Innes NP, Frencken JE, Bjørndal L Managing carious lesions: consensus recommendations on terminology. Adv Dent Res. 2016; 28:49-57
Black GV A Work on Operative Dentistry Vol 1. Management of Children's Teeth.Chicago: Medico Dental Publishing Company; 1908
Kidd E. Should deciduous teeth be restored? Reflections of a cariologist. Dent Update. 2012; 39:159-166
Gruythuysen RJ. Non-restorative cavity treatment. Managing rather than masking caries activity (Dutch). Ned Tijdschr Tandheelkd. 2010; 117:173-180
Ekstrand KR, Christiansen ME. Outcomes of a non-operative caries treatment programme for children and adolescents. Caries Res. 2005; 39:455-467
Horst JA, Ellenikiotis H, Milgrom PL. UCSF protocol for caries arrest using silver diamine fluoride: rationale, indications and consent. J Calif Dent Assoc. 2016; 44:16-28
Gao SS, Zhang S, Mei ML, Lo EC, Chu CH. Caries remineralisation and arresting effect in children by professionally applied fluoride treatment – a systematic review. BMC Oral Health. 2016; 16
Contreras V, Toro MJ, Elías-Boneta AR, Encarnación-Burgos A. Effectiveness of silver diamine fluoride in caries prevention and arrest: a systematic literature review. Gen Dent. 2017; 65:22-29
Kay EJ, Vascott D, Hocking A, Nield H. Motivational interviewing in general dental practice: a review of the evidence. Br Dent J. 2016; 221:785-791
Keat RM, Fricain JC, Catros S The dentist's role in smoking cessation management – a literature review and recommendations: Part 2. Dent Update. 2018; 45:298-309
Stel G, Veerkamp JSJ, Amerongen WE van, Martens LC, Gemert-Schriks MCM van Treatment of (deep) caries lesions in primary teeth.Houten: Bohn Stafleu van Loghum; 2013
Ingers G, Cromvik U, Gleerup A, Rönnerman A. The effect on space conditions of unilateral grinding of carious proximal surfaces of primary molars – a longitudinal study. ASDC J Dent Child. 1982; 49:30-34
Mejàre I, Stenlund H, Julihn A, Larsson I, Permert L. Influence of approximal caries in primary molars on caries rate for the mesial surface of the first permanent molar in Swedish children from 6 to 12 years of age. Caries Res. 2001; 35:178-185
Bhatia SK, Maguire SA, Chadwick BL Characteristics of child dental neglect: a systematic review. J Dent. 2014; 42:229-239
Gruythuysen RJ, van Loveren C, Wiggelendam JM, Boven JA van, Burgersdijk RC. Neglect of oral care in children: a matter of integral approach. Ned Tijdschr Geneeskd. 2015; 159
Rotter JB. Social Learning and Clinical Psychology.New York: Prentice-Hall; 1954
Duijster D, de Jong-Lenters M, Verrips E, van Loveren C. Establishing oral health promoting behaviours in children – parents' views on barriers, facilitators and professional support: a qualitative study. BMC Oral Health. 2015; 15
van Loveren C, van Palenstein Helderman W. EAPD interim seminar and workshop in Brussels May 9 2015: Non-invasive caries treatment. Eur Arch Paediatr Dent. 2016; 17:33-44
Hansen NV, Nyvad B. Non-operative control of cavitated approximal caries lesions in primary molars: a prospective evaluation of cases. J Oral Rehabil. 2017; 44:537-544
Innes NP, Manton DJ. Minimum intervention children's dentistry – the starting point for a lifetime of oral health. Br Dent J. 2017; 223:205-213
Mijan M, de Amorim RG, Leal SC The 3.5-year survival rates of primary molars treated according to three treatment protocols: a controlled clinical trial. Clin Oral Investig. 2014; 8:1061-1069
Leal SC, Bronkhorst EM, Fan M, Frencken JE. Effect of different protocols for treating cavities in primary molars on the quality of life of children in Brazil – 1 year follow-up. Int Dent J. 2013; 63:329-335
Nainar SM. Is it ethical to withhold restorative dental care from a child with occlusoproximal caries lesions into dentin of primary molars?. Pediatr Dent. 2015; 37:329-331
Andropoulos DB, Greene MF. Anesthesia and developing brains – implications of the FDA warning. N Engl J Med. 2017; 376:905-907
Frachella J.United States: Personal communication; 2017
Santamaria RM, Innes NP, Machiulskiene V, Evans DJ, Alkilzy M, Splieth CH. Acceptability of different caries management methods for primary molars in a RCT. Int J Paediatr Dent. 2015; 25:9-17
Santamaria RM, Innes NPT, Machiulskiene V Alternative caries management options for primary molars: 2.5-year outcomes of a randomised clinical trial. Caries Res. 2017; 51:605-614
Nyvad B, Fejerskov O. Active root surface caries converted into inactive caries as a response to oral hygiene. Scand J Dent Res. 1986; 94:281-284
Schwendicke F, Krois J, Splieth CH, Innes N, Robertson M, Schmoeckel J, Santamaria RM. Cost-effectiveness of managing cavitated primary molar caries lesions: a randomized trial in Germany. J Dent. 2018; 78:40-45
Vermaire JH, van Loveren C, Brouwer WB, Krol M. Value for money: economic evaluation of two different caries prevention programmes compared with standard care in a randomized controlled trial. Caries Res. 2014; 48:244-253
van Strijp G, van Loveren C. No removal and inactivation of carious tissue: non-restorative cavity control. Monogr Oral Sci. 2018; 27:124-136
Non-restorative cavity treatment: should this be the treatment of choice? reflections of a teacher in paediatric dentistry René JM Gruythuysen Dental Update 2024 46:3, 707-709.
Authors
René JMGruythuysen
Retired Dentist, Post-academic Teacher Paediatric Dentistry, Tandzorg.nl, Rotterdam, The Netherlands
Non-Restorative Cavity Treatment (NRCT) is not favoured by many paediatric dentists. However, perhaps it should be the treatment of choice rather than confronting child and parents with a restorative, symptomatic, often less child-friendly approach. Does the child have a right to a viable biological treatment option, because solving a biological problem, basically caused by neglect, with technical solutions is ethically not defensible in all cases? Restorations simply mask the caries activity. What matters is the oral health and the well-being of the child. How can this best be served?
CPD/Clinical Relevance: This paper might serve as a discussion document for a group of oral health providers deciding practice policy with regard to the management of caries in primary teeth.
Article
Questioning the restorative approach
Some definitions and their corresponding acronyms start this section: Non-Restorative Cavity Treatment (NRCT) is a non-restorative method of controlling dentine lesions. It sits alongside Non-Operative Caries Treatment Programme (NOCTP), a method of controlling enamel lesions. Taken together, this non-restorative management of enamel and dentine lesions is called Non-Restorative Cavity Control (NRCC).1
NRCT manages cavitated caries lesions without placing fillings by making the lesions cleansable. This was first advocated for use in young children by GV Black in 1908.2 His non-restorative approach was based on his belief in plaque control to manage caries and his insistence that the most important thing in treating children was not to frighten them. In addition, in 1908 the filling materials available were amalgam and gold inlays, neither really suitable for use in primary teeth. The method is still relevant today because it is a biological, child-friendly approach to reduce, and preferably stop, the caries activity.
Some years ago Edwina Kidd questioned the traditional restorative approach to treating decayed deciduous teeth: ‘Whether deciduous teeth should be restored has caused controversy for at least 150 years and the argument rages on. Dental caries is a controllable process. The role of operative dentistry and restorations, as far as caries control is concerned, is to make cavitated, uncleansable lesions accessible to plaque control. However, deciduous teeth are exfoliated and perhaps non-operative treatments (plaque control, fluoride, diet) are all that are required to take cavitated teeth pain-free to exfoliation’.3
The present paper stresses the role of the parent/carer and the oral health team to NRCT, a technique which makes it possible for the carer to manage caries by plaque control rather than relying on fillings. The paper will start by describing the clinical aspects of NRCT, then the significance of supporting the carer will be addressed. It is this person who controls caries and effective communication between the oral health team and the carer is essential to the success of the technique. Subsequently, the attitude of both the oral health team and the carer to the technique will be considered. Do either consider that they can be in control of the oral health promoting outcome? At the end of the paper the results of clinical trials will be discussed.
Non-restorative cavity treatment
NRCT is indicated in young children with active, cavitated, caries lesions in the primary dentition and/or with dental anxiety. The emphasis of NRCT is to treat the causes of caries over time, decreasing discomfort for children and promoting oral health. Restoration of teeth is of secondary importance. NRCT requires some specific measures to manage cavitated caries lesions:4
Gain the informed consent of the carer. This role is critical to the technique and acceptance of this responsibility is essential to promote the oral health of the child;
Make cavities accessible for plaque removal using a slicing technique for approximal lesions. A contact should be kept in the cervical part of the tooth. Distal surfaces should be sliced rather flatter than mesial surfaces to facilitate the plaque removal (Figure 1a);
Carious dentine may be treated with anti-cariogenic agents (eg fluoride varnish, silver diamine fluoride) and/or a protective layer applied (eg glass ionomer cement) (Figure 1b);
Communicate with carers on their role in plaque control. This will certainly include twice daily brushing of the sliced area with fluoride-containing toothpaste;
Fix a suitable recall appointment to monitor the carer's brushing and review the caries activity of the lesion. The lesion should be seen to arrest over weeks and months (see: Monitoring caries activity). The monitoring system is basically the same as advocated by the performers of the non-operative caries treatment programme (NOCTP) for caries lesions in the enamel.5
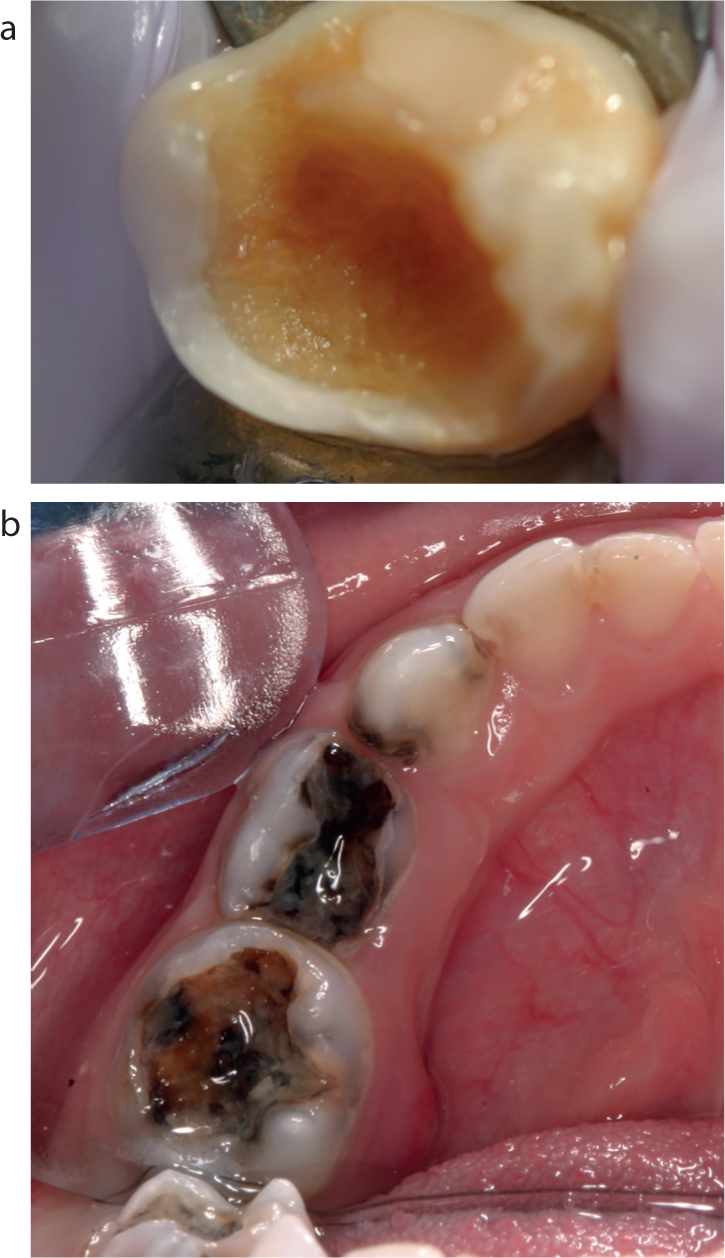
Figure 1.
(a) Slice technique: try to keep the contact in the cervical part and slice distal surfaces rather flatter than mesial surfaces to facilitate plaque removal. Arrest progression of the cavitated lesion by prolonged, vigorous brushing perpendicular to the dental arch. Courtesy of BSL, Springer Media, Houten, the Netherlands. (b) Bad, symptomatic approach on the right side (lingual abscess), after referring, followed by well-performed aetiological approach at the left side, combined with SDF application. Courtesy of Thierry Boulanger.
It is important to prevent pain and inflammation and adopt another (restorative) approach when continuing NRCT has not become in the interest of the child.
The use of silver diamine fluoride
Silver diamine fluoride (SDF) is a safe, effective treatment for dental caries across the age spectrum. SDF is indicated for the following patients:
Those with extreme caries risk;
Those who cannot tolerate conventional care;
Patients who must be stabilized so that they can be restored over time;
Patients who are medically compromised or too frail to be treated conventionally; and
A systematic review showed that SDF reduces the growth of cariogenic bacteria. It inhibits demineralization and promotes the remineralization of demineralized enamel and dentine. Moreover, it hampers degradation of the dentine collagen.7 In another systematic review it was concluded that, at concentrations of 30% and 38%, SDF shows potential as an alternative treatment for caries arrest in the primary dentition and permanent first molars.8 However, SDF should never be applied as an alternative to meticulous brushing plaque control (Figure 2a). It may assist lesion arrest, giving more time for the carer to perfect plaque control in cases of increased risks for pain/inflammation (Figure 2b).
Figure 2.
(a) The prescription ‘preformed crowns’ on the right side by a postdoc in paediatric dentistry was turned into NRCT, showing stabilized caries lesions on the right side without application of SDF after more than 2 years. Courtesy of BSL, Springer Media, Houten, the Netherlands. (b) Young child with hypersensitive carious teeth successfully treated by application of SDF, and parental help with cleaning, diet. Restorative treatment under general anaesthesia could be avoided. Courtesy of Thierry Boulanger and Ameera Paurobally.
Communication
Good communication is central to the technique. A proven tool is Motivational Interviewing which can be the starting point for the communication about the carers' wishes.9 What do they want, or not want, for their child? For many, this is not a new technique but it takes a lot of practice to become familiar with this approach or another ‘change model’.10 It may determine the level of oral care that parents or carers will provide and guide the recall interval that they are prepared to accept.
Although called an ’interview’, 90% of the time is spent listening to the client. It is not instruction, which is a one-sided communication. The professional should ask questions to gain insight to the motivation of the carer, rather than give unsolicited advice. Clinicians should be prepared to be disappointed by relapse but hide their disappointment! See if what is not happening can be turned to advantage. Clinical pictures to show progress, or lack of it, can be very useful here. Show, in neutral words, how these pictures can be interpreted and let carers draw their own conclusions about the caries activity.
Monitoring caries activity
Monitoring caries activity is the simplest way to determine caries risk. A child with lots of caries experience, where the caries activity is now at a standstill, needs rather less attention than a child who shows little caries experience, but where the caries activity has increased recently. In addition, it is important to know where in the dentition active caries lesions are located. Preventive actions should be focused on arresting the caries activity of these specific lesions. This is precisely what NRCT does. It is a biological solution to a biological problem. The difficulty comes when the carer considers a technical solution, such as a filling, has solved the biological problem.
However, monitoring caries lesions requires experience. There is not a clear demarcation in an individual lesion between activity and inactivity. This is a continuous scale and the clinician is deciding where on the scale this lesion is. For instance, dark dentine lesions are not always inactive and light dentine lesions are not always active (Figures 3a and b). Lesion texture is very useful. Determining the activity of a dentine lesion can be aided by probing with a blunt or a periodontal probe gently pressed onto the dentine (Figure 4). Photography aids monitoring, although it will not record texture, but it is useful for showing the changes in plaque accumulation and lesion colour. Comparing two sets of photographs will show the effect of the care.
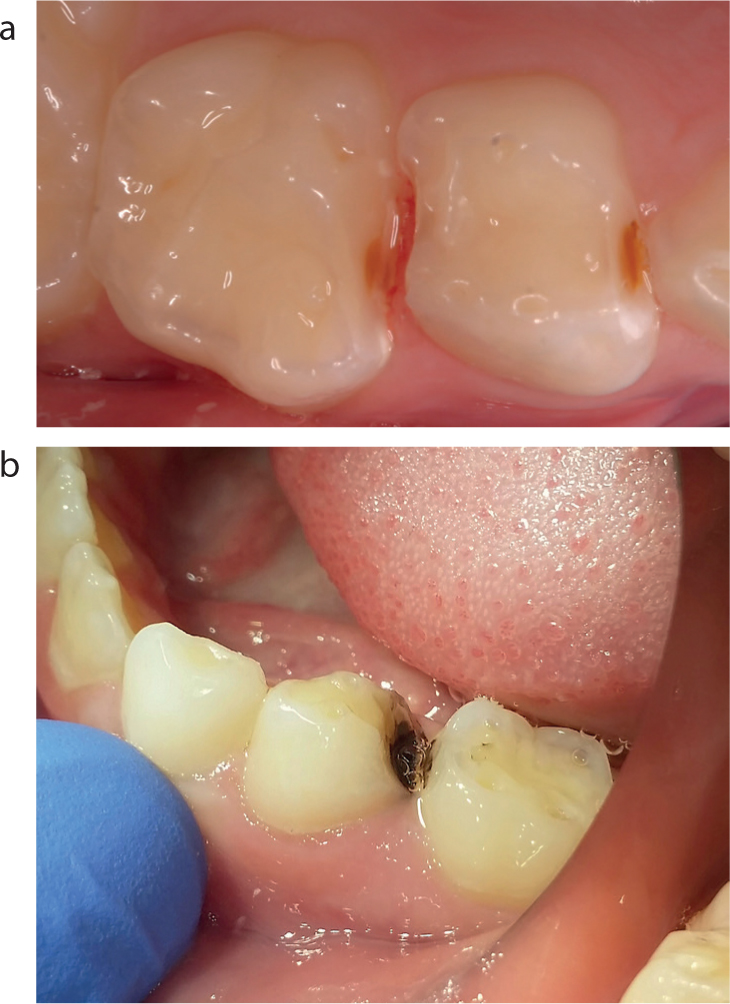
Figure 3.
(a) Light-coloured stabilized caries lesion with a hard texture after loss of a glass ionomer restoration. (b) Arrested lesion turned into a soft, caries active lesion after poor oral health care. Note visible plaque. Courtesy of BSL, Springer Media, Houten, the Netherlands.Figure 4. A blunt probe. Courtesy of BSL, Springer Media, Houten, the Netherlands.
Criticisms of NRCT
Non-restorative cavity treatment focuses on educating the carer in oral health care. The carer is put in charge of caries control. Despite this being essential, there is unease among some oral health providers. Here are some specific criticisms (among other things from a Dutch textbook of Paediatric Dentistry in 2013),11 together with suggestions that these worries may be unfounded: The criticisms are in italics.
Following slicing, space may be lost by mesial drift. Many years ago it was shown that providing the slicing is done correctly, this is not a problem.12
Following slicing, there is likely to be food impaction. Proper opening or slicing of the lesion can eliminate or minimize this (Figures 5a and b).
There may be lesion sensitivity after slicing. This can be managed by application of fluoride varnish or silver diamine fluoride.
Once a tooth is sliced, restoration is often no longer possible and extraction is the only remaining alternative. In practice this concern is usually unfounded. The technique opens up the undisturbed area for the biofilm and with carer cleaning, the caries process will slow down or arrest. If the oral health provider now wants to place a traditional restoration because of increased risk of pain/inflammation, an adhesive restoration usually solves the problem (Figures 6a–c). Sometimes capping the cusps is needed for additional retention and a Hall crown would be useful here when there is still enough space.
A restoration is preferable because it facilitates plaque removal. This frequently stated assumption must be questioned (Figure 7). If the distal surface of the second primary molar is carious, the mesial surface of the first permanent molar is 15 times more likely to become carious, whether or not a restoration is placed.13 Indeed, it could be argued that the non-restorative approach is preferable because it allows access to the mesial surface of the permanent tooth for cleaning, fluoride application and monitoring.
Figure 5.
(a) Sliced surfaces too vertical, promoting food impaction. Courtesy of BSL, Springer Media, Houten, the Netherlands. (b) Correct slice angle keeping cervical contact. Courtesy of Thierry Boulanger.Figure 6.
(a) NRCT failed due to incorrect slicing, inadequate carer guidance and lack of self-care. In an open conversation with the mother in the absence of the child, the mother drew the conclusion that oral care in the family had to get more priority. (b) Correction of the slicing did not lead to the desired result. It was decided to place restorations. (c) Bitewing radiograph almost 3 years after restoration. Primary teeth about to be shed. Meanwhile, the oral care in this family with three children had significantly improved. Courtesy of BSL, Springer Media, Houten, the Netherlands.Figure 7. Perfect restoration could not prevent the development of a new caries lesion after 2 years. Courtesy of BSL, Springer Media, Houten, the Netherlands.
Neglect of oral care
Neglect of a child's oral health can lead to pain, poor growth and impaired quality of life. In populations where there is a high prevalence of dental caries, the determination of which children are experiencing oral neglect is challenging.14 Inadequate oral care in children may be the result of ignorance, inability to deal with an unco-operative child or parental neglect. Of course, not following the advice of general health care providers to visit an oral health provider includes neglect of oral care too. Poor oral health care in a child may be a sign of more symptoms regarding child neglect.15
Based on a child neglect systematic review it was concluded that: ‘While it is indisputable that members of the dental team are well positioned to observe the signs of general and/or dental neglect, lack of clinical confidence in identifying and referring neglect prevails…….Given the known consequences of dental neglect, it is to be hoped that dental practitioners will be more pro-active in working with their local safeguarding team to ensure the safe and appropriate care of these children.’14 Please consider this conclusion in the light of the whole child rather than a purely teeth-centred approach. General health providers, including GPs, paediatricians and public health nurses, can all provide alerts regarding neglect of oral care. They can investigate whether the oral problems indicate wider problems of neglect in the child.15 It is recommended that general and oral health providers work together and make use of their respective expertise.
A contentious suggestion
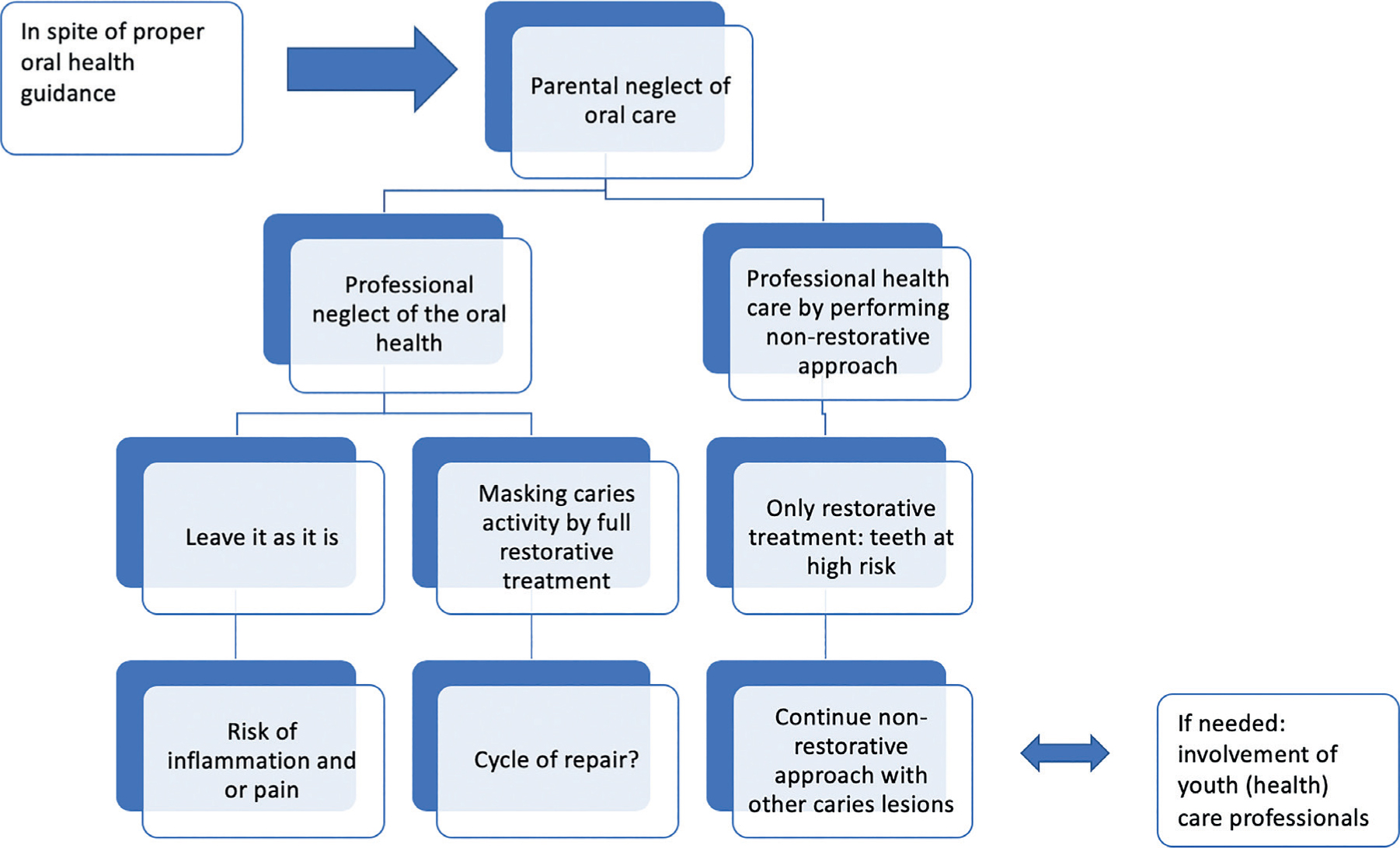
‘Restorative treatment of caries lesions in a child with neglected teeth masks the lack of oral health care’
This sentence may be a surprise and even considered insulting by some paediatric dentists! However, consider that a restoration is a technical solution to a biological problem and could mislead the parents with regard to the current state of the oral health. That's why, despite preventive instructions, fillings will often fail due to new caries (Figure 7). Non-restorative treatment methods, on the other hand, focus solely on stopping caries activity by plaque removal. These methods are all about guidance of oral health care and transferring responsibility to where it has to be, with the carer (Figure 8). This means motivating parents to re-brush their child's teeth every day. Failure is very obvious to the carer on recall because the sliced tooth shows an active caries lesion.
Figure 8. How to manage neglect of oral care?
Locus of control
This section contains a suggestion for consideration. The suggestion is unproven and contentious!:
Is an oral health provider's attitude to NRCT dependent on his/her locus of control?
Locus of control is the framework of Rotter's social-learning theory of personality.16 It is the extent to which people believe that they can influence the events in their lives. Is our locus of control internal or external? Our perception of where control lies can have an impact on our viewpoint and the way we interact with our environment. People who base their success on their own work and believe that they control their life have an internal locus of control. In contrast, people who attribute their success or failure to outside influences have an external locus of control.
There is currently interest in the locus of control in patients.17 Regarding caries prevention and the management of pre-cavitated caries lesions, it is stated that: ‘Non-invasive therapies can also be effective to arrest cavitated lesions but the success depends greatly on behavioural changes of patients to brush the lesions’.18 Patients' locus of control may be relevant to whether they make the necessary behavioural changes. Do they believe that they are in control and that their actions will make a difference? However, should the locus of control of the oral health provider also be considered? Might this also be relevant to the outcome and to whether the NRCT approach is chosen at all? And if ‘yes’, to what extent?
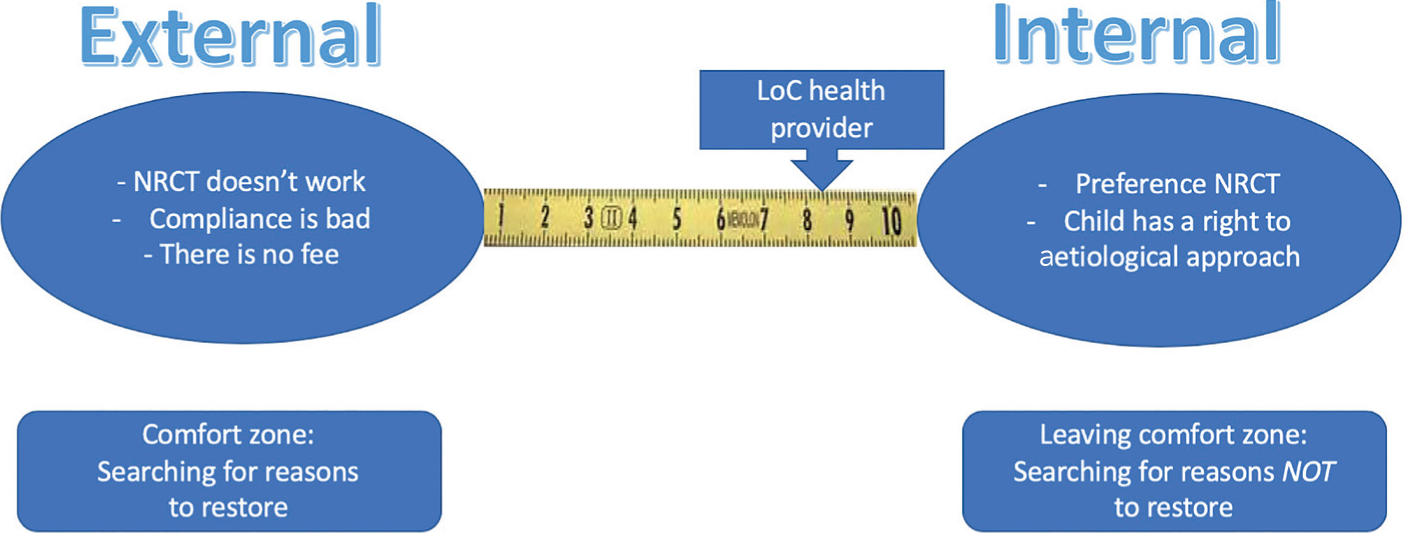
Some oral health providers think that they can improve the oral health of their patients. They have an internal locus of control with respect to the oral behaviour of their patients. Other oral health providers blame outside forces, such as bad co-operation of patients and public services, for the poor oral health behaviour of their patients. They have an external locus of control. Their attitude is: whatever they do is doomed to failure because of forces beyond their control (Figure 9). Could the unfounded criticisms of NRCT be a sign of an external locus of control?
Figure 9. Is this rule ‘locus of control oral health provider’ in the case of diagnosed caries activity/dental fear justified? (Sketch based on: Ned Tijdschr Tandheelkd 2018; 125: 38).
Non-restorative cavity treatment may stand or fall with the locus of control of the oral health provider (Figure 9). Could it be that oral health providers with an external locus of control focus on the weaknesses of non-restorative cavity treatment (see criticisms above) in order to avoid its application? Those with an internal locus of control may see the same criticisms as challenges to encourage improving the method. Hansen was the first researcher to show that self-reflection was relevant to at least 33% of the failures in a 9–44 months prospective clinical evaluation of NRCT.19 Unfortunately, there are no data of the locus of control of the oral health provider. We only know that restoration of cavities is rather more popular than promoting prevention by the non-restorative approach in paediatric dentistry. Some want to move from the traditional ‘drill and fill’ towards a more ‘child friendly’ approach, highlighting sealants and sealing in demineralized dentine.20 Interestingly, these rather more symptomatic than biological concepts still involve the oral health professional providing a technical solution. When can we expect the huge step forward to a biological (= plaque removal) approach in paediatric dentistry?
Clinical trials of non-restorative approaches
Mijan et al carried out a clinical study in which, in an experimental group (UltraConservative Treatment), small cavities were restored with glass ionomer cement using an atraumatic restorative technique, while medium/large cavities were left unrestored but cleaned daily with toothpaste/toothbrush under supervision.21 Conventional restorative protocols were used in control groups. After three and a half years the clinical results were similar in experimental and control groups. Another part of this study showed that well performed, non-restorative treatment is associated with a preservation of the Quality of Life. In other words, all treatment protocols were effective in reducing children's experience of pain, their sleeping problems and their irritability and/or frustration levels over the 1-year period.22
Despite the clinical evidence of efficacy for the non-restorative approach to dentine lesions, in the eyes of some paediatric dentists NRCT is a controversial treatment concept. In a short communication about the acceptability of NRCT, it was discussed whether it is ethical to apply NRCT to children with approximal cavities in the temporary teeth.23 The author suggested that NRCT can be viewed as dental neglect because it prevents a restorative treatment that would predictably deliver freedom from pain and infection. The author forgets that NRCT is not designed only to treat the symptoms but, in the first place, aims to improve the oral health of the child.
Following the Hippocratic tradition of doing no harm, NRCT seeks to avoid unnecessary invasive treatments. If these are performed under general anaesthesia, they pose risks in young children.24 John Frachella, a paediatric dentist in the United States, claims that he has decreased treatment under general anaesthesia by 90% by applying SDF (Figure 2b).25 Preventing pain and inflammation and adequate monitoring, are essential parts of the NRCT treatment concept.4
A systematic review on the effectiveness of preformed steel crowns (Hall crowns) in the treatment of carious temporary molars with high caries active children includes a ‘single tooth’ randomized controlled trial on NRCT, compomer restorations (CR) and Hall crowns (HT).26 Twenty teeth were recorded as having at least one minor failure: NRCT, n = 8 (5%); CR, n = 11 (7%); HT, n = 1 (1%). The Hall crown performed best and the comparison between NRCT and CR showed no significant difference. Nine (6%) experienced at least one major failure: NRCT, n = 4 (2%); CR, n = 5 (3%); HT, n = 0 (0%). Individual comparison of NRCT and CR showed no statistically significant difference in major failures. The authors concluded that the study's preliminary results (1 year) were at risk of bias but, after the experiment, 89% of the oral health providers continued to prefer a restorative covering.27
Perhaps the locus of control of these oral health providers remained external and presumably these preferences will have influenced the results. Since no grinding/slicing protocol was published, the reader has no way of knowing whether the slicing was carried out correctly.
The 2.5 year results of this study showed, for cumulative survival rates: HT = 92.5%, NRCT = 70.5% and CR = 67.2% (p = 0.012).28 NRCT and CR outcomes were comparable. HT performed better than NRCT and CR for all outcomes. In the study, 69% of children in the NRCT armed with treatment failures failed to attend the 3-month recalls regularly. Still, the results were comparable with making fillings. So, one could discuss possible improvement of the results by introducing stricter protocols (including youth care – Figure 8) for recall and by using the option to slow down the caries activity with SDF.
Moreover, single tooth studies are not designed to test the aetiological approach because they do not take into account the oral health benefits for the child of these treatments.
Many Cochrane reviews are critical of the methodology of the studies available. Randomized clinical trials, favoured by Cochrane reviews, are designed for testing a simple hypothesis. It is interesting to speculate whether NRCT protocols can ever be properly evaluated in these research methods. This is partly because the NRCT concept involves both a technical element (slicing), but the behavioural content is critical to success or failure. Can patients and oral health providers be matched in these behavioural elements to produce unbiased experimental and control groups? In other words, what is the risk of bias due to validity problems? This will be another contentious point!
Nevertheless, it has been known for over 30 years that caries activity in dentine lesions can be arrested.29 What might be needed is further qualitative research with a series of well-documented case reports (successful and failed cases) so that the results of NRCT in practice for the individual child and oral health provider can be evaluated.
Final observations
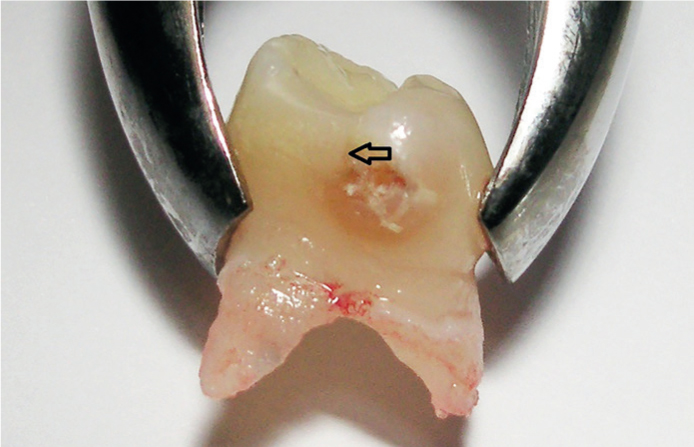
A recent cost-effectiveness analysis on an existing randomized clinical trial compared the relative costs and clinical outcomes of three different approaches, Hall crowns (HT), non-restorative cavity control (NRCC, without the promising use of SDF), and conventional compomer restorations (CR).30 The treatments were applied to a single tooth in each child. Hall crowns were less costly than the other two interventions, surviving longer and requiring fewer interventions. Cost studies are needed. This cost analysis is quite restricted (single tooth) and the subject deserves further study in new, larger trials specifically designed to evaluate cost more realistically. The unit of activity will need to be the child not a single tooth. This will mimic the clinical situation where a child will present with several carious teeth. It will be very important to design trials so that there is long term evaluation of oral health, such as the caries status of erupting first molars (Figure 10). The NRCC (with SDF, if needed!) approach might be ultimately more beneficial, and therefore cheaper, because oral health has been promoted through behavioural change and fewer lesions subsequently develop. There is already some indication that behavioural change can decrease caries activity and decrease costs. When non-operative caries treatment and prevention were compared with traditional treatment, the non-operative programme was preferred after 3 years.31
Figure 10. Superficial caries lesion mesially on the left first permanent upper molar could be stabilized by NRCT done to the primary molar. Courtesy of BSL, Springer Media, Houten, the Netherlands.
NRCC has been advocated, particularly in primary dentitions, for families able to accept responsibility for the disease and commit to remedial action, including diet modification and regular, frequent toothbrushing with a fluoride toothpaste.32 However, the approach seems particularly suitable for families where co-operation is not currently forthcoming. Of all approaches, this one stresses behaviour change as the basis for successful treatment. Dutch guidelines, based on five years of experience, suggest that NRCT is explicitly indicated in young children with active caries lesions and children with dental anxiety where restorative treatments are not accepted.11 This applies to caries lesions in the enamel (NOCTP) or in the dentine (NRCT). The aim is to promote the self-care of caries-active children in order to arrest the caries process. After more than ten years of Dutch experience there is no reason to change this guideline. That's why, in the eyes of the author, non-restorative caries control should be the treatment of choice for children before shedding primary teeth.