Littlewood SJ, Kandasamy S, Huang G. Retention and relapse in clinical practice. Aust Dent J. 2017; 62:51-57
de Bernabe PG, Montiel-Company JM, Paredes-Gallardo V Orthodontic treatment stability predictors: a retrospective longitudinal study. Angle Orthod. 2017; 87:223-229
Freitas KMS, Guirro WJG, de Freitas DS, de Freitas MR, Janson G. Relapse of anterior crowding 3 and 33 years postretention. Am J Orthod Dentofacial Orthop. 2017; 152:798-810
Sinclair PM, Little RM. Maturation of untreated normal occlusions. Am J Orthod. 1983; 83:114-123
Behrents RG, Harris EF, Vaden JL, Williams RA, Kemp DH. Relapse of orthodontic treatment results: growth as an etiologic factor. J Charles H Tweed Int Found. 1989; 17:65-80
Meade MJ, Millett D. Retention protocols and use of vacuum-formed retainers among specialist orthodontists. J Orthod. 2013; 40:318-325
Meade MJ, Dreyer CW. A survey of retention and retainer practices of orthodontists in Australia. Aust Orthod J. 2019; 35:174-183
Dogramaci EJ, Rossi-Fedele G. The quality of information on the Internet on orthodontic retainer wear: a cross-sectional study. J Orthod. 2016; 43:47-58
Singh P, Grammati S, Kirschen R. Orthodontic retention patterns in the United Kingdom. J Orthod. 2009; 36:115-121
Salehi P, Heidari S, Tanideh N, Torkan S. Effect of low-level laser irradiation on the rate and short-term stability of rotational tooth movement in dogs. Am J Orthod. 2015; 147:578-586
Hirate Y, Yamaguchi M, Kasai K. Effects of relaxin on relapse and periodontal tissue remodeling after experimental tooth movement in rats. Connective Tissue Res. 2012; 53:207-219
Hawley CA. A removable retainer. Int J Orthod Oral Surg. 1919; 5:291-305
Sheridan JJ, LeDoux W, McMinn R. Essix retainers: fabrication and supervision for permanent retention. J Clin Orthod. 1993; 27:37-45
Al-Moghrabi D, Salazar FC, Pandis N, Fleming PS. Compliance with removable orthodontic appliances and adjuncts: a systematic review and meta-analysis. Am J Orthod Dentofacial Orthop. 2017; 152:17-32
Al-Moghrabi D, Pandis N, Fleming PS. The effects of fixed and removable orthodontic retainers: a systematic review. Prog Orthod. 2016; 17
Pratt MC, Kluemper GT, Lindstrom AF. Patient compliance with orthodontic retainers in the postretention phase. Am J Orthod Dentofacial Orthop. 2011; 140:196-201
Al-Moghrabi D, Johal A, O'Rourke N Effects of fixed vs removable orthodontic retainers on stability and periodontal health: 4-year follow-up of a randomized controlled trial. Am J Orthod Dentofacial Orthop. 2018; 154:167-174
Lai C, Grossen J, Renkema A-M, Bronkhorst E, Fudalej P, Katsaros C. Orthodontic retention procedures in Switzerland. Swiss Dent J. 2013; 124:655-661
Padmos JA, Fudalej PS, Renkema AM. Epidemiologic study of orthodontic retention procedures. Am J Orthod Dentofacial Orthop. 2018; 153:496-504
Habegger M, Renkema AM, Bronkhorst E, Fudalej PS, Katsaros C. A survey of general dentists regarding orthodontic retention procedures. Eur J Orthod. 2017; 39:69-75
Kotecha S, Gale S, Khamashta-Ledezma L A multicentre audit of GDPs knowledge of orthodontic retention. Br Dent J. 2015; 218:649-653
Bearn DR. Bonded orthodontic retainers: a review. Am J Orthod Dentofacial Orthop. 1995; 108:207-213
Green JIJ. Dental materials: the multi-stranded wire retainer. BDJ Team. 2015; 1
Abudiak H, Shelton A, Spencer RJ, Burns L, Littlewood SJ. A complication with orthodontic fixed retainers: a case report. Ortho Update. 2011; 4:112-117
Little RM. Clinical implications of the University of Washington post-retention studies. J Clin Orthod. 2009; 43:645-651
Patel A, Sandler J. First aid for orthodontic retainers. Dent Update. 2010; 37:627-630
Zachrisson BU. Multistranded wire bonded retainers: from start to success. Am J Orthod Dentofacial Orthop. 2015; 148:724-727
Rinchuse DJ, Miles PG, Sheridan JJ. Orthodontic retention and stability: a clinical perspective. J Clin Orthod. 2007; 41:125-132
Johnston C, Littlewood S. Retention in orthodontics. Br Dent J. 2015; 218:119-122
Kucera J, Marek I. Unexpected complications associated with lower fixed retainers. Am J Orthod Dentofacial Orthop. 2016; 149:202-211
Lee KD, Mills CM. Bond failure rates for V-loop vs straight wire lingual retainers. Am J Orthod Dentofacial Orthop. 2009; 135:502-506
Rose E, Frucht S, Jonas IE. Clinical comparison of a multistranded wire and a direct-bonded polyethylene ribbon-reinforced resin composite used for lingual retention. Quintessence Int. 2002; 33:579-583
Bolla E, Cozzani M, Doldo T, Fontana M. Failure evaluation after a 6-year retention period: a comparison between glass fiber-reinforced and multistranded bonded retainers. Int Orthod. 2012; 10:16-28
Salehi P, Zarif Najafi H, Roeinpeikar SM. Comparison of survival time between two types of orthodontic fixed retainer: a prospective randomized clinical trial. Prog Orthod. 2013; 14
Foek DL, Ozcan M, Krebs E, Sandham A. Adhesive properties of bonded orthodontic retainers to enamel: stainless steel wire vs fiber-reinforced composites. J Adhes Dent. 2009; 11:381-390
Lodha S, Kumar S, Mehta S. Technique tips – Active lingual retainer. Dent Update. 2014; 41
Kravitz ND, Grauer D, Schumacher P, Jo YM. Memotain: a CAD/CAM nickel-titanium lingual retainer. Am J Orthod Dentofacial Orthop. 2017; 151:812-815
Moskowitz EM, Park MB, Maestre ME. Direct bonding of Ortho Flextech lingual retainers. J Clin Orthod. 2004; 38:554-556
Pandis N, Fleming PS, Kloukos D, Polychronopoulou A, Katsaros C, Eliades T. Survival of bonded lingual retainers with chemical or photo polymerization over a 2-year period: a single-center, randomized controlled clinical trial. Am J Orthod Dentofacial Orthop. 2013; 144:169-175
Gange P. The evolution of bonding in orthodontics. Am J Orthod Dentofacial Orthop. 2015; 147:S56-S63
Artun J, Spadafora AT, Shapiro PA. A 3-year follow-up study of various types of orthodontic canine-to-canine retainers. Eur J Orthod. 1997; 19:501-509
Waring DT, Cappelli R. The Manchester positioner – dual retention made easy. J Orthod. 2009; 36:111-114
Egli F, Bovali E, Kiliaridis S, Cornelis MA. Indirect vs direct bonding of lower fixed retainers in orthodontic patients: comparison of retainer failures and posttreatment stability. A 2-year follow-up of a single-center randomized controlled trial. Am J Orthod Dentofacial Orthop. 2017; 151:15-27
Andrén A, Asplund J, Azarmidohkt E, Svensson R, Varde P, Mohlin B. A clinical evaluation of long term retention with bonded retainers made from multi-strand wires. Swed Dent J. 1998; 22:123-131
Conway M, Littlewood SJ, Hodge TM, Nelson-Moon Z. Bonded retainers placed under rubber dam: an exploratory RCT. J Orthod. 2011; 38
Feilzer AJ, Laeijendecker R, Kleverlaan CJ, van Schendel P, Muris J. Facial eczema because of orthodontic fixed retainer wires. Contact Derm. 2008; 59:118-120
Littlewood SJ, Millett DT, Doubleday B, Bearn DR, Worthington HV. Retention procedures for stabilising tooth position after treatment with orthodontic braces. Cochrane Database Syst Rev. 2016;
Edman Tynelius G, Bondemark L, Lilja-Karlander E. A randomized controlled trial of three orthodontic retention methods in Class I four premolar extraction cases – stability after 2 years in retention. Orthod Craniofac Res. 2013; 16:105-115
O'Rourke N, Albeedh H, Sharma P, Johal A. Effectiveness of bonded and vacuum-formed retainers: a prospective randomized controlled clinical trial. Am J Orthod Dentofacial Orthop. 2016; 150:406-415
Forde K, Storey M, Littlewood SJ, Scott P, Luther F, Kang J. Bonded versus vacuum-formed retainers: a randomized controlled trial. Part 1: stability, retainer survival, and patient satisfaction outcomes after 12 months. Eur J Orthod. 2018; 40:387-398
Edman Tynelius G, Petrén S, Bondemark L, Lilja-Karlander E. Five-year postretention outcomes of three retention methods – a randomized controlled trial. Eur J Orthod. 2014; 37:345-353
Krämer A, Sjöström M, Hallman M, Feldmann I. Vacuum-formed retainer versus bonded retainer for dental stabilization in the mandible – a randomized controlled trial. Part I: retentive capacity 6 and 18 months after orthodontic treatment. Eur J Orthod. 2019; https://doi.org/10.1093/ejo/cjz072
Storey M, Forde K, Littlewood SJ, Scott P, Luther F, Kang J. Bonded versus vacuum-formed retainers: a randomized controlled trial. Part 2: periodontal health outcomes after 12 months. Eur J Orthod. 2018; 40:399-408
Meade MJ, Weston A, Dreyer CW. Valid consent and orthodontic treatment. Aust Orthod J. 2019; 35:35-45
Alkadhimi A, Sharif M. Orthodontic retention: a clinical guide for the GDP. Dent Update. 2019; 46:848-860
Professor of Orthodontics/Consultant, Orthodontic Unit, Cork University Dental School and Hospital, University College Cork, Wilton, Cork, Republic of Ireland
Indefinite retention is now considered essential to prevent relapse after orthodontic treatment. Compliance with removable retainer wear is suboptimal and appears to decline with time post-treatment. As a result, use of bonded retainers may become more commonplace in the future. In this narrative review, the characteristics of bonded retainers are outlined and a summary of the evidence from randomized clinical trials regarding their effectiveness is provided. Guidance is also offered regarding care and maintenance.
CPD/Clinical Relevance: All general dental practitioners (GDPs) should be familiar with types of bonded retainers, evidence relating to their effectiveness and the GDP's role regarding their care and maintenance.
Article
Maurice J Meade
Relapse is the return, following orthodontic correction, of the features of the original malocclusion.1 Retention is the phase, following active orthodontic treatment, that attempts to maintain teeth in their corrected positions.2 Relapse is variable and unpredictable, with lower anterior segment alignment and overbite appearing to be the least stable orthodontically-corrected occlusal features.2,3,4
Facial growth continues throughout life and this may lead to unwanted and variable occlusal changes, such as the development of lower incisor imbrication. These changes are ‘normal’ physiological changes and occur in both orthodontically-treated and untreated individuals.3,5,6 Retention procedures, therefore, may be considered necessary to minimize the occlusal effects of these age changes, as well as to maintain the results of orthodontic correction.
There appears to be agreement among orthodontists in national surveys that indefinite retention is necessary and that guidance regarding orthodontic retention practices requires development.7,8,9,10 Although investigations have explored the use of biomedical agents, low light laser and vibrational therapies in an attempt to prevent relapse, the principal method of retention involves the use of an orthodontic retainer.11,12 Retainers are either removable, most commonly the vacuum-formed retainer (VFR) and the Hawley retainer, or fixed as a lingual/palatal or rarely labial bonded retainer (BR).13,14
Compliance with removable retainer wear appears to reduce as time from removal of fixed appliances increases.15,16,17 Use of BRs appears to be increasing.18 They are the preferred retainer type, either on their own or in combination with removable retainers (‘dual’ or ‘hybrid’ retention’),4 among specialist orthodontists in several countries, including Norway and the Netherlands.8,19,20 Recent studies, however, have indicated that knowledge related to BRs may be lacking among GDPs and that GDPs would welcome further training and education in this regard.21,22
The aims of this narrative review are to:
Outline the characteristics of lingually or palatally placed BRs;
Review the evidence regarding the effectiveness of types of BRs;
Provide guidance to GDPs on the care and maintenance of BRs.
Characteristics of BRs
In relation to the characteristics of BRs, the following will be considered:
Development, advantages and disadvantages;
Material types and design;
Bonding adhesive;
Bonding protocol;
Failure and unintended effects.
Development, advantages and disadvantages
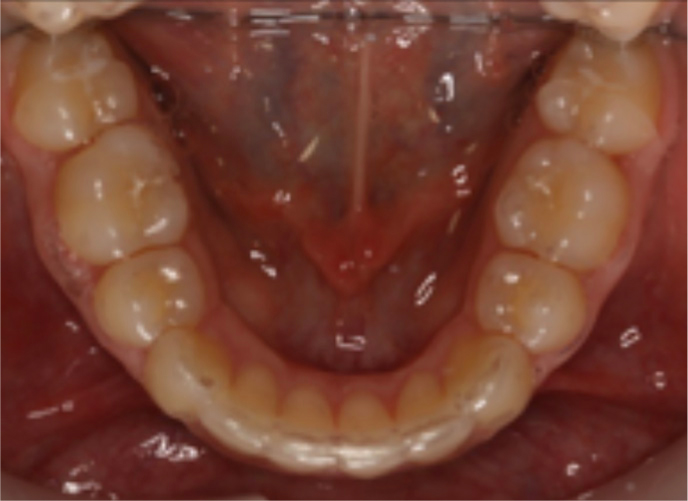
Bonded retainers were first described in the early 1970s, which was more than 50 years after the Hawley retainer and 20 years before the VFR (Figures 1–3).13,14,23 Proposed advantages and disadvantages of BRs are shown in Table 1.2,23,24,25,26,27,28
Figure 1. Lower Vacuum Formed Retainer.Figure 2. Upper Hawley retainer.Figure 3. Lower BR (0.01” x0.028” braided rectangular SS) bonded to both canines and all incisors.
Advantages
Disadvantages
Aesthetics
Technique sensitive during placement
Wear not dependant on patient compliance
Difficulty bonding to artificial substrates such as porcelain
Patient and social acceptability
Unwanted tooth movement if active at placement or ‘activated’ during wear
Superior settling compared to a Hawley retainer or VFR
Bond failure or retainer breakage
Difficulty with maintenance of optimal oral hygiene
Occlusal interference
Indications for a BR include those listed in Table 2.4,23,24,25,26,27,28 It is accepted, however, that BRs alone may not be appropriate for some post-treatment situations, such as maintenance of an expanded upper or lower arch.7,10,28
Pre-treatment Features
Post-treatment Features
Median diastema
Space closure following lower incisor extraction
Generalized anterior spacing
Proclination of lower incisors
Severe rotations
Increase in intercanine width
Impacted canines and incisors
Residual overjet in the absence of lower lip support
Severely displaced teeth
Minimal or no overbite after incisor crossbite correction
Severe incisor crowding
Deep overbite correction
Loss of periodontal support
Correction of anterior open bite by orthodontic means
Cleft lip and palate
Teeth with no opposing tooth contact
Material types and designs of BRs
Lingually or palatally placed BRs typically comprise one of several material types and are held in place by a bonding adhesive.29
Stainless steel wire
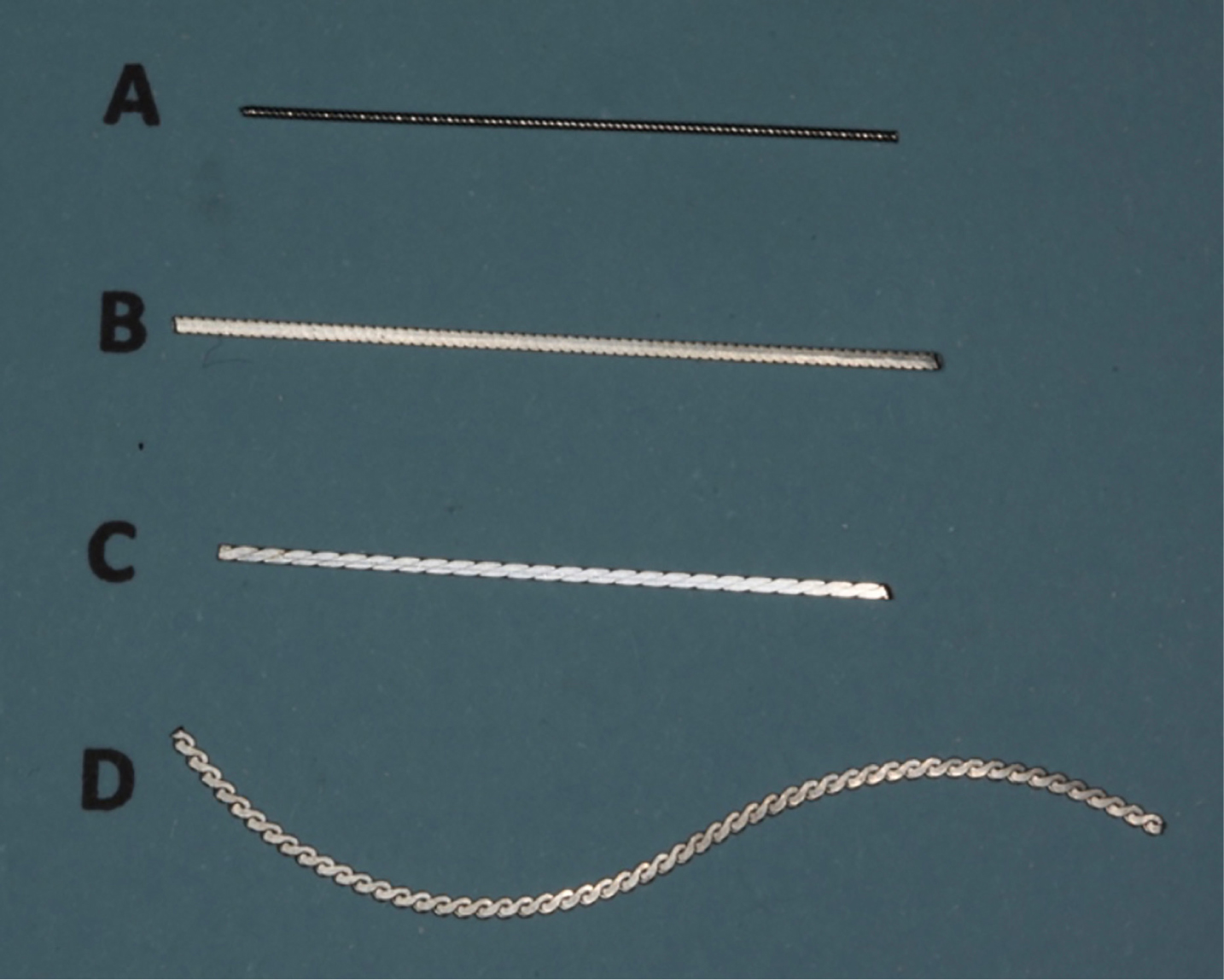
Multistrand stainless steel (SS) appears to be the most commonly used wire type for BRs.24,29Figure 4 shows a range of SS wires used for BR fabrication. These may be bonded to the ‘end teeth’ only of those requiring retention, usually the canines (sometimes called ‘canine-to-canine’), or more commonly are bonded to the palatal/lingual surfaces of all the teeth in the labial segments.23 Zachrisson suggests only extending the BR from lateral incisor to lateral incisor in the upper arch in children and adolescents, as failure rates are higher when canines are included.29 SS wires for BRs may be round or rectangular in cross-section and are usually formed from 3–6 fine strands of wire that are either braided or arranged co-axially.23,28,29 The flexibility of the wire facilitates physiological movement of the teeth, even when several adjacent teeth are bonded. Common diameter sizes range from 0.0175” to 0.0215”.29
Figure 4. A range of SS wires used for BR fabrication. (a) ‘Penta One Coaxial’: 0.0215” (Ortho Organizers, Carlsbad, California). (b) ‘Flattened multistrand’: 0.01” x 0.03”’ (Sheboygan, Wisconsin). (c) ‘Braided Retainer Wire’: 0.01” x 0.028” (Ortho Technology, Lutz, Florida). (d) ‘Ortho-Flextech®’: 0.016” x 0.038” (Reliance Orthodontic Products, Itasca, Illinois).
Plain SS wire tends to have a greater diameter (usually 0.025” to 0.032”) and is consequently more rigid. It is a common choice of wire for ‘canine-to-canine’ retainers (Figure 5).29 This thicker wire may reduce the risk of wire fracture but the lack of flexibility may make it more prone to failure.29 A thicker upper BR wire may also provide a ‘biteplane’ effect and help maintain correction of a deep overbite.30 The ‘canine-to-canine’ design may be indicated when there is alteration of the antero-posterior or lateral position of the lower labial segment during treatment and maintenance of the post-treatment intercanine width is essential.25,29,30 It is potentially easier to place and more hygienic than a BR attached to all six anterior teeth.31 It is also ‘fail safe’; the patient is immediately aware if attachment to one or both canine teeth fails.32 It may, however, be less effective at maintaining incisor alignment.30
Figure 5. Lower ‘canine-to-canine’ BR (0.032” round SS bonded to canines only).
Gold-coated, multi-stranded and round wires have been developed and are claimed to be more aesthetic.29 A ‘V-loop’ design involving 0.0195” multistrand SS has also been described with the potential advantage of facilitating easier oral hygiene.33
Fibre-reinforced retainer
Fibre-reinforced retainers were introduced as an aesthetic alternative to SS wires (Figure 6).34,35,36 They include glass fibre-reinforced and plasma-treated polyethylene woven ribbons (often 500–1000 fibres or ribbons) that can be adapted to the lingual surfaces of the teeth and bonded using composite resin (CR). When CR is added, the retainer becomes more rigid and helps to splint the teeth together.
Figure 6. Ribbond® fibre-reinforced BR. (Reproduced with the kind permission of Dr Dave Rudo).
These retainers are translucent, easy to shape and can be cured at the same time as the bonding adhesive. They may be suitable for patients with nickel allergy as they contain no nickel. Their reduced ‘bulk’ and ease of repair are additional potential advantages. The increased rigidity of this retainer type, however, may run the risk of greater likelihood of failure during masticatory function.37
Nickel titanium wire
A 0.018” Nickel-titanium (NiTi) wire bonded lingually to each tooth from canine-to-canine has been used to correct relapse of lower anterior crowding and then left in place as a passive retainer.38
CAD/CAM Nickel titanium retainer
A new CAD/CAM retainer (Memotain®; Ormco CA Digital) made of 0.014” x 0.014” rectangular nickel-titanium, custom cut from nickel-titanium sheets and electropolished, is precisely contoured to the patient's tooth anatomy (Figure 7). Proposed advantages include more precise bonding without occlusal interference or microbial colonization.39
Figure 7. CAD/CAM Memotain™: (a) upper and (b) lower retainer. (Reproduced with the kind permission of Ormco CA Digital).
Another type of retainer which uses CAD/CAM is SureSmile® (OraMetrix, Richardson, Tx 75082). A robot hand bends the copper-nickel-titanium with plastic deformation created on application of a blast of intense heat during the bending process.39
LingLockTM retainer
The alumino-ceramic LingLockTM retainer consists of pairs of retention elements each with interlocking components.40 Retention is gained by the close contact of the parts while allowing access for interdental floss. Additional proposed advantages are improved aesthetics, reduced laboratory and chairside time, reduced risk of fracture and ‘easy repair’.
Ortho Flextech® retainer
This is a type of ‘flexible chain’ (Ortho Flextech®, Reliance Orthodontic Products, Itasca, Illinois) fabricated from white gold, copper, zinc, silver and nickel and its adaptability makes it potentially easier for operators to place (Figure 4d).41
Bonding adhesive
Composite resin is most commonly used for bonding a lingual, palatal or labial retainer to enamel.23 Macro-filled, hybrid, micro-filled and nano-filled composites have all been described. There appears to be no difference in failure rates of retainers bonded with light-cured composite or chemically-cured composite.42 Alternative bonding adhesives may be required for artificial tooth substrates.43
Bonding protocol
Two main techniques have been described:
Direct technique;
Indirect technique.
Direct technique
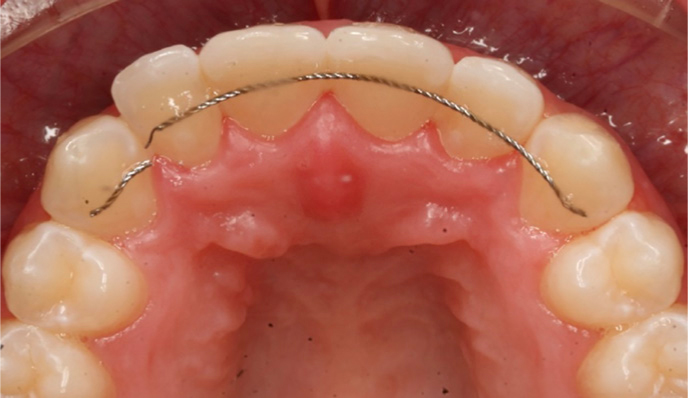
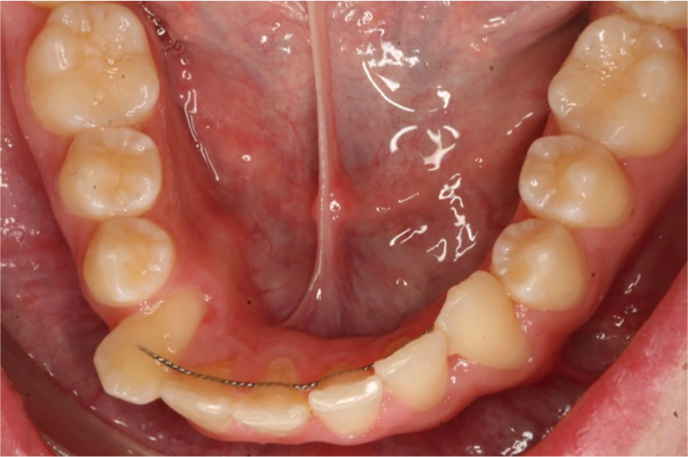
This involves placement of the BR without the need for an intermediate (laboratory) step. The wire must be ‘shaped’ or fabricated to conform to the morphology of the surfaces of the teeth on which the BR is to be placed. It must be correctly positioned and kept passive to ensure optimal bonding and prevent inadvertent activation.23,44 Dental floss, orthodontic elastics and SS ligatures have been used to assist in maintenance of correct position during placement (Figure 8).25
Figure 8. Dental floss used to maintain correct position of BR (0.010” x 0.028” braided SS) during direct bonding.
Indirect technique
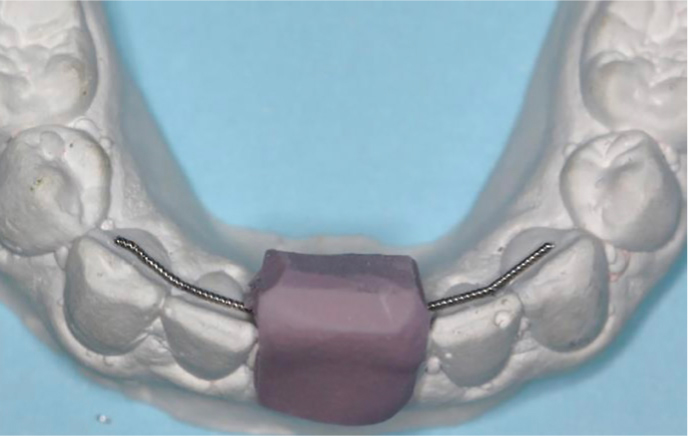
The indirect technique involves fabrication of the BR on a cast of the patient's dentition, typically recorded shortly prior to the completion of treatment. The BR is then transferred to the mouth via, for example, a silicone putty or an acrylic positioning matrix (Figure 9).45 Potential advantages of the indirect technique include more accurate positioning of the BR as well as minimal disturbance during bonding.25 Additional time for preparation of the BR and the extra laboratory costs may be potential disadvantages.46
Figure 9. Silicone putty and BR (0.0215” five-stranded SS) prior to direct bonding.
Failure and unintended effects
Bonded retainers may fail in the following ways:
At the wire-composite interface;
At the adhesive-enamel interface;
Stress fracture of wire.
At the wire-composite interface
Bond failure, with the detachment of the retainer from the CR, is often due to mechanical/masticatory forces and may explain reported increased failure rates of upper BRs. Sufficient CR must be used. A thickness of 1 mm covering a bonding surface area of 3.5 mm per tooth has been suggested.25 A more heavily filled CR may be helpful in resisting occlusal forces on upper BRs.30 Cutting a groove in the palatal surfaces of the upper anterior teeth, in which the BR can be bonded, has been suggested as a way of minimizing occlusal interference.47
At the adhesive-enamel interface
To ensure optimal enamel adhesion, a dry field is essential. Rubber dam use has been proposed to minimize the risk of moisture contamination during BR placement but its use did not reduce bond failure rates.48 The enamel surface requires thorough cleaning, with some advocating sandblasting.43
Stress fracture of wire
This may be associated with wire fatigue or be due to excessive bite force. Breakage may occur in thinner wires, whereas thicker wires may ‘detach’ rather than break due to their increased rigidity (Figure 10).
Figure 10. BR breakage (0.016” x 0.016” braided SS) with unwanted movement of permanent upper right lateral incisor and canine.
Unintended effects
Care in placement is advised as a BR may be unintentionally activated and cause side-effects such as minor tooth rotations, bone fenestration and excessive displacement of teeth.32 It may also become inadvertently activated if the wire becomes distorted during function (Figure 11).
Figure 11. Displacement of permanent lower right canine and incisors due to inadvertent activation of BR (0.016” x 0.016” braided SS). (Reproduced with the kind permission of Dr Melinda Barva).
An unusual complication, facial eczema, has also been reported following placement of a nickel containing BR but there were no oral symptoms.49
Evidence in relation to BR effectiveness
Presently, evidence only exists for certain types of BR, principally SS wires bonded to all teeth in the upper and/or lower labial segments, but the wire size has differed between studies.16
Currently, there is no evidence regarding the effectiveness of a CAD/CAM nickel titanium retainer, LingLock™ retainer or OrthoFlextech® retainer, although a trial is ongoing comparing a CAD/CAM nitinol and a chairside bonded retainer (OrthoFlextech®) BR.50
While systematic reviews have concluded that there is a lack of evidence on which to base retention practices16,51 this narrative review focuses on evidence from prospective RCTs involving BRs regarding:
Effectiveness in maintenance of post-treatment alignment and occlusal stability;
Effects on oral health;
Survival and failure rate;
Patient and practitioner satisfaction;
Cost-effectiveness.
Effectiveness in maintenance of post-treatment alignment and occlusal stability
Measurement of post-treatment alignment has been most commonly undertaken using Little's Irregularity Index (LII). This is the sum of the distances between the contact points of the teeth in the upper and lower labial segments, ie from ‘canine to canine’. Other measures of stability include intercanine width, intermolar width, extraction space reopening, arch length, overjet and overbite.
Table 3 shows the mean and/or median changes in LII reported for BRs compared to VFRs, pre-fabricated positioners and interproximal reduction (IPR).18,54,55,56,57
Study Characteristics
Intervention
LII (mm)
McDermott et al56 2013N: 85Mean age: Unreported.Outcome: 2 years after debond
Lower VFRavsLower BR (0.018” multistrand SS wire bonded to incisors and canines)
*statistically significant. a: wear VFR full-time except for eating and oral hygiene. b: wear VFR 22 to 24 hours per day for first 2 days, then night only for 12 months and alternate nights for next 12 months. c: VFR full-time basis for 6 months, nights only for next 6 months, alternate nights for next 6 months, one or two nights wear weekly. d: VFR wear every night. e: VFR full-time for 1 week, followed by every night for the first 12 months and then reducing in frequency until 1-2 nights per week from 24 months after ‘debond’.
Statistically significant differences were noted between retainers in LII in the lower arch in four of the studies.18,54,55,56 A statistically significant difference was observed in one study for the LII in the upper arch between all groups compared.55 The upper intercanine width also changed significantly in the latter study.55 The mean/median LII change in the lower arch associated with BRs ranged from 0.45 mm to 2.1 mm, whereas the mean/median range related to VFRs was 1.3 mm to 2.37 mm.18,55,56,57 The LII change was greatest with the prefabricated positioner (3.4 mm).55 The evidence suggests that BRs were marginally more effective than VFRs or prefabricated positioners in maintaining lower incisor alignment.
Effects on oral health
Three studies have incorporated an assessment of gingival and periodontal health in relation to BRs. A BR appears inferior to a VFR for gingival and periodontal health at 12-month57,58 and 48-month review.18,58,59 Greater levels of plaque, gingival inflammation and calculus were found with a BR compared to a VFR.
Studies reporting the survival rates of BRs versus RRs are given in Table 4. Those reporting survival and/or failure rates of a variety of BR types are given in Table 5.
Evidence is conflicting regarding failure rate/breakage for BR compared to VFR in the lower arch in the first 12 months after orthodontic treatment,54,59 but no differences in these outcomes have been observed between these retainers in the upper arch.54,60
Polyethylene ribbon retainers and multistrand SS retainers appear to perform similarly (Table 5).
Patient and practitioner satisfaction
Bonded retainers were significantly ‘more acceptable to wear’ than VFRs but took much longer to fit.60
No statistically significant differences were found at 12 months between patients' opinions of wearing BRs or VFRs compared to fixed appliances. Both types of retainer were perceived to be better, or at least no worse, than fixed appliances, with no difference in embarrassment except for two subjects allocated VFRs. Speech was affected less with BRs than with VFRs but the latter were easier to clean.59
Cost-effectiveness
Indirect bonding of a BR in the mandible was significantly faster,41 taking a mean time of 321 (SD: 31) seconds compared to a mean time of 401 (SD: 40) seconds for direct placement.41 This, however, may not result in significant cost saving as there was no difference in BR failure rates placed using either technique.41
Discussion and guidance on care and maintenance of BRs
In this narrative review, the characteristics of BRs have been outlined and the evidence from RCTs summarized in relation to their effectiveness. Retainer choice and retention protocol must be based on patient, treatment and operator factors. Especially important are the starting malocclusion and the final outcome of orthodontic treatment.
The RCTs assessed in this review had considerable heterogeneity with regard to BR design and comparison group. Changes in stability were commonly assessed using LII. Even with a BR in place, some relapse in upper and lower incisor alignment seems inevitable.18,52,53,54,55,56,57 It is vital that patients appreciate that placing a BR does not eliminate the potential for change in labial segment alignment, but any change is likely to be small. Despite this, BRs appear to be more effective than VFRs at maintaining lower incisor alignment,18,52,53,54,55,56,57 and as effective at maintaining upper incisor alignment.54 These findings, however, are based on limited evidence. Clinicians have to weigh up the extra clinical time for themselves and patients in placing a BR versus the convenience of a VFR, albeit with a slight potential difference in alignment. The impact of compliance with retainer wear on any change in incisor alignment must also be discussed between the clinician and patient.15 In addition, patients appear to prefer BRs compared to VFRs, although there is conflicting evidence regarding survival and failure rates between these retainer types in the lower arch.44,54,60 As there appears to be no difference in the failure rate between BRs placed directly or indirectly, either technique is considered acceptable for placement. Additionally, BRs fabricated from multistrand SS and those from polyethylene ribbon retainer appeared to perform similarly.34,35,36
Importantly, from the RCTs reviewed, BRs do not appear to have significant adverse effects on oral health compared to VFRs up to four years after debond, but further follow-up is required.18,58,59 Studies are also required to investigate whether BR wear is associated with root resorption.
It is essential that the orthodontist provides guidance to the patient on the care and maintenance of BRs with an appropriate recall plan. This involves discussion with the patient during the informed consent process prior to starting orthodontic treatment.61 This should be reinforced before and after BR placement. While it is usual for the orthodontist to review the BR in the short term, in many cases this is not practical in the longer term.7,20
Patients, however, should be advised by the orthodontist that long-term regular review is necessary to check that the BR is ‘intact’ and dental tissues around the BR remain healthy.31 To this end, long-term surveillance regarding care and maintenance can be delegated to GDPs, as this is within their scope of practice, but only following discussion and mutual agreement with the orthodontist.62,63
A recall schedule with a checklist of what to ascertain regarding the BR and supporting tissues and instructions as to how this can be undertaken should be provided by the orthodontist. In particular, the review should include careful examination to ensure that the CR has not become detached from the enamel surface.
Recall intervals should be tailored to the individual patient. It has been recommended that the BR should be checked at least once every year.31 The BR review may be incorporated into the patient's regular check-up. Instructions for appropriate use of dental floss, ‘floss-spreaders’ and effective brushing to minimize plaque and calculus around the BR should be reinforced.31 Care should be exercised when scaling around the BR to avoid accidental ‘debonding’. Advice issued on placement in relation to cautious eating/chewing to avoid breakage, inadvertent activation or ‘debonding’ of the BR should also be repeated.23,32
If the BR is distorted, broken or has come off entirely, referral to a specialist orthodontist may be required as any unwanted tooth movement may require addressing.27 If the patient had been provided with a removable retainer at the end of orthodontic treatment, then the GDP should encourage its wear until the BR can be repaired. If the BR requires rebonding, and provided the GDP has received training and is confident to undertake the procedure, then the steps outlined in Table 6 should be followed.27,31,62,63,64
Procedure for repair of a BR
▪ Remove residual CR (tooth/teeth/BR) with fluted TCB/SSH Ensure BR not distorted
▪ Etch enamel (15–20 sec) with 35% phosphoric acid
▪ Rinse/dry thoroughly with moisture/oil-free air
▪ Isolate with rubber dam/cotton rolls/saliva ejectors
▪ Apply unfilled resin to etched surface
▪ Apply/adapt CR* to BR using TCI or foam MB dipped lightly in bonding agent
▪ Ensure CR covers middle third of crown, lies above and below wire and covers BR
▪ Light cure CR, ensure no ledge at tooth–CR interface
*With high filler content. TCI: Teflon-coated instrument. MB: Microbrush.
Conclusions
Indefinite retention is required to minimize movement of teeth after orthodontic treatment. Bonded retainers appear to be used more commonly than ever before. It is important, therefore, that the GDP be familiar with the characteristics of BRs and evidence relating to their effectiveness. It is also essential that the GDP should be aware of their role in the care and maintenance of BRs.