Wong JY, Pfahnl AC. 3D printing of surgical instruments for long-duration space missions. Aviat Space Environ Med. 2014; 85:758-763
Rastogi VK, Smith LS, Schmid MJ, Parsons LM, Grant CG, Kondor S, Macedonia C. A novel approach for assured sterility of medical devices. J Med Device. 2013; 7:030947-51
Bletzinger KU, Ramm E. Structural optimization and form finding of light weight structures. Comput Struct. 2001; 79:2053-2062
Patent application publication: Pub No. US 2015/0366635 A1. 2015;
Byun C, Kim C, Cho S, Baek SH, Kim G, Kim SG, Kim SY. Endodontic treatment of an anomalous anterior tooth with the aid of a 3-dimensional printed physical tooth model. J Endod. 2015; 41:961-965
Miyazaki T, Hotta Y, Kunii J, Kuriyama S, Tamaki Y. A review of dental CAD/CAM: current status and future perspectives from 20 years of experience. Dent Mater J. 2009; 28:44-56
Colpani JT, Borba M, Della Bona Á. Evaluation of marginal and internal fit of ceramic crown copings. Dent Mater. 2013; 29:174-180
Anunmana C, Charoenchitt M, Asvanund C. Gap comparison between single crown and three-unit bridge zirconia substructures. J Adv Prosthodont. 2014; 6:253-258
Tamac E, Toksavul S, Toman M. Clinical marginal and internal adaptation of CAD/CAM milling, laser sintering, and cast metal ceramic crowns. J Prosthet Dent. 2014; 112:909-913
E Silva JS, Erdelt K, Edelhoff D, Araújo É, Stimmelmayr M, Vieira LC, Güth JF. Marginal and internal fit of four-unit zirconia fixed dental prostheses based on digital and conventional impression techniques. Clin Oral Investig. 2014; 18:515-523
Song TJ, Kwon TK, Yang JH, Han JS, Lee JB, Kim SH, Yeo IS. Marginal fit of anterior 3-unit fixed partial zirconia restorations using different CAD/CAM systems. J Adv Prosthodont. 2013; 5:219-225
Srikakula NK, Babu CS, Reddy JR, Saiprasad SH, Raju AS. Comparision of marginal fit of zirconium oxide copings generated using four different CAD-CAM systems – an in vitro study. J Res Adv Dent. 2014; 3:163-171
Sailer I, Fehér A, Filser F, Gauckler LJ, Luthy H, Hammerle CH. Five-year clinical results of zirconia frameworks for posterior fixed partial dentures. Int J Prosthodont. 2007; 20:383-387
Bornemann G, Lemelson S, Luthardt R. Innovative method for the analysis of the internal 3D fitting accuracy of Cerec-3 crowns. Int J Comput Dent. 2001; 5:177-182
Park JY, Kim HY, Kim JH, Kim JH, Kim WC. Comparison of prosthetic models produced by traditional and additive manufacturing methods. J Adv Prosthodont. 2015; 7:294-302
Mai HN, Lee KB, Lee DH. Fit of interim crowns fabricated using photopolymer-jetting 3D printing. J Prosthet Dent. 2017; 118:208-215
Yahata Y, Masuda Y, Komabayashi T. Comparison of apical centring ability between incisal-shifted access and traditional lingual access for maxillary anterior teeth. Aust Endod J. 2017; 43:123-128
Gok T, Capar ID, Akcay I, Keles A. Evaluation of different techniques for filling simulated C-shaped canals of 3-dimensional printed resin teeth. J Endod. 2017; 43:1559-1564
Patel S, Aldowaisan A, Dawood A. A novel method for soft tissue retraction during periapical surgery using 3D technology: a case report. Int Endod J. 2017; 50:813-822
Robberecht L, Chai F, Dehurtevent M, Marchandise P, Bécavin T, Hornez JC, Deveaux E. A novel anatomical ceramic root canal simulator for endodontic training. Eur J Dent Educ. 2017; 21:e1-e6
Zehnder MS, Connert T, Weiger R, Krastl G, Kühl S. Guided endodontics: accuracy of a novel method for guided access cavity preparation and root canal location. Int Endod J. 2016; 49:966-972
Shi X, Zhao S, Wang W, Jiang Q, Yang X. Novel navigation technique for the endodontic treatment of a molar with pulp canal calcification and apical pathology. Aust Endod J. 2018; 44:66-70
Obregon F, Vaquette C, Ivanovski S, Hutmacher DW, Bertassoni LE. Three-dimensional bioprinting for regenerative dentistry and craniofacial tissue engineering. J Dent Res. 2015; 94:143-152
Bertassoni LE, Cecconi M, Manoharan V, Nikkhah M, Hjortnaes J, Cristino AL Hydrogel bioprinted microchannel networks for vascularization of tissue engineering constructs. Lab Chip. 2014; 14:2202-2211
Miller JS, Stevens KR, Yang MT, Baker BM, Nguyen DH, Cohen DM Rapid casting of patterned vascular networks for perfusable engineered three-dimensional tissues. Nat Mater. 2012; 11:768-774
Hanson Shepherd JN, Parker ST, Shepherd RF, Gillette MU, Lewis JA, Nuzzo RG. 3D microperiodic hydrogel scaffolds for robust neuronal cultures. Adv Funct Mater. 2011; 21:47-54
Nakao K, Morita R, Saji Y, Ishida K, Tomita Y, Ogawa M The development of a bioengineered organ germ method. Nat Methods. 2007; 4:227-230
Ikeda E, Morita R, Nakao K, Ishida K, Nakamura T, Takano-Yamamoto T Fully functional bioengineered tooth replacement as an organ replacement therapy. Proc Natl Acad Sci. 2009; 106:13475-13480
Kim K, Lee CH, Kim BK, Mao JJ. Anatomically shaped tooth and periodontal regeneration by cell homing. J Dent Res. 2010; 89:842-847
Zhang W, Ahluwalia IP, Yelick PC. Three dimensional dental epithelial-mesenchymal constructs of predetermined size and shape for tooth regeneration. Biomaterials. 2010; 31:799-8003
Lipson H. New world of 3-D printing offers “completely new ways of thinking”: Q&A with author, engineer, and 3-D printing expert Hod Lipson. IEEE Pulse. 2012; 4:12-14
Schubert C, Van Langeveld MC, Donoso LA. Innovations in 3D printing: a 3D overview from optics to organs. Br J Ophthalmol. 2014; 98:159-161
Cui X, Boland T, D'Lima DD, Lotz MK. Thermal inkjet printing in tissue engineering and regenerative medicine. Recent Pat Drug Deliv Formul. 2012; 6:149-155
Gross BC, Erkal JL, Lockwood SY, Chen C, Spence DM. Evaluation of 3D printing and its potential impact on biotechnology and the chemical sciences. Anal Chem. 2014; 86:3240-3253
Ozbolat IT, Yu Y. Bioprinting toward organ fabrication: challenges and future trends. IEEE Trans Biomed Eng. 2013; 60:691-699
Chiu YC, Fang HY, Hsu TT, Lin CY, Shie MY. The characteristics of mineral trioxide aggregate/polycaprolactone 3-dimensional scaffold with osteogenesis properties for tissue regeneration. J Endod. 2017; 43:923-929
A review of additive manufacturing in conservative dentistry and endodontics part 2: applications in restorative dentistry and endodontics Peddi Shanmukh Srinivas TS Ashwini MG Paras Dental Update 2024 46:3, 707-709.
Authors
Peddi ShanmukhSrinivas
Postgraduate Student, Department of Conservative Dentistry and Endodontics, JSS Dental College and Hospital, Jagadguru Shree Shivaratheeshwara University, Mysuru, India
Postgraduate Student, Department of Conservative Dentistry and Endodontics, Maratha Mandal's Nathajirao G Halgekar Institute of Dental Sciences, Belgaum, Karnataka, India
Faculty, Department of Conservative Dentistry and Endodontics, JSS Dental College and Hospital, Jagadguru Shree Shivaratheeshwara University, Mysuru, India
The field of science and research is dynamic and the scientific disciplines of restorative dentistry and endodontics is no exception. The practice of dentistry and the technology involved has evolved hugely from the traditional to the contemporary. As a result of continual developments in technology, newer cutting edge methods in production and treatment have evolved. This paper explores the scope of additive manufacturing technology in restorative dentistry and endodontics, progress achieved in this field, practicality hurdles, and a promising future that this technology might provide if harnessed to its full potential.
CPD/Clinical Relevance: This paper gives an update on current concepts of additive manufacturing being employed in the field of restorative dentistry and endodontics for clinical practice, academic progress and translational research.
Article
Manufacture of clinical instruments
A study conducted by Wong and Pfahnl evaluated the feasibility of fused deposition modelling (FDM) 3D printing 10 Acrylonitrile Butadiene Styrene (ABS) thermoplastic surgical instruments.1 All simulated preparation, draping, incising, and suturing tasks were successfully performed using 3D printed instruments. All 13 surgeons were in agreement that the 3D printed instruments performed adequately, and experienced operators would be able to adapt using the 3D printed thermoplastic surgical instruments. In future, it will be feasible to 3D print surgical tools pre-operatively on demand for dental procedures. This production method has an inherent advantage over sterilization as heating of the thermoplastic filament during the FDM printing process can sterilize the printed product.1 A study found that the high temperature (300–311°C) of the FDM 3D printing process sterilized 18 of 20 tested ABS thermoplastic instruments fabricated on a Stratasys Dimension u Print Plus SE printer.2
Manufacture of complex file structures for endodontic filing
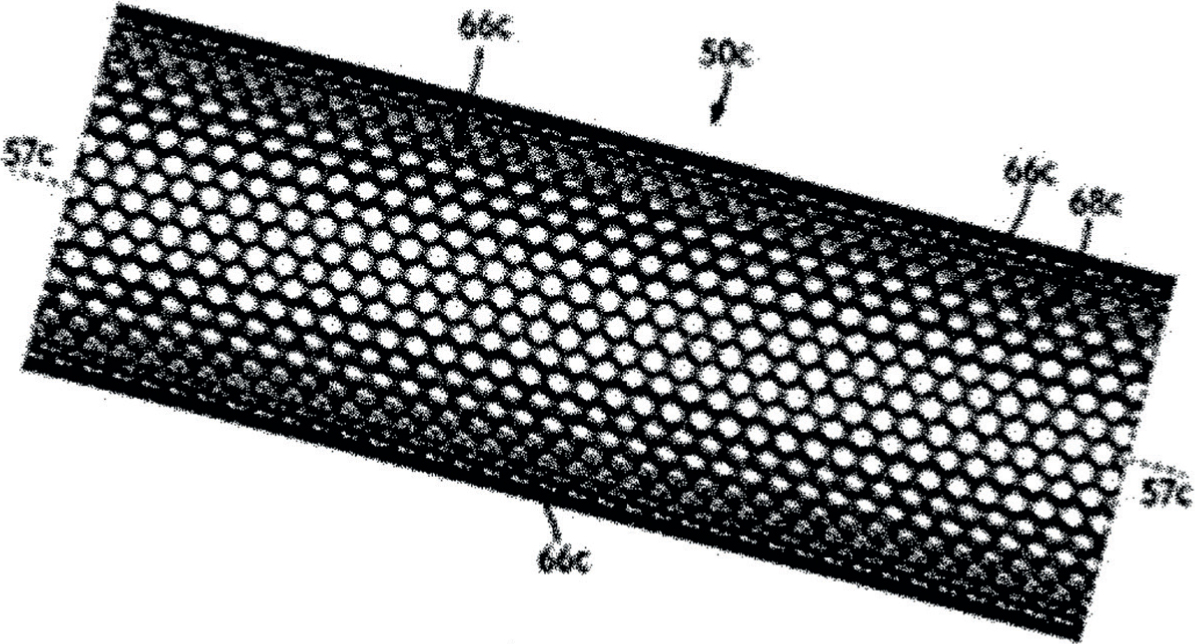
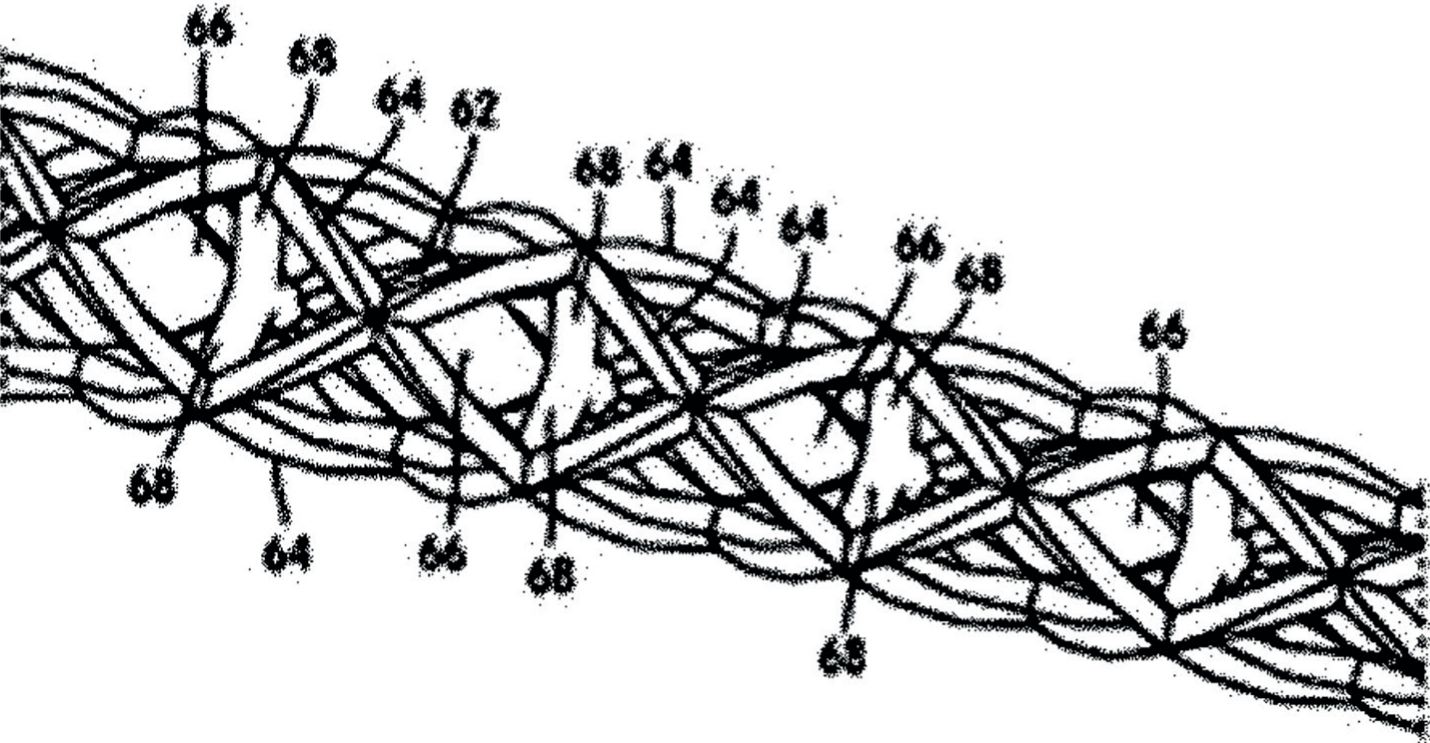
Additive manufacturing technologies have enabled the manufacture of complex cross-sectional areas like the honeycomb cell.3 For instance, Figure 1 shows a hybrid design where the endodontic instrument may shape the root canal apically to allow irrigants to clean the canal thoroughly apically and provide for a shape for obturation, while in the mid root and coronal aspects it is allowed to expand and collapse in order to allow the endodontic instrument to adapt to natural root anatomy. It emphasizes how 3D printing makes it a possibility to print tangible and complex structures.4 Another way of using 3D printing technology is to allow for the support structures internally.4Figure 2 shows an example of internal struts to support the structure of the stent design. Other alternatives would be to alter the width and the thickness of different strut pieces to allow for more support or flexibility in different regions of the file.4
Figure 1. Hollow file system designed to allow flow of irrigants within file.Figure 2. Internal support struts to support stent design.
Clinical treatment
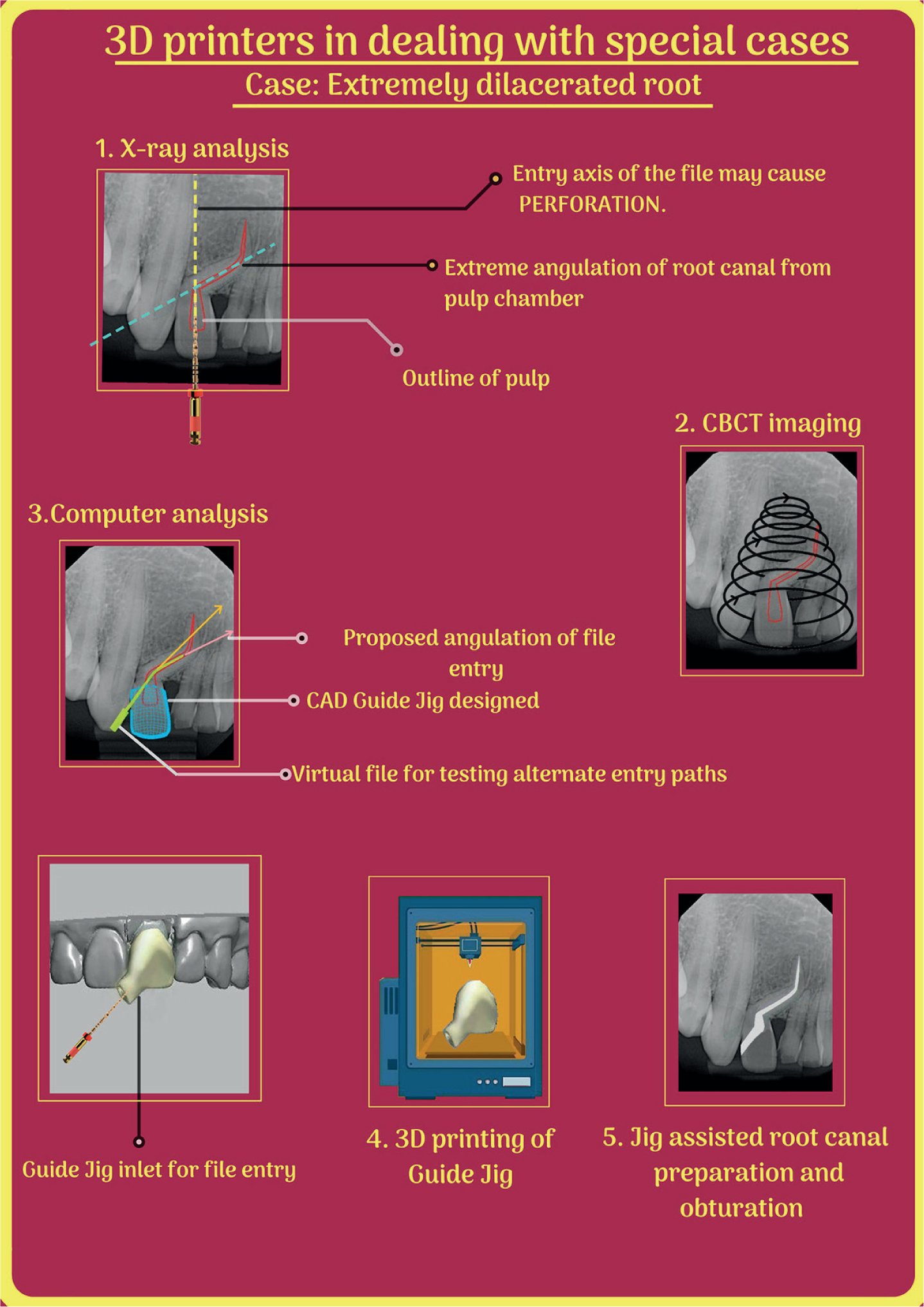
Clinical cases have been reported where 3D printing has been used for successful management of various conditions. Byun et al performed endodontic treatment of a 12-year-old male patient referred for an upper right maxillary tooth.5 The subject tooth showed Class 2 mobility, with swelling and a sinus tract in the buccal mucosa and periapical radiolucency. The tooth presented a very narrow structure between the crown and root due to distal concavity and severe dilacerations of the root; a previous convention approach led to perforation.5 A translucent physical tooth model carrying the information on internal root canal structures was printed by a 3D printing process through the data acquisition from CBCT scanning of the tooth. A custom-made guide jig was fabricated employing the tooth model to achieve a safe and precise working path.5
Results
Endodontic procedures including access cavity preparation were performed using the physical tooth model as a guide jig and, after 7 months follow-up, the endodontically treated tooth showed complete periapical healing with no clinical signs and symptoms (Figure 3).5
Figure 3. Infographic on uses of 3D printing in special cases.
Ceramic crowns
Dentistry has a long history of technological development and innovation in fabrication of dental prostheses to recover a patient's tooth function.6 Metal ceramic is a very common material used worldwide, and it has been successfully used as the gold standard for its excellent performance in oral stability, aesthetic value and marginal adaptation.7,8,9
In recovery, using a dental prosthesis, marginal adaptation is an important factor.7 An inappropriate margin could cause a minute gap between the abutment tooth and prosthesis, which may lead to a vicious sequelae of plaque accumulation, secondary caries, microleakage, inflammation after endodontic treatment, or periodontal disease.9,10,11,12 In addition, according to previous research, a defective margin may cause a failure of the long-term preservation of the prosthesis, resulting in an increase of prostheses failure rate.13
Conventional lost wax fabrication method for fabrication of prostheses includes a series of processes involving impression registration of a patient's oral cavity, pouring cast, producing a wax pattern, followed by performing investing, casting and polishing. During this process, the risk of inaccuracy may increase due to the properties of the material used, laboratory conditions and human error. In addition, labour charges could also increase cost.6,7,8,9
To address above-mentioned hurdles, an automated computer-aided milling (CAM) system was introduced to the dental field.6,9 The CAM system is a type of subtractive manufacturing that cuts the materials to the desired shape and size. It enables a larger quantity of production than traditional methods, is easy to use, saves the time and made it possible to eliminate human error. Since its advent, the CAM system was being widely used.9 However, Bornemann et al showed that this system tends to reduce accuracy through the scanning process, software design, milling and a number of other related processes.14 This results in too much consumption of raw material, and the wear of bur leading to increased cycles of bur replacement for milling.
‘Micro-SLA’ is characterized with high accuracy and, due to its high resolution, it is more appropriate for manufacturing the dental prosthesis than any other printer. Also, compared to other 3D printers, it is cheaper and faster (14 mm/hour on the basis of the vertical standard).15
According to a study comparing marginal adaptability of ceramic crowns fabricated using the ‘Micro-SLA’ method, traditional lost wax technique, milling technique and multijet modelling, conducting the marginal adaptation using ‘Micro-SLA’ was comparable to the traditional lost wax technique, which happens to be the gold standard.9 Hence, the study concluded that the ‘Micro-SLA’ generated ceramic crowns could be a potential replacement.
An in vitro study conducted by Mai et al to evaluate the fit of interim crowns fabricated using polyjet 3D printing and comparing it with crowns fabricated using milling and compression molding methods, the milling and polyjet groups showed more accurate results in the proximal and marginal regions. In the axial regions, even though the mean discrepancy was smallest in the molding group, the data showed overall large deviations. In the occlusal region, the polyjet group was most accurate, and compared with the other groups, the milling group showed larger internal discrepancies.16
Tamac et al compared marginal and internal adaptation of ceramic facing metal crowns fabricated using CAD/CAM milling, a direct laser sintering method of 3D printing (DLS), and traditional casting, and an evaluation was conducted using a silicon impression technique observed under a binocular stereomicroscope.9 They concluded that all crowns fabricated with DLS showed highest discrepancy of the lot in the occlusal and axio-occlusal region. In other regions, adaptation of all three groups was comparable.9
Clinical research
A study conducted by Yahata et al compared the apical centring ability of incisal shifted access (ISA) with that of traditional lingual access (TLA). Fifteen 3D printed resin models were prepared from the computed tomography data from a human maxillary central incisor. Results showed that access cavity preparation has a significant effect on apical centring ability and ISA is beneficial for maintaining apical configuration.17 3D printed models assisted in standardizing the procedure and prevented the hassles of sample collection.
Another study, conducted by Gok et al to evaluate the efficiency of different obturation techniques in C-shaped canals, to standardize the canal anatomy of a mandibular molar with a C1 root canal configuration, was scanned with CBCT imaging, and generated DICOM images which were 3D printed.18 This study defines the role of 3D printing in procuring standardized models for eliminating discrepancy and to achieve reliable results.
Endodontic periapical surgery
In a case report by Patel et al, a 53-year-old patient was referred for endodontic treatment of her maxillary left central incisor. A microsurgical approach was finalized, data from the diagnostic CBCT scan was used to make a physical model of the operative site, and CAD software was used to design a custom soft tissue retractor to be used during the patient's surgery. A custom retractor was fabricated with a 3D printer. During surgical procedure, the retractor enhanced visualization and soft tissue handling, improving the quality of treatment and, consequently, the prognosis.19
Clinical training
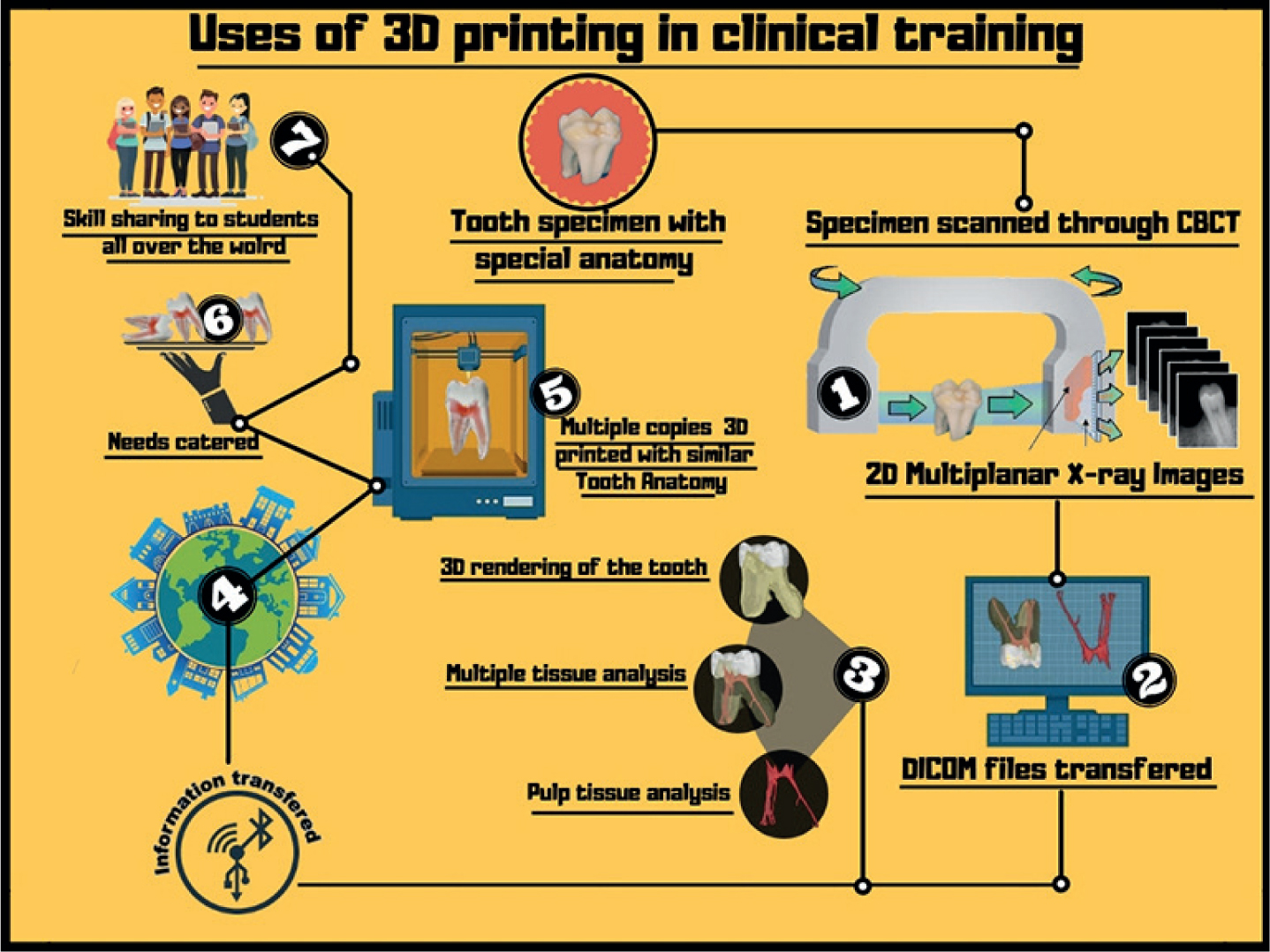
Robberecht et al tested a specific ceramic shaping technique (3D printing and slip casting of a root canal mould) to reproduce canal systems with the desired shape and complexity using a microporous hydroxyapatite (HAp)-based matrix. With this technique, it is possible to reproduce the radio-opacity of a tooth and variations in root canal morphology. The endodontic treatment simulation on those models confirmed that the models provided good tactile sensation during instrumentation and displayed suitable radiological behaviour. This novel anatomic root canal simulator is well suited for training undergraduate and postgraduate students in endodontic procedures (Figure 4).20
Figure 4. Infographic on uses of 3D in clinical training.
Guided endodontics
Zehnder et al performed endodontic treatment utilizing 3D printed templates to gain guided access to root canals and evaluated its accuracy in vitro.21 Deviations of planned and prepared access cavities were low, with means ranging from 0.16–0.21 mm at the base of the bur and 0.17–0.47 mm at the tip of the bur. Mean of angle deviation was 1.81°, with no significant difference between operators. They concluded that ‘Guided endodontics’ allowed an accurate and precise access cavity preparation up to the apical third of the root.21 Though groundbreaking, many authors still highlighted its limitation in posterior teeth root canal therapy until recently, when Shi et al used 3D printed guiding templates for successful conservative access into a mandibular molar with calcified canals.22 In future, 3D printing technology may become gold standard for the initiation of root canal therapy when concerned with access opening as it reduces the potential for iatrogenic errors, making it a dependable technology.
Application in regenerative dentistry
Pulp
Direct examples of pulp regeneration through 3D bioprinting, to the author's knowledge, is still lacking in the literature, but the fundamental building blocks of pulpal tissue have already been successfully fabricated using different printing methods. Biomimetic 3D printed functional blood capillaries have been reported recently.23,24,25 These networks are being populated by endothelial cells in a co-culture with other cell types and have demonstrated effective delivery of oxygen and nutrients, as well as waste removal from relatively large pre-osteoblast cell-laden hydrogels.24 Similarly, an interpenetrating hydrogel network of chemically cross-linked and physically entangled poly(2-hydroxyethyl methacrylate) hydrogel was 3D printed to guide the spread and proliferation of primary rat hippocampal neurons, hence forming differentiated, intricately branched, engineered neuron networks.26
These examples, combined with recent developments in spatially controlled extrusion printing of cell aggregates, represent a promising future for the 3D printing of pulp.
Whole-tooth regeneration
Recent developments in the field of whole-tooth regeneration27,28 have shed light on the potential of this technique for clinical applications. Early prototypes of 3D printed structures replicating the anatomy of the tooth and using composite inks of poly-e-caprolactone and hydroxyapatite have already been tested in vitro and in vivo.29,30 The controlled formation of cell aggregates in vitro, mimicking the epithelial mesenchymal interface that naturally occurs in the early stages of tooth formation, has been recognized as a fundamental step in whole-tooth regeneration.27,28,29,30 It has been hypothesized that architectural cues, such as size and positioning of cell aggregates, may be important determinants of the development and maturation of the tooth germ,31 as well as the positing and growth of cusps in the growing tooth.
Therefore, the quest for controlled on-demand formation of engineered teeth may greatly benefit from 3D printing technologies, where precise positioning of 3D cell aggregates is reproducibly achieved.
Challenges in building 3D vascularized organs
Proof-of-concept studies regarding bioprinting have been performed successfully, but the organs that have been produced are miniature and relatively simple.31,32,33 They are also often avascular, aneural, alymphatic, thin or hollow, and are nourished by the diffusion from host vasculature.31,32,33,34
However, when the thickness of the engineered tissue exceeds 150–200μm, it surpasses the limitation for oxygen diffusion between host and transplanted tissue.33 As a result, bioprinting complex 3D organs will require building precise multicellular structures with vascular network integration, which has not yet been done.34
Most organs needed for transplantation are thick and complex, such as the kidney, liver and heart.29 Cells in these large organ structures cannot maintain their metabolic functions without vascularization, which is normally provided by blood vessels.35 Therefore, functional vasculature must be bioprinted into fabricated organs to supply the cells with oxygen/gas exchange, nutrients, growth factors and waste-product removal, all of which are needed for maturation during perfusion.33,35
Although the conventional tissue engineering approach is not now capable of creating complex vascularized organs, bioprinting shows promise in resolving this critical limitation.33
The precise placement of multiple cell types is required to fabricate thick and complex organs, and for the simultaneous construction of the integrated vascular or microvascular system, that is critical for these organs to function.33
Regeneration using cell homing
Tooth regeneration by cell delivery encounters the above-mentioned translational hurdles. Kim et al conducted a study in which anatomically-shaped human molar scaffolds and rat incisor scaffolds were fabricated by 3D bioprinting from a hybrid of poly-ε-caprolactone and hydroxyapatite with 200-μm-diameter interconnecting microchannels. Stromal-derived factor-1 (SDF1) and bone morphogenetic protein-7 (BMP7) were delivered in scaffold microchannels. After 9 weeks, a putative periodontal ligament and new bone regenerated at the interface of the rat incisor scaffold with the native alveolar bone. Regeneration of tooth-like structures and periodontal integration by cell homing provide an alternative to cell delivery.29
Another study was conducted by Chiu et al where fabrication and characterization of mineral trioxide aggregate(MTA)/polycaprolactone 3D scaffold was done. They concluded that MTA 3D printed scaffolds exhibited good physical and chemical properties along with significant osteogenic differentiation ability, which lays down the cornerstone for the utility of 3D printing in bone/dental tissue engineering,36 which may accelerate its clinical applications due to its practicality and frugality.
Conclusion
3D printing is a technological revolution with a potential to transform the way we perceive dentistry. With advancements and innovations 3D printers have come a long way improvising their performance, resolution, availability and clinical applications. Research realm is continuously endeavouring to evolve and make additions to current inventory of dental applications of 3D printing technology. Existing advances that have been made so far in the field of dentistry are already significant and groundbreaking, but other revolutionary applications, such as pulp and tooth printing, will need time for fruition.