Tracey C, Lee R T. Root resorption: the aggressive unerupted second premolar. Br Orthodontic J. 1985:97-101
Sian J S. Root Resorption of First Permanent Molar by a Supernumerary Premolar. Dent Update. 1999; 26:210-211
Tabiat-Pour S, Newlyn A. Root resorption of a maxillary permanent first molar by an impacted second premolar. Br Dent J. 2007; 202:261-262
Ericson S, Kurol J. Incisor root resorptions due to ectopic maxillary canines imaged by computerized tomography: a comparative study in extracted teeth. Angle Orthod. 2000; 70:276-283
Wang H Y. Root resorption associated with impacted maxillary third molar. Oral Surg Oral Med Oral Pathol. 1992; 73:765-766
Haapasalo M, Endal U. Internal inflammatory resorption: the unknown resorption of the tooth. Endodontic Topics. 2006; 14:60-79
Patel S, Dawood A, Whaites E, Pitt Ford T. The potential applications of cone beam computed tomography in the management of endodontic problems. International Endodontic Journal. 2007; 40:818-30
Kim E, Kim KD, Roh BD, Cho YS, Lee SJ. Computed tomography as a diagnostic aid for extracanal invasive resorption. Journal of Endodontics. 2003; 29:463-5
Patel S, Dawood A, Wilson R, Horner K, Mannocci F. The detection and management of root resorption lesions using intraoral radiography and cone beam computed tomography – an in vivo investigation. International Endodontic Journal. 2009b; 42:831-8
Waterhouse P J, Nunn J H. Crown and root resorption of a maxillary permanent first molar by an impacted second premolar: a case report. Int J Paediatr Dent. 1995; 5:259-262
Hall F M, Cook P A. Resorption of first mandibular molar. Br Dent J. 1989; 166:19-20
Resorption of maxillary first permanent molars by impacted maxillary second premolars: A case series Isabelle Heliotis Manpreet Gakhal Rosemary Whatling Dental Update 2024 47:11, 707-709.
Authors
IsabelleHeliotis
Specialty Trainee in Paediatric Dentistry, Royal London Dental Hospital, Turner Street, Whitechapel, London E1 1DE
Although rare, resorption of the first permanent molar caused by impaction of the second premolar does occur. Three paediatric patients with impacted upper second premolars, distinct symptoms and signs of resorption are described. One case with clear resorption of the upper molar on initial presentation was managed immediately with extraction of the first permanent molar. Eruption of the impacted premolars was monitored in the other two cases, but symptom changes and sectional cone beam computed tomography (CBCT) highlighted resorption of the first permanent molars. In both cases the resorbed first permanent molars required extraction. Frequent clinical and radiographic assessment is imperative in such cases, along with consideration for the use of CBCT.
CPD/Clinical Relevance: Many dental health professionals are unaware that resorption of maxillary molars induced by impacted premolars is possible, thus, this phenomenon is not monitored, resulting in misdiagnosis and avoidable patient morbidity.
Article
Introduction
It is generally considered that impacted second premolars in both the mandible and maxilla will eventually erupt with or without displacement. Surgical removal of the impacted premolar is often avoided owing to the potential risk of damage to adjacent teeth and surrounding anatomical structures such as the mental nerve.1 Root resorption of first permanent molars by impacted premolars has been previously reported but remains a rare, clinical phenomenon.1,2,3 Resorption is most commonly documented relating to upper incisors associated with ectopic canines and supernumeraries or in the second molar region with impacted third molars.4,5
This case series describes the presentation of three female patients to the Royal London Paediatric Dental Department over a 5-year period. The patients had impacted maxillary second premolars that resulted in the resorption of the first permanent molar. The level of dental crowding in each patient ranged from mild to severe, and all three individuals experienced pain in clinically different manners.
Case 1
This 13-year-old girl was referred from her general dental practitioner (GDP) for ‘multiple hypoplastic teeth causing pain’. She presented with a class 1 incisor relationship on a skeletal I base, with class 2 molars on the right and class 2 ½ unit molars on the left. She presented with moderate crowding in her upper anterior segment and severe crowding in the posterior upper arch.
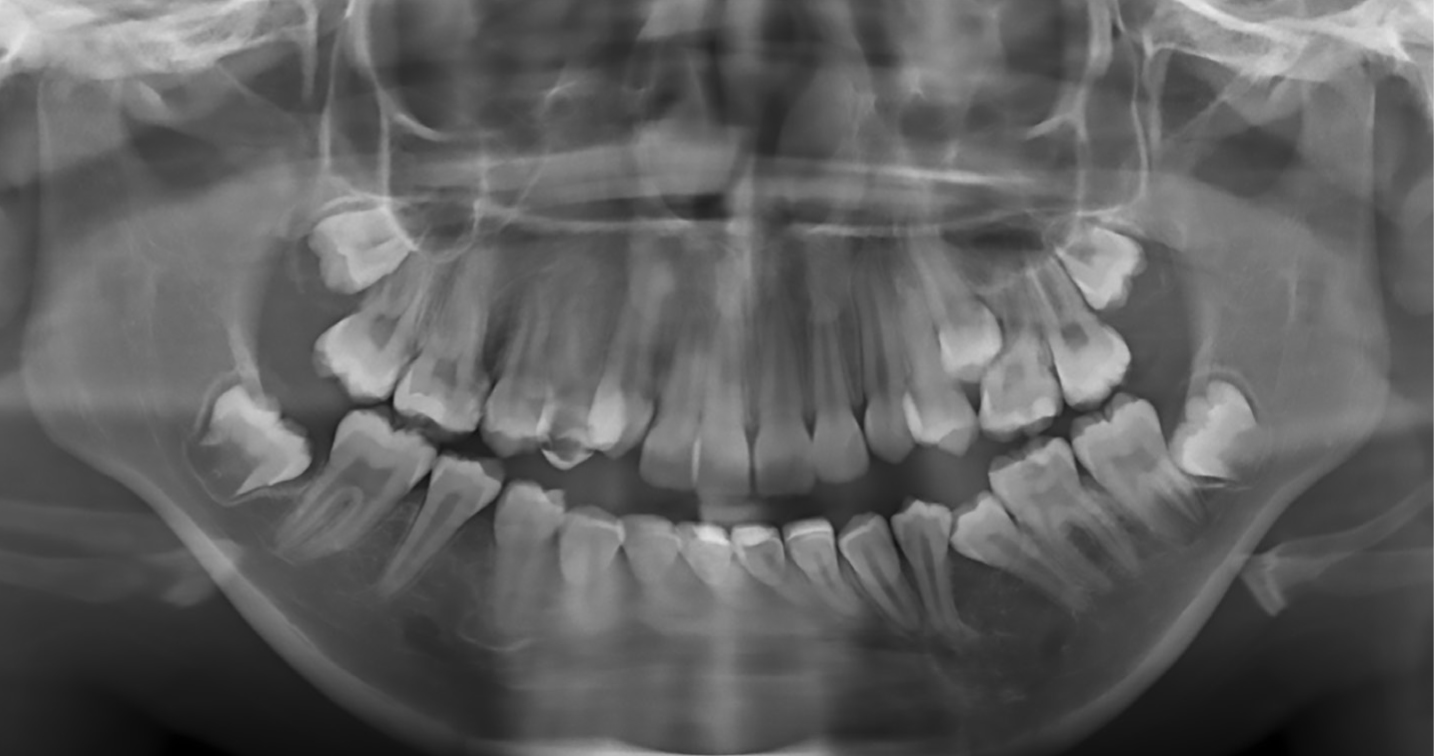
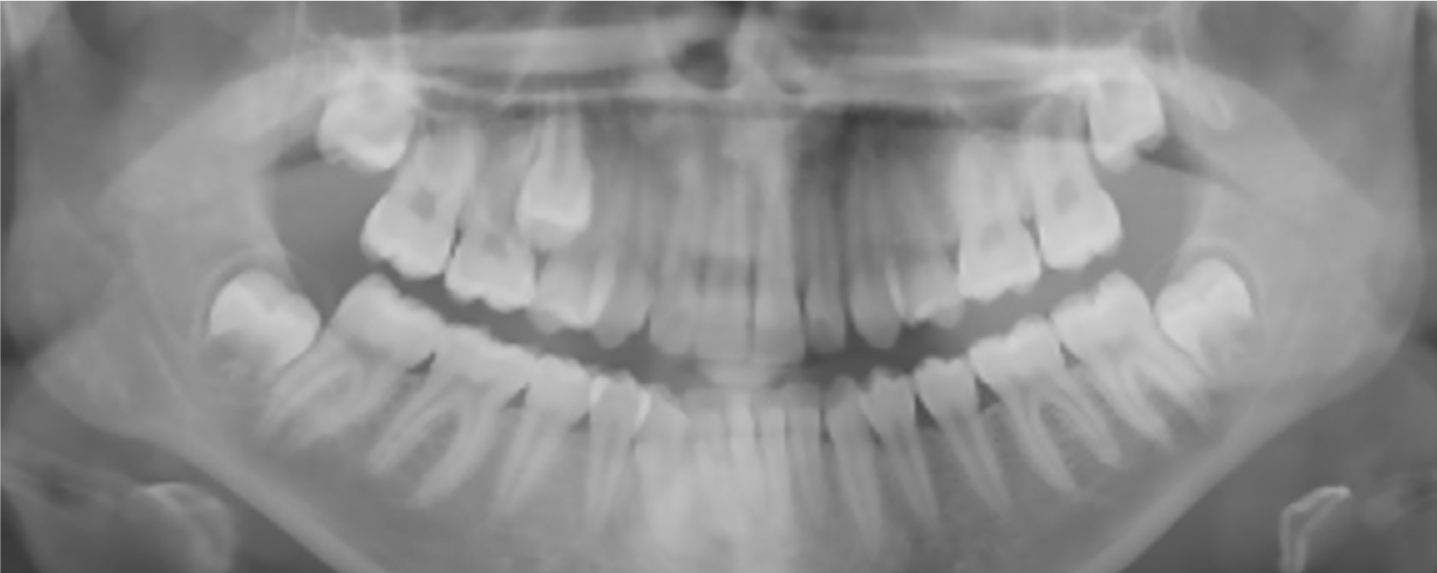
The patient reported only sensitivity from the upper left (UL) 7 with chronological hypoplasia when eating cold foods, but had no symptoms from the UL6. She was medically fit and healthy. Clinical examination revealed that her upper left second premolar was clinically unerupted with the UL46 in contact. There was a palpable palatal swelling. An orthopantomogram (OPG) radiograph identified impaction of both the UL5 and lower left (LL) 5 with possible resorption of the mesiobuccal and palatal roots of UL6 (Figure 1).
Figure 1. OPG taken in January 2015 showing impaction of UL5 and LL5, with possible root resorption of the UL6. No dentine caries was evident in the upper left quadrant.
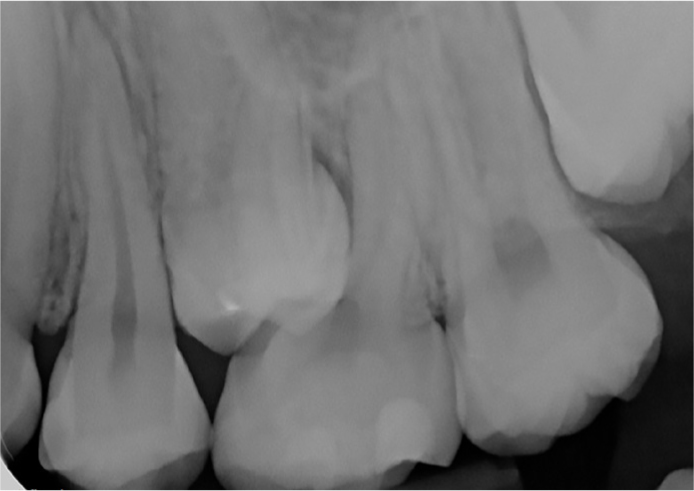
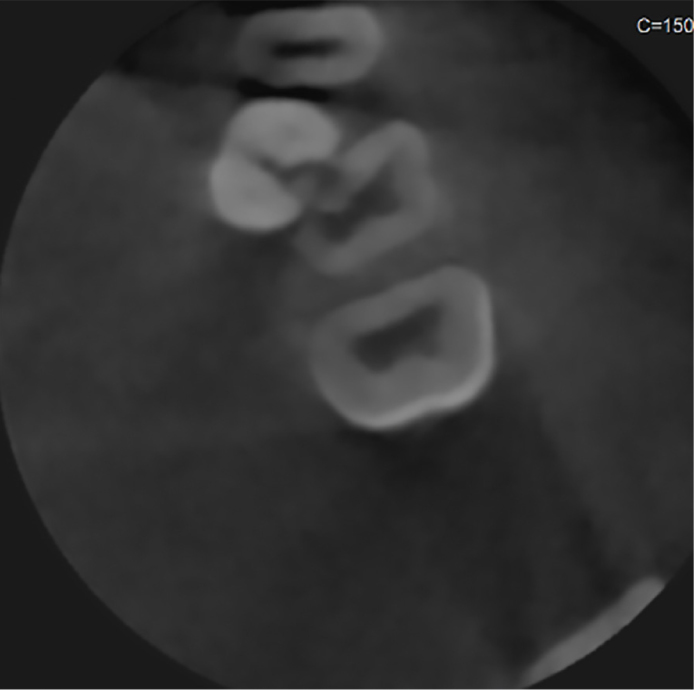
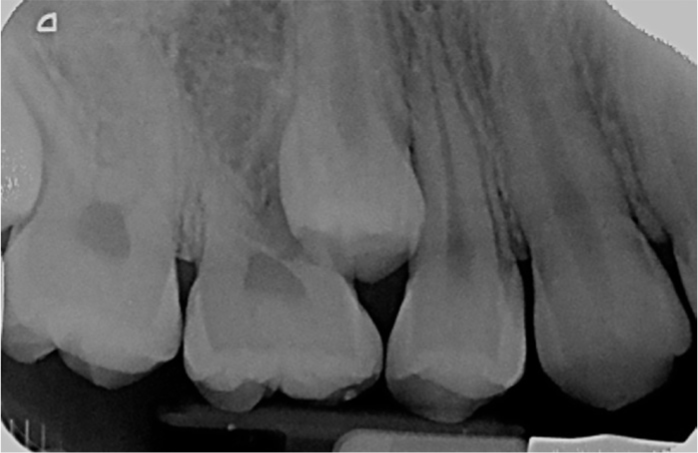
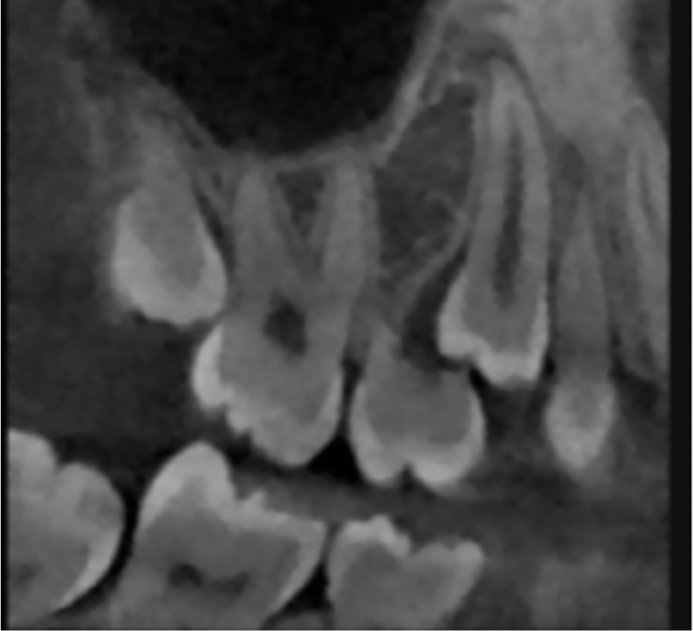
The patient was immediately referred to the joint orthodontic–paediatric clinic in 2015 where a periapical radiograph was taken of the UL56 (Figure 2). Owing to the asymptomatic nature of the UL6, and positive results to sensibility testing, it was not clear whether the radiograph presented superimposition of the two teeth or resorption. The patient was reviewed 12 months later at which stage she reported ‘a shooting pain when biting’ from the UL6 and ‘aching’ from the UL6 region causing her to ‘wake up at night’. A sectional cone beam computed tomography (CBCT) (Figure 3) was taken at this point, confirming resorption of UL6. The report highlighted that there was significant resorption of the palatal and mesiobuccal roots of the UL6. There was no resorption associated with the UL4. It was therefore decided to surgically extract UL6 under local anaesthesia. Owing to the severe resorption of the UL6, the palatal root fractured and required surgical removal.
Figure 2. Periapical radiograph taken November 2015 showing superimposition and possible resorption of the mesiobuccal root of the UL6 from UL5. Sound restorations are present in the UL6. No caries is evident.Figure 3. Sectional CBCT taken in November 2016 showing impaction of UL5. The crown lies between the roots of the UL4 and UL6. There is significant resorption of the palatal and mesial aspect of the UL6. There is no resorption associated with the UL4.
Review appointments were made following the UL6 extraction to assess eruption of the UL5 and space closure at the joint orthodontic–paediatric clinic; however, unfortunately the patient was not brought.
Case 2
This 12-year-old girl was referred in 2017 by her GDP for ‘impacted teeth and supernumeraries’. She presented with a class 2 division 1 incisal relationship on a skeletal III base with bilateral class 1 molars and severe crowding of the upper left arch. The patient had reported only one episode of ‘short lasting pain’ in the upper left region. Medically, she was diagnosed with autism and systemic lupus erythematosus.
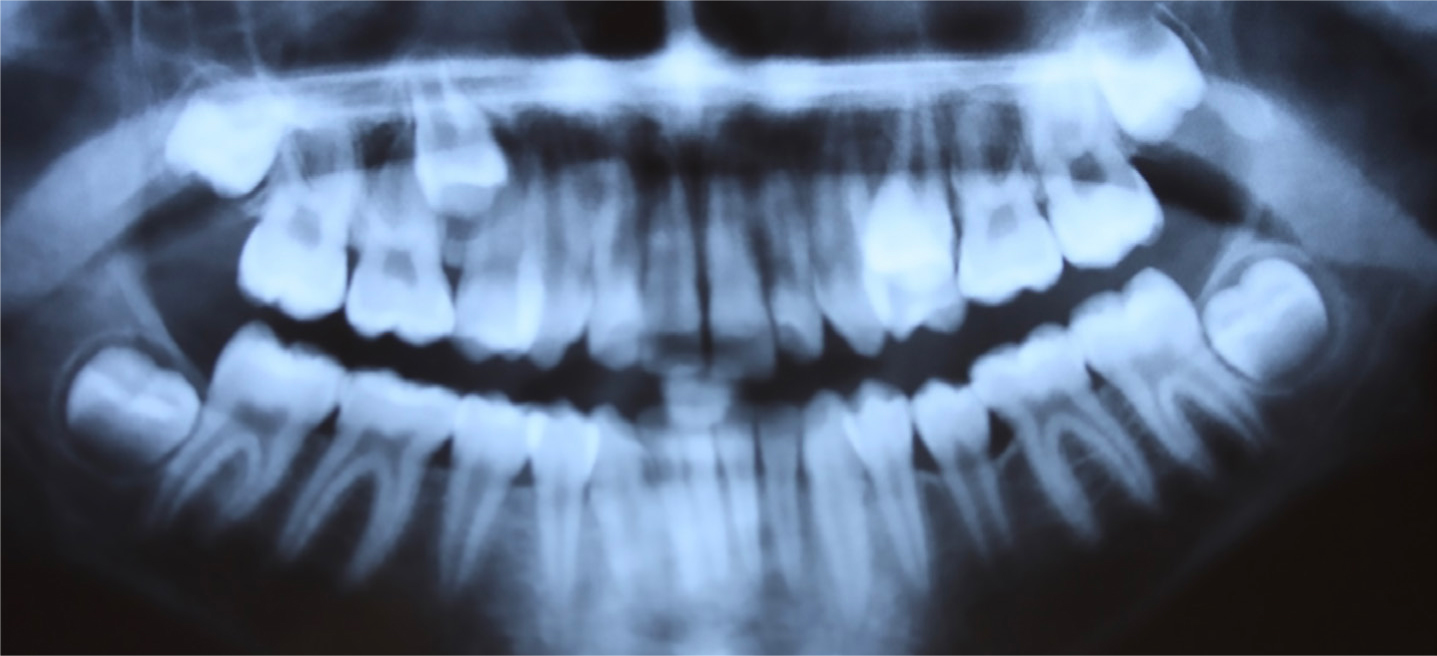
Clinical examination identified the presence of a supplemental supernumerary in the UL quadrant followed by UL4, UL5 with impaction against the UL6 and a grossly carious mesio-occlusal cavity of the UL6. An OPG confirmed clinical findings and also highlighted the resorption of the UL6 by the impacted UL5 along with the presence of further unerupted supplemental teeth in the LL45 lower right (LR) 45 regions (Figure 4).
Figure 4. OPG showing resorption of UL6 by UL5, and the presence of supplemental teeth in the upper left quadrant and LL45, LR45 regions.
It was arranged for the UL6 to be surgically extracted under general anaesthetic due to limited cooperation. The palatal and distobuccal roots were extracted uneventfully but a buccal flap with bone removal was required to remove the remaining mesiobuccal root.
The supplemental tooth in the upper left quadrant was left in situ, with the space left to close following removal of the UL6 and complete eruption of the UL5. The unerupted supplemental teeth in the lower arch were also left to be monitored with yearly radiographic review, owing to the risk of damage to the mental nerve associated with surgical removal and the wishes of the child's mother to avoid further surgical procedures.
Case 3
This 11-year-old girl was referred by her GDP in 2012 regarding ‘unerupted upper second premolars’. She presented with a class 1 incisor relationship on a skeletal I base with class 2 ½ unit left molar relationship and class 2 right molar relationship, and well aligned upper and lower arches.
On initial examination, the patient reported symptoms. She was medically fit and healthy.
Clinically, the UL5 was erupted and palatally positioned and the upper right (UR) 5 was unerupted but palpable palatally. Figure 5 confirms the presence and position of the impacted teeth with an inability to determine the presence of any resorption of the UR6.
Figure 5. OPG taken by GDP in April 2012 identifying the impaction of the UL5 and unerupted UR5. Any resorption of the UR6 is difficult to diagnose from the radiograph.
It was planned for the UL5 to be extracted under local anaesthetic and the eruption of the UR5 to be reviewed after 1 year. At the review appointment on a joint paediatric–orthodontic clinic, the patient reported a ‘slight aching pain’ from the UR6, but with no disturbance to sleep. Sensibility testing of the UR6 was positive and a repeat OPG radiograph was taken (Figure 6). A joint decision was made to allow the premolar to erupt further and then to extract, this was reviewed after 1 year.
Figure 6. OPG taken in April 2014 showing possible resorption of UR6 mesiobuccal +- palatal roots induced by the UR5.
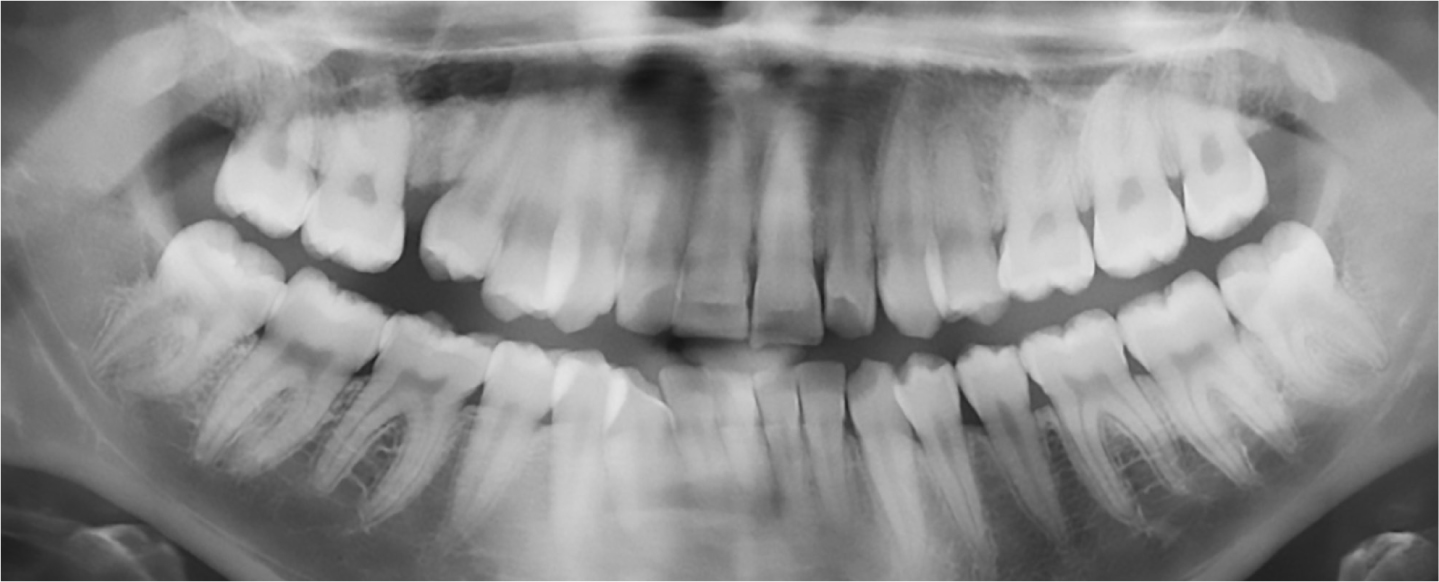
At the 2-year review, an intra-oral periapical radiograph (Figure 7) showed clear resorption of the mesial root of the UR6. A sectional CBCT scan (Figure 8) identified extensive resorption of the mesiobuccal and palatal roots of the UR6. It was arranged for the UR6 to be extracted surgically under inhalation sedation with a buccal flap and bone removal to extract the grossly resorbed mesiobuccal and palatal roots. This, in turn, allowed the UR5 to erupt successfully, which was followed by an upper fixed appliance to aid space closure. Figure 9 highlights the remaining space in the upper right quadrant following extraction of the UR6 requiring orthodontic closure.
Figure 7. Periapical radiograph taken in August 2015 showing resorption of mesiobuccal +- palatal root of UR6 from the impacted UR5.Figure 8. Sectional CBCT taken in October 2015 showing extensive resorption of the mesiobuccal and palatal roots of the UR6 induced by the impacted UR5.Figure 9. OPG taken in January 2019 prior to orthodontic treatment highlighting the remaining space in the upper right quadrant following extraction of the UR6.
Discussion
Buccal segment crowding can be the result of the early loss of deciduous molars or tooth/arch size discrepancy.3 Identifying the position of the impacted teeth should be undertaken clinically with additional radiographic imaging when necessary. Digital palpation of unerupted teeth can often determine the position of the tooth relative to the arch. However, when the impacted tooth is within the line of the arch, palpation may be uneventful but as Sian2 outlines, probing around the area of impaction can sometimes identify the position of the impacted tooth indicated by limited probing depths. Intra-oral radiographs and the use of parallax can be imperative in such cases to determine both the position of the impacted tooth and presence of resorption.3,6,7 However, both Kim et al8 and Patel et al7 highlight that, due to the limitation of two-dimensional radiographic imaging with parallax, the true severity of resorption in all dimensions cannot be accurately calculated.
The invention of sectional CBCT has allowed this limitation to be overcome.9 CBCT has proven to be more effective and reliable in detecting the presence and type of resorption than intra-oral radiography. Patel et al9 concluded that, although the overall sensitivity of intra-oral radiography was relatively high in diagnosing resorption defects, it was not comparable to that of CBCT scans which had 100% accuracy in the diagnosis of resorption presence and type. As a result, cases can be diagnosed earlier with a correct and accurate diagnosis, thus facilitating the treatment and long-term management of such teeth.9 Use of CBCT following an initial examination in Case 3 could have established the presence of any resorption of the UR6 at this early stage of impaction. If absent, elective extraction of the UR4 could have been considered followed by space maintenance to facilitate the eruption of the UR5, as described in a similar case by Waterhouse and Nunn.10 Unfortunately, the later stage of impaction of the premolars on presentation in Cases 1 and 2 contraindicate this option.
Interestingly all three of the cases had reported very few, or no symptoms on initial examination despite the active resorption occurring. Several authors have previously reported the relatively asymptomatic nature of this process despite resorption being evident into pulp.10,11 Eventually two of the three individuals reported a more frequent, intense pain history similar to cases documented by Sian2 and Tracey and Lee1. In addition, Tracey and Lee1 also describe how the presence of symptoms, together with the impaction of a tooth in a crowded arch, should lead to a high level of suspicion regarding resorption of adjacent teeth. As a consequence, the necessary investigations should be undertaken.
These three cases have highlighted that although resorption of molars by impacted premolars may remain a rare phenomenon, it is possible, and when suspected, the necessary investigations should be undertaken promptly. Furthermore, sectional CBCT, with its relatively low radiation dose and superior accuracy in comparison to intra-oral radiography, should be considered at an early stage of clinical management in such cases.