Merskey H, Bogduk N. Classification of Chronic Pain. Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms, 2nd edn. Seattle: IASP Press; 1994
Katusic S, Beard CM, Bergstralh E, Kurland LT. Incidence and clinical features of trigeminal neuralgia, Rochester, Minnesota, 1945–1984. Ann Neurol. 1990; 27:89-95
Hall GC, Carroll D, Parry D, McQuay HJ. Epidemiology and treatment of neuropathic pain: the UK primary care perspective. Pain. 2006; 122:156-162
Koopman JS, Dieleman JP, Huygen FJ, de MM, Martin CG, Sturkenboom MC. Incidence of facial pain in the general population. Pain. 2009; 147:122-127
Mueller D, Obermann M, Yoon MS, Poitz F, Hansen N, Slomke MA Prevalence of trigeminal neuralgia and persistent idiopathic facial pain: a population-based study. Cephalalgia. 2011; 31:1542-1548
Pan SL, Chen LS, Yen MF, Chiu YH, Chen HH. Increased risk of stroke after trigeminal neuralgia – a population-based follow-up study. Cephalalgia. 2011; 31:937-942
Pan SL, Yen MF, Chiu YH, Chen LS, Chen HH. Increased risk of trigeminal neuralgia after hypertension: a population-based study. Neurology. 2011; 77:1605-1610
Wu TH, Hu LY, Lu T, Chen PM, Chen HJ, Shen CC Risk of psychiatric disorders following trigeminal neuralgia: a nationwide population-based retrospective cohort study. J Headache Pain. 2015; 16
Maarbjerg S, Wolfram F, Gozalov A, Olesen J, Bendtsen L. Association between neurovascular contact and clinical characteristics in classical trigeminal neuralgia: a prospective clinical study using 3.0 Tesla MRI. Cephalalgia. 2015; 35:1077-1084
Devor M, Amir R, Rappaport ZH. Pathophysiology of trigeminal neuralgia: the ignition hypothesis. Clin J Pain. 2002; 18:4-13
Moisset X, Villain N, Ducreux D, Serrie A, Cunin G, Valade D Functional brain imaging of trigeminal neuralgia. Eur J Pain. 2011; 15:124-131
Hung PS, Chen DQ, Davis KD, Zhong J, Hodaie M. Predicting pain relief: use of pre-surgical trigeminal nerve diffusion metrics in trigeminal neuralgia. Neuroimage Clin. 2017; 15:710-718
Maarbjerg S, Gozalov A, Olesen J, Bendtsen L. Trigeminal neuralgia – a prospective systematic study of clinical characteristics in 158 patients. Headache. 2014; 54:1574-1582
The International Classification of Headache Disorders. Cephalalgia. 2018; 38:1-211
Cruccu G, Finnerup NB, Jensen TS, Scholz J, Sindou M, Svensson P Trigeminal neuralgia: new classification and diagnostic grading for practice and research. Neurology. 2016; 87:1-9
Zakrzewska JM. Insights Facts and Stories behind Trigeminal Neuralgia.Gainesville: Trigeminal Neuralgia Association; 2006
Maarbjerg S, Gozalov A, Olesen J, Bendtsen L. Concomitant persistent pain in classical trigeminal neuralgia – evidence for different subtypes. Headache. 2014; 54:1173-1183
Zakrzewska JM, Padfield D. The patient's journey through trigeminal neuralgia. Pain Clinical Update. 2014; 22:1-7
Zakrzewska JM, Wu J, Mon-Williams M, Phillips N, Pavitt SH. Evaluating the impact of trigeminal neuralgia. Pain. 2017; 158:1166-1174
Zakrzewska JM, Linskey ME. Trigeminal neuralgia. Br Med J. 2014; 348
Cruccu G, Gronseth G, Alksne J, Argoff C, Brainin M, Burchiel K AAN-EFNS guidelines on trigeminal neuralgia management. Eur J Neurol. 2008; 15:1013-1028
Zakrzewska JM, Jorns TP, Spatz A. Patient led conferences – who attends, are their expectations met and do they vary in three different countries?. Eur J Pain. 2009; 13:486-491
Trigeminal Neuralgia Joanna M Zakrzewska Dental Update 2024 46:8, 707-709.
Authors
Joanna MZakrzewska
MD, FDS RCS, FFD RCSI, FFP MRCA, FHEA
Professor of Pain in Relation to Oral Medicine, Clinical and Diagnostic Oral Sciences Dental Institute, Barts and the London Queen Mary's School of Medicine and Dentistry, Turner Street, London E1 2AD, UK
Trigeminal neuralgia is one of the most severe facial pains that patients can experience. This unpredictable, episodic pain, mostly unilateral in the distribution of the trigeminal nerve, results in recurrent shooting pain lasting for seconds to minutes. It is light touch provoked and therefore prevents patients from eating and touching their face, and so has a significant impact on quality of life. Patients often consult a dentist because it usually presents like dental pain. Dentists need to avoid irreversible dental treatment. Response to carbamazepine is good but tolerability is poor. Surgical options are available and are generally successful. Patients can gain further information from a patient support group, such as Trigeminal Neuralgia Association UK.
CPD/Clinical Relevance: Although rare, trigeminal neuralgia patients often present to dentists who therefore need to recognize it as a non-dental cause of pain in order to avoid irreversible dental treatment.
Article
Trigeminal neuralgia (TN) is described as a: ‘sudden, usually unilateral, severe, brief, stabbing, recurrent pain in the distribution of one or more branches of the trigeminal nerve’, which is triggered by light touch activities.1
Epidemiology
Trigeminal neuralgia is considered to be a rare disease and the estimated prevalence from an old study in the USA put it at 4.1/10,000.2 More recent studies in the UK3 and Holland,4 using data from primary care records, suggests a higher incidence of 8 to 12.6 per 100,000 per annum. In a study in Germany, where all the diagnoses were validated by specialists, a lifetime prevalence of 0.3% (95% CI 0.1–0. 5%) was estimated.5 Up to 90% of patients develop TN after age 50, with the peak between 60–70 years, and there is a slight predominance in women. It can occur in young people and even children. The disease most frequently linked with TN is multiple sclerosis (in around 5–10% of cases). In this group, it occurs in a younger age group and there is an increased frequency of bilateral pain. Tumours account for a very small number of cases. Hypertension is a risk factor and strokes more likely.6,7 Data from a population-based study in Taiwan highlights increased risk of depression, anxiety and sleep disorder after diagnosis of TN.8 There are reports of familial links.
Pathophysiology
Trigeminal neuralgia is a neurological pain, the cause of which is still not completely understood. In many patients, a strongly pulsating blood vessel is found to be pressing on the trigeminal nerve at a point where the cells producing myelin change from the peripheral to central type.9 This causes demyelination and so sets up a cross circuit between those nerve fibres which relay light touch sensations and those which relay pain signals, the so-called ignition hypothesis.10 The result is intermittent but excruciating and debilitating pain. There is growing evidence that patients with TN have a number of abnormalities of their nerve functions, including abnormal sodium channels, nociceptive inhibitory pathways and possible inflammatory changes, but more research needs to be carried out to establish the causes as it could be multifactorial.11,12
Clinical features
Although it would appear from the diagnostic criteria that the disorder is easy to diagnose, it is being increasingly recognized that this is not the case and more detailed clinical characteristics are now being reported.13,14 It has been generally accepted that, in those patients in whom a nerve compression has been identified on Magnetic Resonance Imaging (MRI), the term classical TN is used, whereas in those patients where no cause is found, it is called idiopathic TN. Secondary TN is that in which a cause is identified, eg MS, vascular anomalies or tumours.15 The principal features are shown in Table 1, alongside the way patients describe their pain.16
Feature
Clinical Feature
Patient Description
Onset
Sudden and memorable
‘While brushing my teeth one morning I got a bolt of lightning exploded in my face’
Timing
Each attack lasts seconds to minutes
‘Within 30 minutes I had three jolts of pain each lasting 30-45 seconds’
Periodicity
Number per day can vary from 4-50, can get series of stabsRemission periods of weeks or years
‘Within 30 minutes I had three jolts of paineach lasting 30-45 seconds’‘I was having 20-40 attacks per day.The tic episodes would sometimes completely disappear for as long as six months, then reappear out of nowhere’
Site
Trigeminal nerve distribution, most common lower part of the face and intraoral
‘My right upper and lower molars, as well as my right lateral tongue, lower half of the right side of my face’
Character
Shooting, sharp, electric
‘Lightning bolt, inserted a knife in my cheek, twisted it and pulled it out’
Severity
Severe
‘The intensity is unlike anything I could ever imagine, the pain is so strong it steals your mind, it takes over all your thoughts, it is excruciating’
Provoking factors
Light touch
‘Everyday functions of talking, yawning, brushing one's teeth, eating, blowing one's nose are punished by deep, mean long stabs of electric current’
Relieving factors
Keeping still, medications
‘It helped not to move my face at all’
Associated factors
May be some background dull aching pain Occasionally, autonomic features Weight loss
‘A throbbing, burning pain, lost 40 pounds in the last two months’
Impact
Depression, anxiety, decreased quality of life
‘Isolation, depression, fear of increasing pain are just some of the emotions I try to work through. This pain has taken over my life’
Many patients will first visit a dentist as the pain often presents intra-orally and, for that reason, patients are convinced that the cause is dental. Trigeminal neuralgia presents abruptly with patients remembering exactly what they were doing during their first attack, called a memorable onset. It is important to establish the timing. It is an episodic pain and drawing diagrams and asking patients to label them can help in differentials.
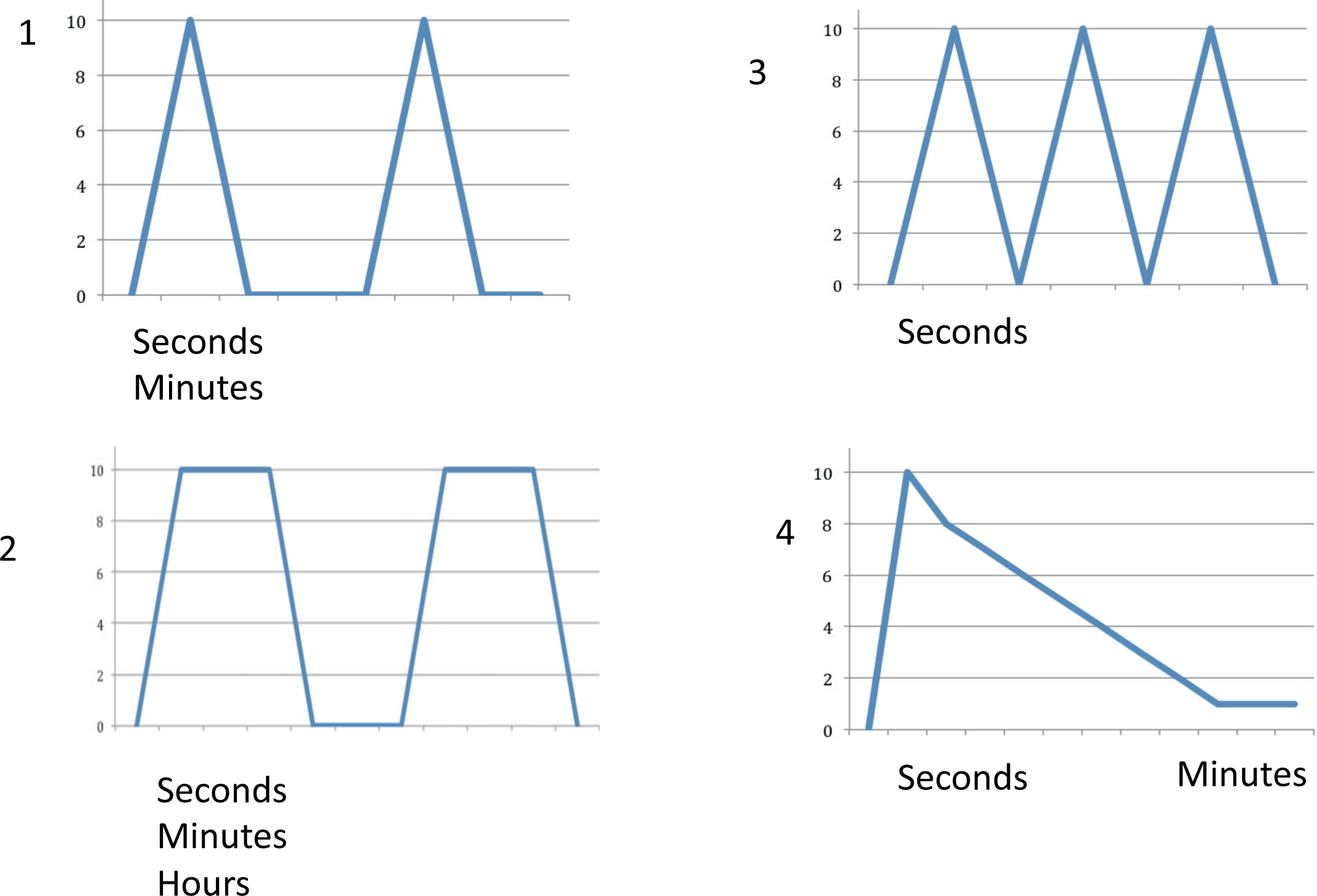
Take a look at the patterns in Figure 1. A pattern like number 1 is the most classical type but, when the pain episode is severe, it can be like number 3, where there is a series of stabs lasting seconds but in quick succession before there is a refractory period when pain cannot be triggered. If the pain is number 2 and the episode lasts for hours, it is unlikely to be TN. However, there can be an afterpain that is less severe and more burning, as shown in number 4. This more prolonged pain has variously been termed concomitant pain or type 2 TN.17 The pain begins at the start of light touch, eg eating, rather than on the rebound, as occurs with a cracked tooth. Remission periods are common and more likely at the start of the condition. These periods can last for months before the next relapse. However, these periods are totally unpredictable and vary from patient to patient. The severity can be so high that patients cannot eat, swallow their saliva and become dehydrated and lose weight.
Figure 1. Timing of attacks. X axis: severity on a scale of 0-10, can vary in severity. Y axis time.
It is important to elicit the sharp, stabbing, shooting, electrical character of the pain by asking ‘How does it feel?’ and encouraging patients to use metaphors. We have done this using images.18 Sleep often brings relief, except when going through a very severe bout. Some patients may report intermittent, autonomic features on the painful side only at times of pain, such as red eye, runny eye, drooping of the eyelid, redness of the cheek or nasal changes. These autonomic features may, however, suggest another diagnosis such as SUNA, short unilateral neuralgiform pain with autonomic features. Very rarely do they report other types of chronic pain. Unequal use of the mouth can lead to pain in the muscles of mastication.
On careful examination some patients may have subtle sensory changes. Touching a trigger point can elicit an attack of pain and this can be diagnostic. Intra-oral examination can show decreased oral hygiene on the side of the pain.
Patients with TN experience considerable activity limitation and the limitation is particularly pronounced with activities that involve the face (eg eating, talking, touching the face, being intimate). Weight loss can be substantial as a result. Social isolation is common as patients cannot eat at social events. Fear is very pronounced as they can never predict when they will get their next attack of pain. Over 50% of the patients take a significant amount of time off work. The disability experienced by the patients is associated with high levels of anxiety (>50%), and over 40% are depressed, with 75% showing evidence of catastrophizing.19 From information from the Trigeminal Neuralgia Association (TNA UK) and the national press, eight people are known to have committed suicide as a result of TN since 1996.
Differential diagnosis
It is difficult to make the initial diagnosis as the patient will not have been experiencing the pain for a long time and no remission periods are reported. Patients will report a lack of response to paracetamol and NSAIDs. It is certainly much more likely to be a dental cause, especially when patients have a heavily restored dentition. However, the dentist must be guided by the history, and use examination and imaging when making the diagnosis. A trial of carbamazepine can often be diagnostic as, in the initial phases of the condition, it can result in complete pain relief. Trigeminal neuralgia can be the first presenting episode for multiple sclerosis and its presentation is the same as for classical TN, although patients are more likely to have bilateral episodes of pain. Glossopharyngeal neuralgia is extremely rare and can be difficult to differentiate from TN. The pain is felt either in the throat on swallowing or in the ear. If the pain is centred over the temple region, is of longer duration and the patient is over 50, C reactive protein and an ESR must be done to rule out temporal arteritis. Other neuralgic pains, such as post herpetic neuralgia, will be associated with a history of previous herpes zoster and the pain is continuous. Trigeminal neuropathic pain will be linked to a traumatic event, be it dental or facial trauma.
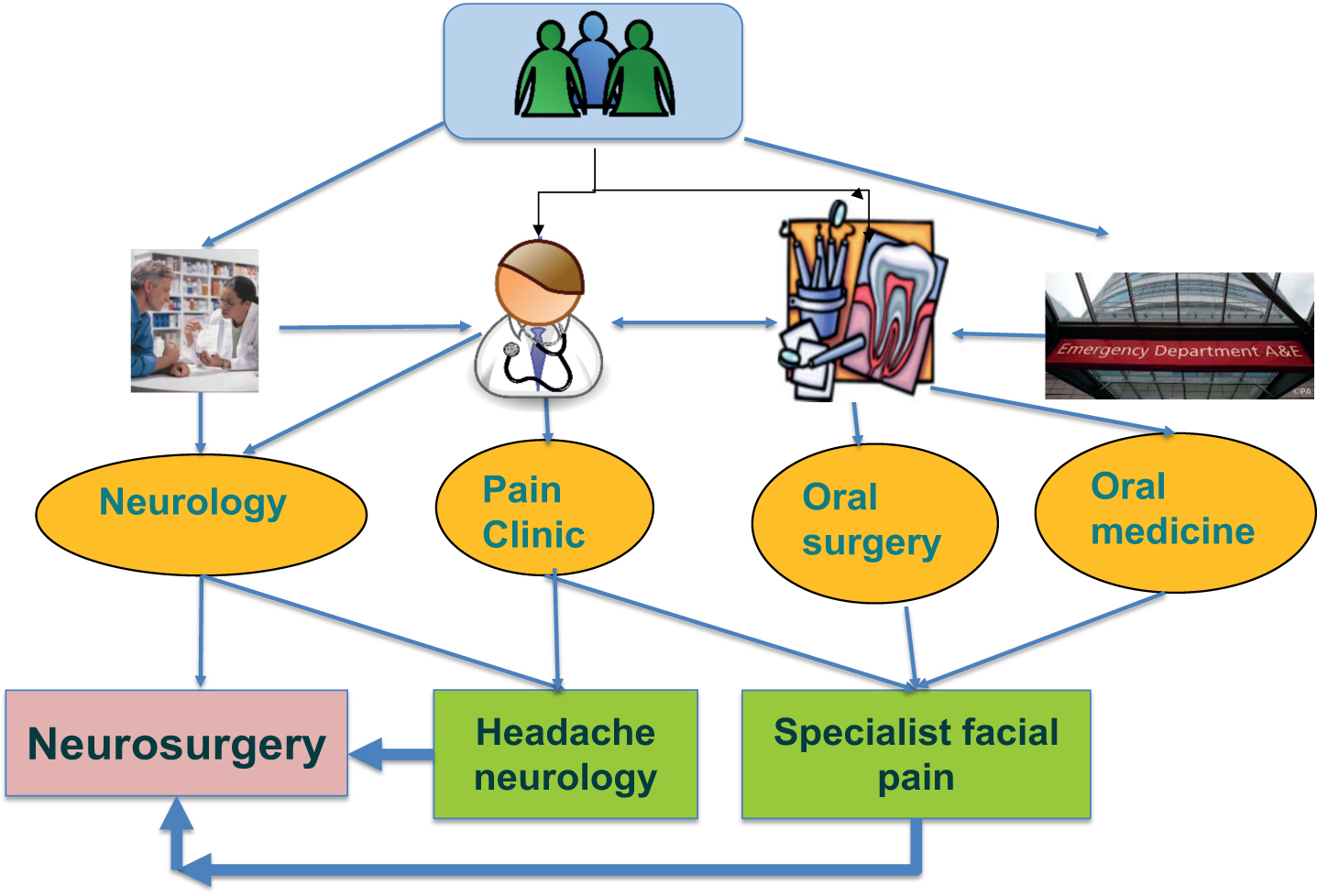
Our UK study shows that it takes, on average, four years for a patient to receive the correct treatment plan and 83% would have been seen by at least one other specialist and one third by two or more specialists before a suitable management plan is made.19 As the trigeminal nerve also supplies the teeth, 70% of patients will have consulted a dentist and 8% will have had treatment, some of which was unnecessary and even harmful. Who the patient consults first will often determine the secondary referral and, as shown in Figure 2, this often leads to inappropriate care and a need for further referral. It is important to identify who has an interest in this condition in your district. Patients are prepared to travel long distances to get appropriate care.
Figure 2. Pathways of referral for patients with trigeminal neuralgia.
Investigations
It is important to rule out any dental causes, therefore local imaging is required before other investigations are done. Specialists will do MRIs to determine if there is a secondary cause.
Management
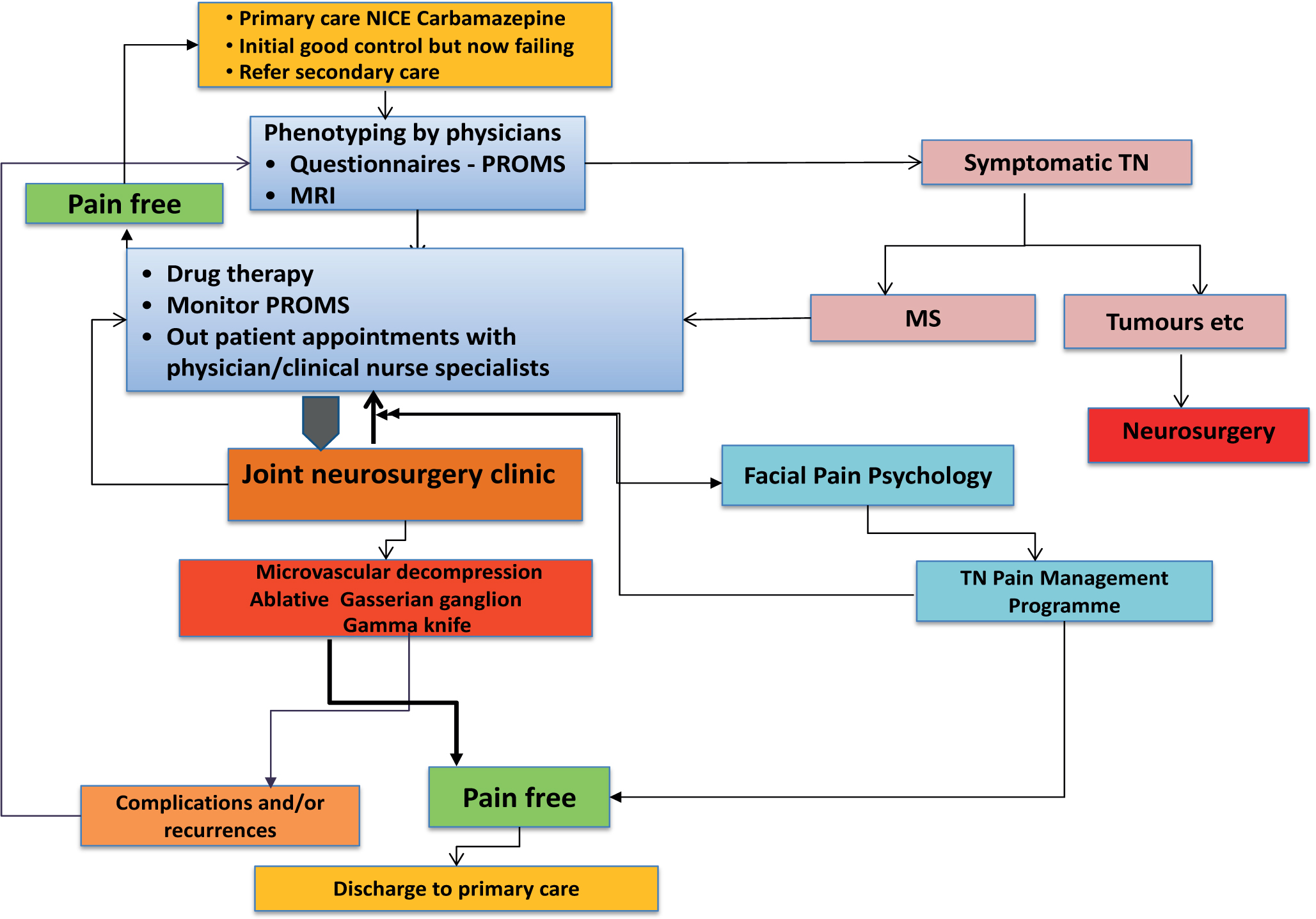
The wide range of treatments, both medical and surgical, currently in use for TN is ample proof that there is no simple answer on how the condition should be managed.20 The level of evidence for current treatments is extremely poor due to a lack of high quality studies.21 A variety of outcome measures for treatment are used which makes comparisons between treatments virtually impossible. A 50% reduction in pain is considered an effective outcome for medical management, but patients expect 100% pain relief from surgical procedures, which can be obtained in some patients. It is important that clinicians managing these patients use internationally approved guidelines and have as far as possible evidence-based care pathways. An overall care pathway, as used at the UCLH NHS Foundation Trust UK, is shown in Figure 3. This is similar to that used by the headache neurologists in Denmark. It is important that there is a multidisciplinary team.22
Figure 3. Care pathway for trigeminal neuralgia used at UCLH NHS Foundation Trust UK (MS - multiple sclerosis; PROMS – patient-related outcome measures).
Pharmacological
No analgesics, including opioids, provide adequate pain relief and the mainstay remains anti-epileptic drugs. The first line drug is carbamazepine and it needs to be started at a low dose, eg 100 mg two or three times a day and gradually increased up to 800 mg daily. Slow escalation helps to reduce side-effects. It will have an effect in 24 hours. Oxcarbazepine is another alternative which has fewer side-effects and fewer drug interactions. Other drugs that can be prescribed by the GP include lamotrigine, baclofen, gabapentin and pregablin. All will result in significant cognitive side-effects, such as memory problems, drowsiness, whereas more peripheral side-effects include nausea and weight gain. It is useful to encourage patients to keep a diary when the pain becomes more severe or when changing drugs. The diary can also be used to determine if a remission period has occurred.
Surgical
When the side-effects of medication become intolerable or the drugs themselves cease to be effective, various surgical procedures can be tried, but here there are widely different techniques used and outcomes are varied and result in complications which can affect quality of life.
Some of these surgical procedures are deliberately destructive to the trigeminal nerve and can lead to loss of sensation in the face. The only one that is non-destructive, microvascular decompression (repositioning an offending blood vessel which may be pressing on the nerve), is a major neurosurgical procedure with potential for significant complications. It has recently been suggested that only those patients who have both compression of the trigeminal nerve in the root entry zone as well as anatomical changes (thinning of the nerve or distortion of the nerve) should be subjected to a microvascular decompression. Microvascular decompression offers the longest pain relief period (70% of patients remain pain free and still off drugs after 10 years) but this treatment may not always be appropriate due to a patient's age or physical condition. The other procedures are mainly done at the Gasserian ganglion level, radiofrequency thermocoagulation, glycerol rhizotomy or balloon compression. Stereotactic radiosurgery aims to irradiate the trigeminal nerve in the posterior fossa and its effects are delayed. All these procedures can result in varying levels of sensory loss and, on average, result in four years of pain freedom.
Acute attacks
Many patients will get flare ups which can be so severe that they attend accident and emergency units. Often, they are given opioids which do little to relieve their pain. To date the evidence for managing these is of low quality. However, it is noted that local anaesthetics injected into trigger areas can be helpful, as shown by a study that added ropivicaine injections to the use of gabapetin. The two main sites would be infra-orbital nerve and inferior dental nerve blocks. A lidocaine injection followed by a marcaine injection to prolong the effect can be helpful. This can be done daily till the increased dose of medication has had time to take effect.
Other
It is important to take a biopsychosocial approach and a course of cognitive behaviour management can be helpful. Through a patient support group, TNA UK patients can meet fellow sufferers and also have access to high quality information www.tna.org.uk. They also hold meetings that are attended by patients and healthcare professionals.23 The Brain and Spine Foundation publish a useful booklet on facial pain which provides details of TN and other related conditions and can be downloaded from https://www.brainandspine.org.uk/