Schneider DL, Steiner R, Romaine J. Human cargo: health conditions of Chinese migrants interdicted offshore by US authorities. J Community Health. 2003; 28:19-39
Ehmsen BK, Biswas D, Jensen NK, Krasnik A, Norredam M. Undocumented migrants have diverse health problems. Dan Med J. 2014; 61
Riggs E, Gussy M, Gibbs L, van Gemert C, Waters E, Priest N, Watt R, Renzaho AM, Kilpatrick N. Assessing the cultural competence of oral health research conducted with migrant children. Community Dent Oral Epidemiol. 2014; 42:43-52
Riggs E, Gussy M, Gibbs L, van Gemert C, Waters E, Kilpatrick N. Hard to reach communities or hard to access services? Migrant mothers' experiences of dental services. Aust Dent J. 2014; 59:201-207
Jaeger FN, Hossain M, Kiss L, Zimmerman C. The health of migrant children in Switzerland. Int J Public Health. 2012; 57:659-671
Aichberger MC, Bromand Z, Rapp MA, Yesil R, Montesinos AH, Temur-Erman S, Heinz A, Schouler-Ocak M. Perceived ethnic discrimination, acculturation, and psychological distress in women of Turkish origin in Germany. Soc Psychiatry Psychiatr Epidemiol. 2015;
Maneze D, Salamonson Y, Poudel C, DiGiacomo M, Everett B, Davidson PM. Health-seeking behaviors of Filipino migrants in Australia: the influence of persisting acculturative stress and depression. J Immigr Minor Health. 2015;
Meredith LS, Eisenman DP, Green BL, Kaltman S, Wong EC, Han B, Cassells A, Tobin JN. Design of the violence and stress assessment (ViStA) study: a randomized controlled trial of care management for PTSD among predominantly Latino patients in safety net health centers. Contemp Clin Trials. 2014; 38:163-172
Schwendicke F, Dörfer CE, Schlattmann P, Page LF, Thomson WM, Paris S. Socioeconomic inequality and caries: a systematic review and meta-analysis. J Dent Res. 2015; 94:10-18
Mulligan R, Seirawan H, Faust S, Barzaga C. Dental caries in underprivileged children of Los Angeles. J Health Care Poor Underserved. 2011; 22:648-662
Julihn A, Ekbom A, Modéer T. Migration background: a risk factor for caries development during adolescence. Eur J Oral Sci. 2010; 118:618-625
Dorn T, Ceelen M, Tang MJ, Browne JL, de Keijzer KJ, Buster MC, Das K. Health care seeking among detained undocumented migrants: a cross-sectional study. BMC Public Health. 2011; 11
O'Leary MC, Sarwar M, Hutchinson SJ, Weir A, Schofield J, McLeod A, Cameron S, McTaggart C, Banday S, Foster GR, Ahmed S, Fox R, Mills PR, Goldberg DJ, Anderson E. The prevalence of hepatitis C virus among people of South Asian origin in Glasgow – results from a community based survey and laboratory surveillance. Travel Med Infect Dis. 2013; 11:301-309
Padovese V, Egidi AM, Melillo TF, Farrugia B, Carabot P, Didero D, Costanzo G, Mirisola C. Prevalence of latent tuberculosis, syphilis, hepatitis B and C among asylum seekers in Malta. J Public Health (Oxf). 2014; 36:22-27
Kuehne A, Fiebig L, Jansen K, Koschollek C, Santos-Hövener C. [Migration and infectious disease surveillance in Germany: Analyses of Tuberculosis, HIV and Syphilis surveillance data]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2015; 58:560-568
Donaldson CD, Jack RH, Møller H, Lüchtenborg M. Oral cavity, pharyngeal and salivary gland cancer: disparities in ethnicity-specific incidence among the London population. Oral Oncol. 2012; 48:799-802
Pearson N, Croucher R, Marcenes W, O'Farrell M. Prevalence of oral lesions among a sample of Bangladeshi medical users aged 40 years and over living in Tower Hamlets, UK. Int Dent J. 2001; 51:30-34
Raphaely NR, O'Moore EOM.London: Health Protection Agency and Department of Health; 2010
Williams R. Health and length of residence among South Asians in Glasgow: a study controlling for age. J Public Health Medicine. 1993; 15:52-60
Hawkins SS, Lamb K, Cole TJ, Law C. Influence of moving to the UK on maternal health behaviours: prospective cohort study. Br Med J. 2008; 336:1052-1055
Zhang W. Oral health service needs and barriers for Chinese migrants in the Wellington area. N Z Dent J. 2008; 104:78-83
Zhang W. Chinese culture and dental behaviour: some observations from Wellington. N Z Dent J. 2009; 105:22-27
Kolasa K. I won't cook turnip greens if you won't cook kielbasa: food behavior or Polonia and its health implications. In: Bauwens E (ed). St. Louis: Mosby; 1978
Scheper-Hughes N. Difference and danger: the cultural dynamics of childhood stigma, rejection, and rescue. Cleft Palate J. 1990; 27:301-307
Population movements, whether voluntary or forced, are an integral part of an increasingly globalized society and, while the health needs of migrant populations cannot be generalized, some migrants can have worse oral health outcomes compared with their host-country counterparts, with their first dental contact typically being for emergency care. Failure to provide immediately necessary treatment may be unlawful under the Human Rights Act 1998.
CPD/Clinical Relevance: NHS dental services need to evolve and address the challenges inherent in caring for vulnerable migrants. Education and appropriate training needs to be developed for the dental profession in order to enable new ways of promoting inter-sectoral care and community engagement.
Article
Jasmine Murphy Crispian Scully
The volume of population movements, whether voluntary or forced, is an integral part of an increasingly globalized society. Migrant populations are composed of several overlapping groups, including long-term and short-term immigrants, migrant and seasonal workers, refugees, asylum seekers, international students and others – such as victims of human trafficking.
A large proportion of the migrant population tends to move through legal channels and their migration does not necessarily have negative health impacts, but some may experience difficulty in accessing appropriate healthcare. For other migrant population groups, the migration process itself may have negative health implications, in particular among the vulnerable migrant subgroups such as trafficked and smuggled people, asylum seekers, refugees and those with humanitarian protection and their families, children and undocumented migrants. Therefore, the health needs of the migrant populations cannot be generalized but the importance of culturally sensitive oral healthcare, that has been recognized for well over a decade, needs to be seriously considered in this context.1
The net long-term international migration to the UK in the year to March 2015 was 330,000 – up 94,000 from the previous year and the highest net migration on record. These figures include an estimated 183,000 EU citizens, 196,000 non-EU citizens and 53,000 people from Romania and Bulgaria (EU2). There were 290,000 people who immigrated for work and 188,000 people immigrated for study. In 2015, asylum applicants (excluding dependents) numbered 25,771. This is an increase of 10% compared with the previous year. However, the number of applications remain low relative to the peak number of applications in 2002 at 84,132.2
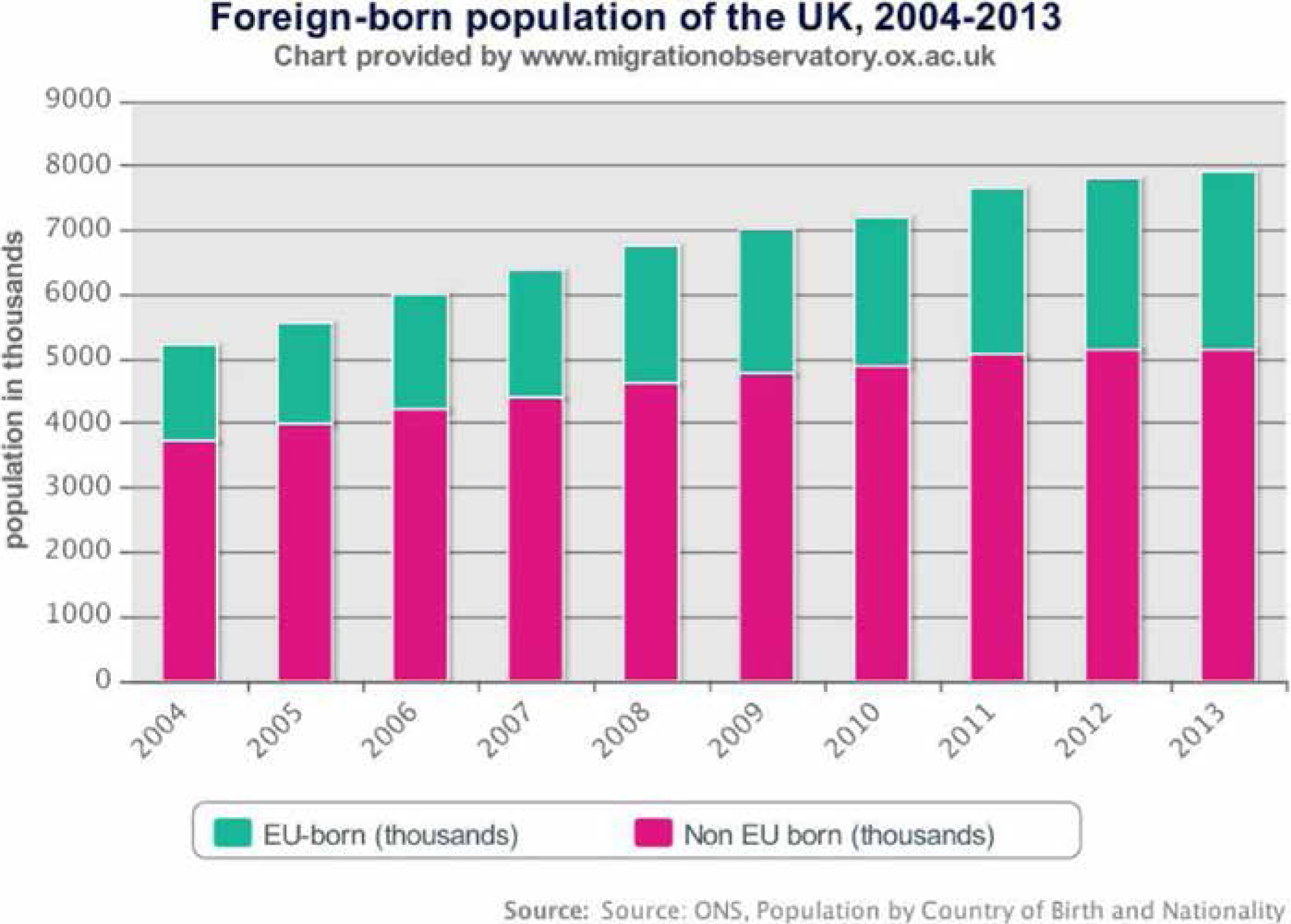
Further, the number of UK residents in 2014 who were born abroad has increased steadily over time (Figure 1). However, it should be noted that the prevalence of migration in the UK is by no means unprecedented by European standards.3
Figure 1. Foreign born population of the UK (2004–2013).
Migrants' rights to accessing NHS dental services
The new NHS Immigration Health Surcharge for temporary migrants, students and their dependents came into effect from April 2015.4 This surcharge ensures that temporary, non-EEA (European Economic Area) migrants coming to the UK for more than six months contribute to the NHS in a manner in line with their immigration status. The surcharge, which is collected by the Home Office, is not a visa fee and goes directly into the NHS and provides migrants with access to the NHS on the same terms as a permanent UK resident, ie they will receive NHS care generally free of charge but may be charged for the services that a permanent UK resident would also pay for, such as NHS dental treatment and prescription charges in England.
Those visiting the UK temporarily (ie less than six months) are exempt from paying the health surcharge and are expected to pay for any NHS healthcare they receive at the point of use.5 However, it should be noted that they are only entitled to receive any treatment that is immediately necessary or urgent on the NHS and it is left to clinicians to determine whether treatment is immediately necessary, urgent or non-urgent. Furthermore, failure to provide immediately necessary treatment may be unlawful under the Human Rights Act 1998, even if payment has not been received in advance.6
It should also be pointed out that healthcare is a devolved matter and therefore different charging exemptions apply in Wales, Scotland and Northern Ireland, although the Immigration Health Charge still applies to migrants who are intending to reside in those parts of the UK. Furthermore, people covered by EU Regulations are entitled to ‘all medically necessary treatment’ for the duration of their visit, which includes dental treatment.7
NHS treatment is not considered a ‘public fund’ for immigration purposes, so migrants subject to the ‘No Recourse To Public Funds’ (NRPF) condition are not prohibited from accessing NHS dental services.8 However, migrants with NRPF in receipt of local authority support will not receive free NHS dental care unless they fall into one of the exempt categories (ie 60 years or over, under 16 years, age 16–18 years and in full-time education, pregnant or have had a baby in the previous 12 months and have a valid maternity exemption certificate). They may, however, be entitled to full or partial help through the NHS Low Income Scheme.9
In summary, NHS dental care can be accessed by all, regardless of immigration status but there are thresholds in terms of coverage entitlement. There is a concern that this not only causes confusion with regards to entitlement, but will also have an uneven impact across migrants whose circumstances often do not fall into neat categories. This could potentially lead to migrants with complex immigration histories being unfairly refused access to NHS dental care due to a lack of knowledge and understanding of regulations regarding entitlements by the dental profession and also vulnerable migrant groups.
Vulnerable migrants
There is no definition of what constitutes a vulnerable migrant entering the UK. The current available literature focuses primarily on asylum seekers and refugees. However, there are other groups which will also be particularly vulnerable, eg those refused asylum, EU and other overseas migrant workers, trafficked people and undocumented migrants. Within these vulnerable groups, there is also likely to be a wide spectrum of vulnerability. The vulnerability of any group differs according to its exposure to a given problem and its capacity to tackle it. Groups with greater vulnerability that gain immediate entitlement to the full range of NHS dental care may include:
Asylum seekers;
Migrants who have been trafficked;
Refugees;
Victims of domestic violence.
However, there are also other migrant groups within the context of greater vulnerability but with only limited entitlements to NHS dental care and/or poor access to public funds and resources, including:
Failed asylum seekers;
Rough sleeping migrants (Eastern, Central and Southern European), their position being compounded by weak welfare protection;
Undocumented migrants (mainly people who have entered the country illegally and not via the asylum seeking or visa processes) are largely invisible in official records and have few if any entitlements to services, including NHS dental care;
Furthermore, some new migrants not listed in the groups above who have not yet engaged with NHS dental care may also be vulnerable (in terms of oral health), as they may have been marginalized and subjects of recognized oral health inequalities in their country of origin. Thus, vulnerability is shaped by many factors and addressing migrant oral health needs is a challenge, both because of the heterogeneity of the migrant population and because of restrictions imposed by legislation on access to NHS dental care.
Oral health of migrants
There are many reports on prevalent health issues related to migrants.10 The Survey of New Refugees in the UK11 reported that refugees had poorer health than the general population in England and Scotland, with those described as being in good health being more likely to be employed than other refugees. Poor health was also associated with slow improvement in English language skills over time. There may also be cultural issues affecting access to healthcare that need to be considered.12
A significant amount of oral health research affecting migrants and recipient communities has been reported from Australia, Europe and the United States of America (USA), with migrant children having worse oral health outcomes compared with their host-country counterparts (Table 1). Additionally, the first dental contact for migrant mothers and their children has been typically for emergency care.13,14,15 There can also be a considerable burden of infectious diseases in certain migrant groups which may impact on oral health and/or healthcare, eg HIV, HBV, HCV (Table 1).
Public health concern around the oral health behaviour and lifestyles of migrants relates not merely to the impact on oral health; for instance reported high smoking rates among migrants from Eastern European countries,28 but also to changes over time in the receiving/host community.29 Particular lifestyle areas of interest pertinent to oral health include smoking patterns, alcohol consumption, diet and breast-feeding. The adoption of norms, values and behaviour prevalent in the receiving/host community can also have longer term negative consequences for health outcomes, eg higher levels of smoking (especially in pregnancy), lower levels of breast-feeding and diets with high fat/sugar content, rates of diabetes, cardio-vascular disease and cancer.30,31
Issue
Comments
References
Stress
From discrimination or violence
Aichberger MC et al16; Maneze D et al17; Meredith LS et al18
Viral infections (eg human immunodeficiency viruses [HIV], hepatitis B virus [HBV] and/or hepatitis C virus [HCV]).Varies significantly by geographic region and reflects global epidemiologic patterns, Some are seen particularly in migrant men who have sex with men (MSM)
Malignant disease (oral and oropharyngeal cancers)
Particularly in people from South Asia (including Bangladesh, Sri Lanka, India, Pakistan, Taiwan); Latin America (Brazil, Uruguay, Puerto Rico and Cuba); and Papua New Guinea, and other Pacific islands in Melanesia. Also in East Asia, and Eastern Europe. Lifestyle habits are important
However, evidence on lifestyle factors affecting oral health status, as well as oral health behaviour, and access to NHS dental care by migrant groups in the UK, is poorly documented. It would be expected that there will be variations in health among different migrant categories, but the absence of data makes it difficult to understand these patterns.
Barriers to dental care and oral health
There is some evidence relating to barriers to healthcare among migrants in the UK, although this is largely from small scale, local and qualitative studies. The UK studies have not reported specifically on access to NHS dental care, but migrants can face significant barriers in accessing dental services, mainly due to lack of knowledge, legislation, inadequate information (particularly for new migrants unfamiliar with healthcare systems in the UK), accessibility, cost, insufficient support in interpreting and translating for people with limited English fluency, lack of access to reliable transport due to poverty, cultural beliefs and practices, long waiting lists, poor services in areas of deprivation where many recent migrants might live, confusion around entitlement to some types of services, particularly among migrants with insecure immigration status, as well as among service providers and cultural insensitivity of some front-line healthcare providers.13,14,22,32,33
Different migrant population groups may differ in the way they think about oral health and in how they define an oral health problem, determine its seriousness, and decide whether and when to seek dental care. For one migrant group, a painful tooth may be enough to motivate care-seeking, but in another, bleeding, swelling or fever may be necessary before dental care is sought. Similarly, the importance of prevention and self-care can also be culturally influenced. For some groups, traditional child-rearing practices can also be detrimental to oral health.34,35
Some of these barriers, such as information, language and transport, appear to cut across length of residence, affecting longer established migrants as well.3 Furthermore, some migrants may choose not to seek dental care due to their chaotic lives, which makes it difficult for them to prioritize oral health; or they may disregard oral health as a form of self-harm or neglect.
Reducing oral health inequalities
As part of the UK government's commitment to reducing oral health inequalities, policy has focused largely on improving access to NHS dental services and in improving oral health outcomes. Very little emphasis has been placed on the specific needs of migrants and, as a result, there is hardly any evidence on oral health outcomes, needs and barriers to NHS dental services for migrants as part of national datasets. This limits the strategic planning, service design and equalities monitoring which are essential to good commissioning practice. As the migrant population is likely to increase over the next decade, the incidence and prevalence of oral diseases common to their country of origin is likely to affect the epidemiology of their host country.
Migration can be associated with poor health outcomes for marginalized and socially disadvantaged populations. The ethnic origin of a patient may unfairly affect access to care and ultimately oral health outcomes. NHS England currently has the responsibility to commission responsive and appropriate NHS dental services for the population in England, while Local Authorities are responsible for the delivery and/or provision of dental public health services in order to improve oral health and reduce oral health inequalities of their local resident population. Migration can therefore pose a challenge to the commissioning, delivery and provision of effective and culturally sensitive NHS dental and oral health promotion services.
The Equality Act 2010 requires public bodies and others carrying out public functions to consider the needs of all individuals in shaping policy, delivering services and also in relation to their own employees.36 Migrants' fundamental oral health needs may not be adequately met, thus raising concerns with regard to equity, social cohesion and inclusiveness. While equal access to NHS dental services is important, so too are oral health promotion and prevention measures, which are often overlooked when considering the health of migrants.
Policy considerations
A public health approach is necessary in order to align strategies, policy options and interventions for improving oral health outcomes for the population and also in avoiding disparities in oral health status and access to NHS dental services between migrants and the host population. Therefore, it is imperative that when the Joint Strategic Needs Assessment (JSNA) is assessing the oral health needs of the local resident population, that consideration is also given to including information on the local migrant population. However, owing to the diversity, invisibility and mobility of the migrant population, this presents a challenge as there is no routinely captured data that can be reported. Furthermore, the health needs of migrant communities are not static and may change quickly. However, these challenges could be addressed by gaining insight and intelligence through partnership working with migrant service users and also the voluntary care sector which may be providing services for this population group. It is also acknowledged that investing time and effort in engaging with specific communities that have previously had limited contact/relationship is challenging, but it may ultimately serve to impact more on health inequalities.
A Joint Strategic Assets Assessment (JSAA) identifies local assets which can help to protect health and wellbeing and improve outcomes and may contribute to reducing oral health inequalities. A mapping exercise should be undertaken in order to map migrant community organizations and local community-based service provision to allow for the building of networks with particularly marginalized communities.
Community engagement/development is about building active and sustainable communities based on social justice, mutual respect, participation, equality, learning and co-operation.37 It involves changing power structures to remove the barriers that prevent people from participating in the issues that affect their lives. Local community development programmes should be sustainably funded and equipped to provide support, expertise and contacts to enable active engagement with migrant communities which will promote social inclusion and independence whilst gathering information about needs and experiences and building capacity.
For any new migrant arrival, the shifting landscape of service provision and governance may create confusion when attempting to navigate statutory structures. Systems and processes should be in place to welcome new arrivals, also providing accurate and appropriate information on accessing NHS healthcare (including NHS dental services), language support and advocacy services, as well as (oral) health promotion services.
Clinical inexperience in interacting with such population groups, compounded by possible incorrect beliefs held by the clinician about the behaviour or health of specific migrant population groups, may contribute to a cultural dissonance and lack of trust between the dental profession and the migrant group. Cultural competence is intimately related to health literacy. Oral health literacy is ‘the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate oral health decisions’.38 Importantly, effective communication is dependent on both the oral health literacy of patients, as well as the skills, preferences and expectations of the dental clinician.39 There should therefore be a proactive approach taken in building capacity within the dental profession in understanding culturally sensitive issues associated with migrants' oral health, and therefore education and training should be considered for the local dental community in understanding oral health aspects associated with population movements.
A local review of the current NHS dental service provision and the extent to which the services meet the current and anticipated future needs of the local migrant population should be undertaken. However, in order to do so, routine and consistent collection of data pertaining to ethnicity and the identification of migrants, along with outcomes data, is fundamental. Ethnicity data collected by dental providers can provide proxy information on the local migrant population. However, ethnicity categories rarely reflect the heterogeneity of the migrant population. Providers should be contracted to collect data on country of origin, nationality or preferred language, which may give a better indication of migration status. Once such data is available, analysis of migrant experiences can be undertaken when mapping current services, which would enable an understanding of the accessibility and effectiveness of existing services in addressing the needs of vulnerable migrants. Referrals and pathways could also be audited in order to ensure that vulnerable migrants are receiving an equivalent service to that of the local/host population, and to identify any inappropriate or ineffective practice or behaviour, either from the migrant population or the dental profession. Alternative pathways for referrals should also be considered to include midwives and health visitors, befriending schemes, health advocate programmes, other community groups and service user support groups.
Equality impact assessments should also be undertaken when reviewing and/or making changes to the delivery of NHS dental services to ensure that they are inclusive for migrants. Such compliance with the Equality Duty will help commissioners meet equality objectives through the design of a commissioning strategy that is inclusive and equalities-focused.36 There should also be improved equalities monitoring of the workforce to increase the diversity of staff to reflect the migrant and BME (black and minority ethnic) population that they serve.
Conclusions
There should be strategic planning taking into account key oral health issues affecting the migrant population, including those affecting the wider determinants of health relating to education, housing, employment, child poverty, health inequalities and community cohesion:
The Joint Strategic Needs Assessment (JSNA) should include the oral health needs of the local migrant population when assessing the oral health needs of the local resident population;
Equality impact assessments should be undertaken when reviewing and/or changing service provision;
Improved data recording is fundamental in order to allow the oral health status and access to dental care of the various subgroups of migrants to be analysed;
NHS dental services need to evolve and address the challenges inherent in caring for vulnerable migrants. As migrants continue to originate from around the globe, and as migrants begin to move to smaller cities and towns, appropriate training needs to be developed for the dental profession in order to enable new ways of promoting inter-sectoral care and community engagement.