involving another tooth, which was not planned for removal bearing a portion of bone.Figure 12. Type 3 fracture. A fracture involving a significant portion of the edentulous bony floor of the antrum in the absence of adjacent teeth.
Management
Type 1
The clinician should obtain a peri-osteal elevator or similar instrument to dissect the soft tissue from the tooth and connected bone to reduce the likelihood of the loss or tearing of soft tissue. Once the tooth and adherent tuberosity bone has been delivered, check for an OAC. This is not a usual complication for a Type 1 fracture. Simple suturing of the soft tissue should improve closure. A follow-up appointment should be arranged if there is any concern about post-operative complications.
Type 2
The clinician should abandon the extraction and prepare to splint the molar to the anterior adjacent tooth, ie the first molar or second premolar if it is present. The area should be allowed to heal for 6–8 weeks. Removal of the intended molar through elective surgical procedure should be planned. The clinician should consider extirpation of the tooth in the meantime, until there has been enough bony healing to allow extraction. As this is a dento-alveolar fracture, the operator may want to consider prescribing a suitable short antibiotic course.
Technical note: with the increasing availability of cone beam CT, obtaining three-dimensional imaging to assist in surgical planning is justified.
Type 2 tooth removal options
Closed removal approach: This technique is favoured by the authors and involves decoronation followed by surgical division of the individual roots using a surgical fissure burr or piezosurgical tip, followed by separation with a Coupland's chisel (or similar). Delivery of the roots can then be performed using fine-beaked forceps using a rotational movement to tease out the roots individually. The operator may also wish to use a narrow luxator to aid mobilization of the roots in an atraumatic fashion. Bone removal may be required in some cases, but can usually be performed without the need to raise a mucoperiosteal flap. In addition to this method, there are systems available which deliver ‘flapless extractions’ such as the Benex system,7 which uses a pulley system that severs the periodontal ligament in a controlled fashion and aims to promote bone preservation during extraction.
Conventional surgical approach: A buccal mucoperiosteal flap should be designed to allow closure if an OAC should form because of the surgical removal. Initially using a mesial relieving incision will allow exposure of the buccal plate pending progress of the surgery. Following removal of buccal bone, forceps should be used with light forces. If the fracture recurs, then surgical removal of the second involved tooth may also need to be considered with modification of the flap distally to include the buccal bone adjacent to this tooth. A closed tooth removal technique should again be considered. It is strongly recommended that the patient be followed up to ensure any complications be managed in a timely manner and to provide assurance for the patient.
Type 3
If this fracture presents, hopefully at an early stage, the clinician needs to decide whether to raise a flap as in the Type 2 fracture and proceed to remove the tooth surgically, or to leave the tooth in situ until bony healing has occurred. The clinician should be aware that elevating the periosteum off the fracture fragment may further compromise the circulation leading to devitalization and subsequent complications including infection and sequestration.
The idea of immediate removal of a large bony segment with the tooth and effecting soft tissue closure can seem drastic due to the volume of bone that would be lost; however, it is an option to consider, especially if the tooth is affected by peri-apical pathology.
Another option would be to decoronate the tooth leaving the roots in situ. This can achieve a double purpose.
It reduces occlusal trauma (therefore reducing pain) and reduces the disturbance of the maxillary floor fracture during the healing process.
It prevents anyone else putting forceps on the tooth, therefore indicating a surgical approach (closed or conventional surgical removal) is the only option remaining.
The tooth may need to be extirpated and pulp canals sealed in this event to reduce post-operative pain. As with any maxillofacial fracture, if a tooth is left in an open fracture site then a suitable antibiotic regimen may be justified. Once bony healing has occurred, surgical removal of the tooth should be performed as previously described. Again, adequate follow-up review for these cases is pertinent for optimal patient care and will allow the operator to refer onto secondary care if suitable progress is not being made.
Clinicians should bear in mind that decoronation of the tooth reduces the ability to splint the tooth, if this is necessary, and can increase the risk of infection due to the roots remaining in situ.
More serious complications
In terms of haemorrhage following tuberosity fracture (most likely to be from a palatal soft tissue tear), the clinician should remain calm and achieve haemostasis. The administration of further local anaesthetic containing a vasoconstrictor if permitted, with packing of the socket with a haemostatic agent. Soft tissue tears should be sutured and pressure applied. A telephone conversation with the local Oral Surgery or Oral and Maxillofacial Unit to gain advice on further action if there are any persisting concerns, and the decision on whether to refer, can be made at this point.
Antral floor involvement
If the bony antral floor has been lost, the sinus is deemed to be breached. Any OAC should be closed at the earliest opportunity, usually with a buccal advancement flap +/- buccal fat pad.8 If the clinician is unable to provide this treatment or a colleague/surgical unit is not available on the ‘same day’, then packing the socket gently with a haemostatic agent with suturing would suffice. For closure, the preferred suture material would be a monofilament, non-absorbable type such as nylon-based sutures because they provide a longer duration of tissue approximation and reduce inflammation and infection.9 The alternative would be absorbable agents, such as Vicryl. Non-absorbable sutures should be removed 14 days after the procedure. When placing sutures, the horizontal mattress suture is ideal as it spreads the tension of the closure over a wider area, reducing risk of wound breakdown and improving tissue support. This should be used along with simple interrupted suture where necessary.
Further referral into secondary care for re-evaluation and definitive closure would be advised. More advanced options for repair include palatal rotational flaps, use of acrylic cover plates, guided bone/tissue regeneration,10 and leukocyte- and plasma-rich fibrin (L-PRF).11
Post-operative instruction
For a tuberosity fracture that has been managed in practice, advise the patient to maintain good oral hygiene with regular tooth-brushing to reduce bacterial load and gentle mouth-washing either with warm salted water or chlorhexidine digluconate 0.2%. The patient should be reviewed again in 7–14 days and any non-resorbable sutures placed should be removed. If the tooth is still to be extracted, then review again in a further 6 weeks to remove any splints, assess whether bony healing has occurred and plan for its removal.
What about decongestants?
In the presence of an OAC, appropriate post-operative management is advised.12, 13
For 2 weeks:
No nose blowing
Sneeze with mouth open
Avoid non-essential air travel
Use a straw for drinking
Consider:
Broad spectrum antibiotic, eg amoxicillin 500 mg, three times daily for 5–7 days. If contraindicated due to allergy, doxycycline 200 mg for the first day and 100 mg daily for the following 6 days)
Ephedrine nasal drops 0.5%, one drop into each nostril, three times daily for a maximum of 7 days.14
Conclusion
By understanding the risk factors, signs and management of tuberosity fractures, clinicians can more ably manage these complications of upper molar extraction within the environment of primary care. Perhaps the Type 3 fracture, more so than any other described, produces a sense of immediate regret in the unsuspecting clinician. Especially when the patient was elderly, had a complicated medical history and was slotted in as an emergency toothache in the late afternoon.
As with all these cases, in hindsight the clinical and radiological evidence may well have alluded to the existence of potential problems. A phone call to your local Oral Surgery or Oral and Maxillofacial Surgical colleagues after such a procedure has been attempted might well provide some helpful advice.
Perhaps the most important point to take away is that recognition of this complication in the early stages allows for a change of tack and putting a ‘plan B’ into action.