Harrel SK, Molinari J. Aerosols and splatter in dentistry: a brief review of the literature and infection control implications. J Am Dent Assoc. 2004; 135:429-437
Burke FJT, Mackenzie L, Sands P. Suggestions for non-aerosol or reduced-aerosol restorative dentistry (for as long as is necessary). Dent Update. 2020; 47:485-493
As the dental profession return to practice following the recent lockdown caused by the COVID-19 pandemic, the correct use of personal protective equipment (PPE) will be essential to comply with Government guidelines and help prevent further spread of the coronavirus. At the time of writing, it is understood that a person may carry COVID-19 and be asymptomatic for a period of time, therefore proper protection for both the patient and the dental professional is critical if dental practices are to continue practising safely.
CPD/Clinical Relevance: A good understanding of PPE will be essential when dental staff return to work. The way we do dentistry will be different for some time, requiring changes to our equipment, materials and procedures.
Article
John Rafelt
The purpose of this article is to provide an understanding of the differences between masks and respirators, guiding the reader to choose the correct face covering for the treatment to be carried out and, most importantly, enabling you to keep yourself, your staff and patients safe while carrying out dental procedures.
What are we trying to stop?
In the workplace we are trying to stop the inhalation of both chemical and biological agents. Chemical agents can include things such as dusts, fumes and mists, whereas biological agents include fungi, viruses and bacteria. Viruses are generally airborne and are transmitted as an aerosol when the virus joins with a water droplet. The generation of aerosols in everyday dental practice is virtually impossible to eliminate and the dental procedures that do and do not produce aerosols have been discussed at length in the dental press, but shall not be covered in any depth within this article.
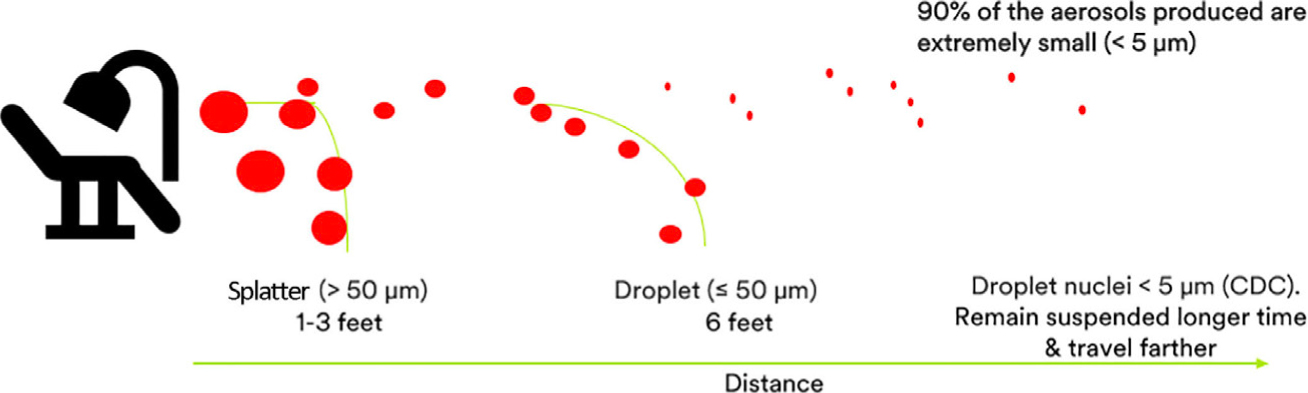
If we assume that some dental procedures produce an aerosol, then we (and our staff) need to be adequately protected from it. As shown in Figure 1, the smaller the droplet, the greater the distance it can travel. The smallest aerosols can even travel into adjacent rooms.
Figure 1. Aerosols and splatter in dentistry.1,2
Respiratory protection options
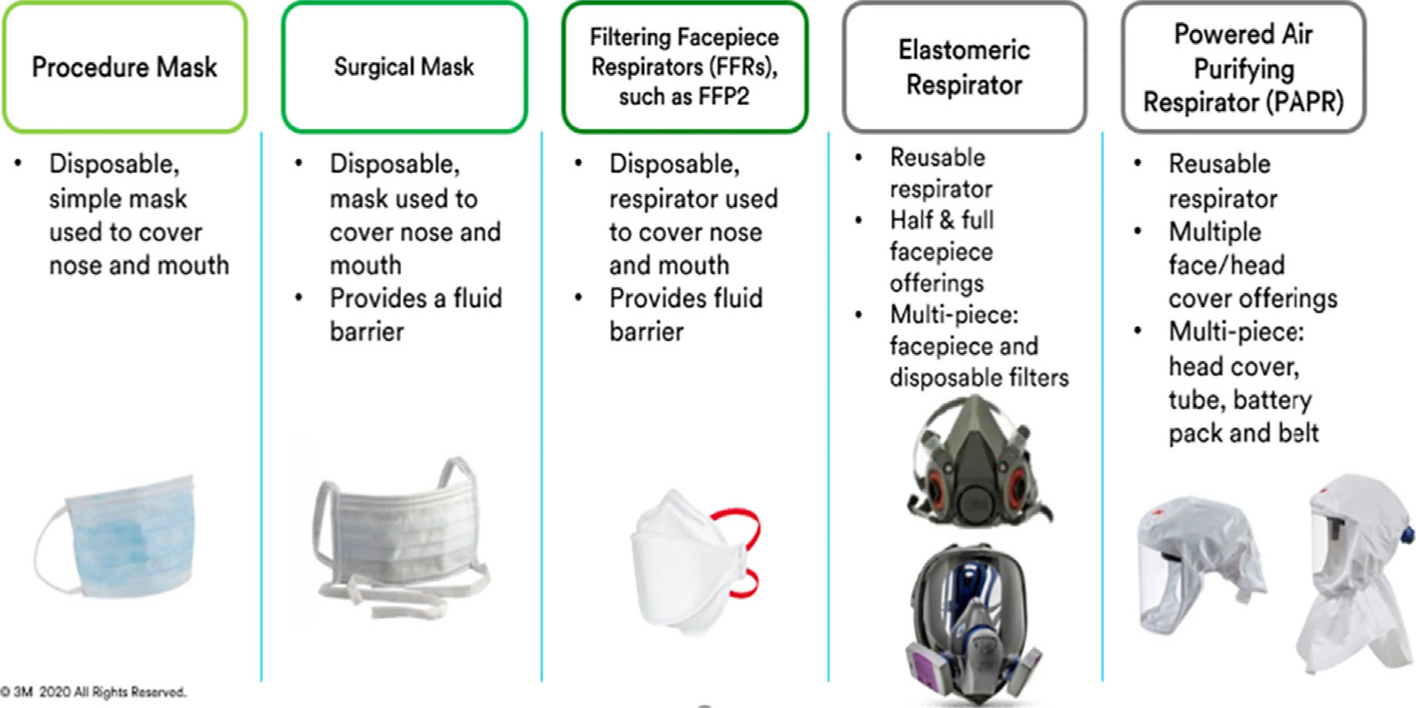
Figure 2 provides an overview of the main types of respiratory protection available on the market today. The level of protection increases as we move from the left-hand side of this table over to the right. The first column on the left-hand end covers procedure masks: these are a simple disposable cover for the nose and mouth and essentially prevent the wearer from expelling particles (droplets) into the environment. These provide little protection to the wearer from airborne aerosols. Masks are available in two types, fluid resistant and non-fluid resistant. Fluid resistant masks are generally referred to as surgical masks as they offer the wearer some protection from fluid.
Figure 2. The main types of respiratory protection available on the market.
The middle column covers respirators. The difference between a mask and respirator has caused much confusion in the last few months, so let's look at the key main differences.
Masks and respirators – what's the difference?
The primary purpose of masks is to prevent the wearer expelling particles into the environment. These do not protect the wearer from airborne aerosols. As mentioned above, some are fluid resistant. These will offer protection from splash and splatter of blood and other infectious materials. Masks do not usually fit tightly to the face and air leakage around the sides is likely.
Respirators, on the other hand, form a tight seal to the face and are designed to reduce the wearer's exposure to airborne particles. These offer different levels of protection, with FFP3 (Filtering Facepiece 3) disposable respirators offering the highest level of protection. Respirators only work correctly if there is a tight seal between the respirator and the user's face. Therefore, it is essential (and a legal requirement in the UK) that respirator wearers are face fit tested before using them in a clinical setting, this being covered in more depth later in this article. Most respirators are fluid resistant, but some on the market are not. It is important that you know if yours is fluid resistant. If not, then extra protection may also be required.
The final two columns in Figure 2 cover elastomeric respirators and powered air purifying respirators. These are not ideal for dentistry as exhaled air may not always be filtered whereas, with an unvalved FFP2 or FFP3 respirator, both the air you breath in and the air you breath out are filtered.
As well as being difficult to clean and sterilize effectively, some of the elastomeric respirators are not fluid resistant as they have been designed for industrial applications rather than healthcare.
Should I use valved or unvalved?
Valved respirators have a valve on the front to allow air to be exhaled more easily. Most valved respirators do not filter the exhaled air, so this type of respirator is not ideal for use when treating patients. Most valved respirators are ideal for protecting the wearer from viruses, but they do not protect the patient. Unvalved respirators filter both the inhaled and exhaled air, ensuring protection for both the wearer and the patient.
What is the difference between FFP2 and FFP3?
To conform with Personal Protective Equipment Directive (EN149:2001 +A1:2009), Filtering Facepieces (FFP) are graded on a one to three scale, depending on the amount of total inward leakage. The total inward leakage is defined as the sum of the filter efficiency, the efficiency of the seal between the mask and skin of the wearer, and the performance of an existing exhalation valve (if present). The minimum performance criteria for total inward leakage (TIL) are as follows:
FFP1 = TIL not greater than 22%
FFP2 = TIL not greater than 8%
FFP3 = TIL not greater than 2%.
FFP respirators should be single use and, in fact, the majority on the market are sold as single use items. Some have the letters NR and D displayed on the front of the respirator, indicating that they are not reusable (NR) and disposable (D). It is unsafe to reuse respirators without proper reprocessing/decontamination, and currently the World Health Organization has stated that medical masks and respirators are not compatible with current existing decontamination methods, as they cannot be cleaned without losing their properties. There are no standardized methods or protocols for ensuring the effectiveness or integrity of respirators after reprocessing. https://apps.who.int/iris/bitstream/handle/10665/331695/WHO-2019-nCov-IPC_PPE_use-2020.3-eng.pdf
Reports of clinicians wearing splash resistant masks over respirators to extend the respirator's life are common. Respirators do make breathing more difficult, so the introduction of an additional mask will only further decrease the ability to breath effectively. There is also the chance that the covering mask may slip during a procedure, allowing the respirator to become exposed and therefore contaminated. The majority of respirators are designed to be single use in order to protect the user and the patient. These should be treated as disposable.
So, to summarize this section, the most suitable respirators for aerosol generating dental procedures (AGPs) are unvalved FFP2 or FFP3 respirators. At the time of writing, the guidance in the UK is to use FFP3 respirators for all dental procedures that generate an aerosol.
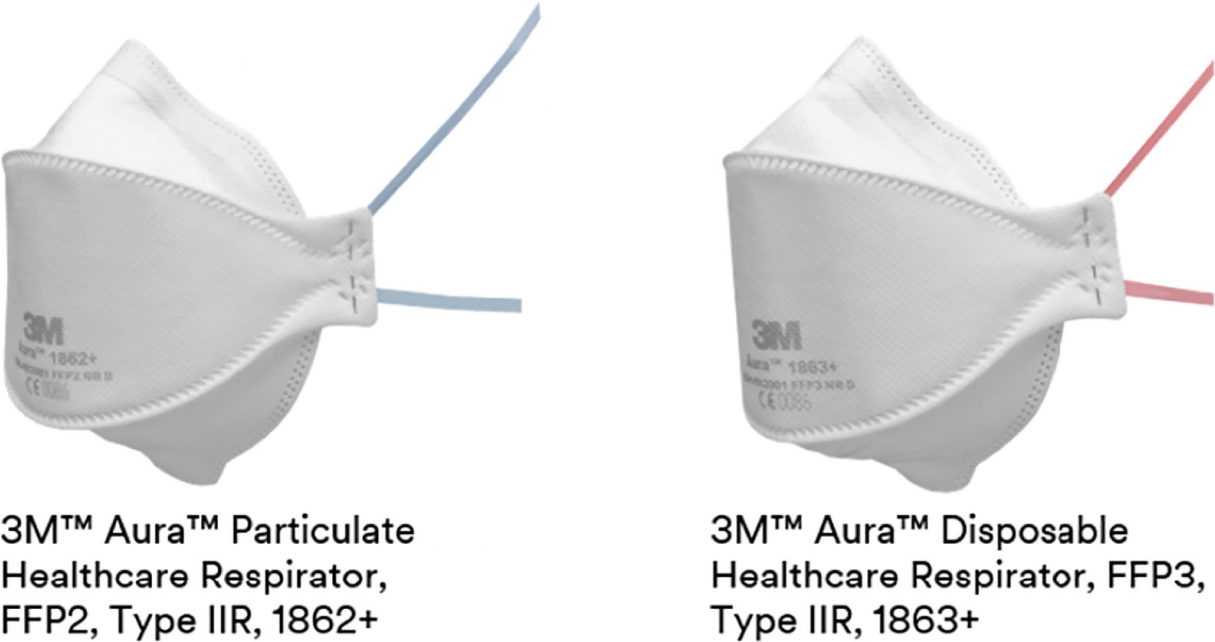
Figure 3 illustrates two surgical respirators. Both are unvalved, type IIR medical devices which are recommended for AGPs.
Figure 3. FFP2 and FFP3 respirators.Figure 4. 3M™Cavilon™No Sting Barrier Film.
What is fit testing?
Disposable respirators work effectively when there is a good seal between the edges of the respirator and the wearer's face. The instant that the seal is broken, protection is compromised, as contaminated air can leak in through any gaps. A fit test is a method for checking that a tight-fitting facepiece matches the person's facial features and seals adequately to the wearer's face. It will also help to identify unsuitable facepieces which should not be used. At the time of writing, it is a legal requirement to complete a fit test before using a respirator in the UK.
Respirators are designed to fit most people, but not everyone can use a respirator. Facial features, nose shape and other factors may impact on the ability to make a good seal. It is necessary to ensure that nothing is going to compromise the fit, so the wearer must be clean shaven, have no jewellery or piercings and not be wearing heavy makeup.
More information regarding the fit test procedure can be found at www.fit2fit.org and at the web address below.
A fit test usually lasts around 30 to 45 minutes and involves wearing a respirator inside a hood while a mist is applied. If the wearer can taste either the sweet or bitter essence in the mist, then the respirator is not fitting correctly. Once a fit check has been passed, the clinician will be able to use that specific respirator for practice. If, in the future, the operator decides to move to another type of respirator, (s)he MUST be fit checked again on the new type.
Following a successful fit check, the user must perform a user seal check each time a respirator is placed. This involves covering the placed respirator with both hands without collapsing the structure. On inhalation, the user should not feel air entering the periphery of the respirator, but should feel negative pressure as the respirator is sucked onto the face. Likewise, on exhaling, there should be no leakage around the periphery, but positive pressure should be felt under the respirator. This must be completed each time a new respirator is placed.
What if my face becomes sore?
Wearing tight-fitting respirators for long periods of time can cause irritation. Perspiration and the rubbing of the respirator can cause a skin injury, so skin protection could be required.
3M™Cavilon™No Sting Barrier Film is used extensively in healthcare settings to protect skin from moisture and friction. Available in either a swab or wipe, Cavilon™film can be applied to the face under the fitting area of a respirator.
One application at the start of the day will be sufficient for a whole day of surgery. However, some respirators on the market are adhesive and are designed to stick to the skin. Cavilon™film can be used under these, but when the respirator is removed from the face, the adhesive can remove the Cavilon™film with it. Therefore, the film should be applied each time an adhesive respirator is placed.
Back to practice
As the dental profession returns to practice, the way patients are treated is going to change for the foreseeable future. Aerosol generating procedures (AGPs) will continue to be a topic for discussion and are likely to govern our own thought processes and risk assessments as we move out of this pandemic. Discussions are already happening around the steps to be taken to minimize AGP3 and, in theory, the quantity of aerosol generated could be reduced by adopting products and techniques that are either quicker to implement or remove steps from usual procedures.
Glass ionomer usage may increase due to the need to temporize a situation or alleviate the need for an adhesive. Some do not require the use of either a conditioner or glaze (eg 3M™Ketac™Universal), so should have the ability to be placed faster. For situations where composite is required, bulk placing materials which don't require a capping layer may save time. Obviously, the majority of composites require the use of an adhesive prior to placement, several of which are available in unit dose delivery, which helps when trying to reduce cross contamination.
Indirect work is going to be a challenge moving forward as it is virtually impossible to eradicate the production of an aerosol when carrying out such procedures. However, the 3M™Protemp™Crown Temporization Material may offer a solution. These preformed, malleable composite crowns can be placed, adapted and light-cured to provide strong restorations, which are indicated for 18 months. These could be used as a temporary solution for a missing or lost crown.
Conclusion
Personal protective equipment use is critical for returning to practice. Most PPE manufacturers are facing a global demand which is outpacing their ability to supply. With a focus still being on frontline healthcare workers, PPE supply is likely to remain a challenge for some time. As a result, suppliers are providing a wide range of masks and respirators to the dental market. Some of these are high quality; some are imported from countries where standards are different from those in the EU; some have a few of the indications that dental professionals require, but not all of them; and there have been several reported cases of counterfeit PPE being offered for sale.
It is important that the dental team are educated on what they are using and therefore what is going to protect them and their patients.