Renton TF. Inferior dental blocks versus infiltration dentistry: is it time for change?. Dent Update. 2019; 46:204-218
Endo T, Gabka J, Taubenheim L. Intraligamentary anesthesia: benefits and limitations. Quintessence Int. 2008; 39:e15-25
Shabazfar N, Daublander M, Al-Nawas B Periodontal intraligament injection as alternative to inferior alveolar nerve block – meta-analysis of the literature from 1979 to 2012. Clin Oral Investig. 2014; 18:351-358
Daublander M, Muller R, Lipp MD. The incidence of complications associated with local anesthesia in dentistry. Anesth Prog. 1997; 44:132-141
Mehdizadeh A. Anaesthesia: a sense of balance. Br Dent J (Letter). 2017; 223
Kammerer PW, Adubae A, Buttchereit I Prospective clinical study comparing intraligamentary anesthesia and inferior alveolar nerve block for extraction of posterior mandibular teeth. Clin Oral Investig. 2018; 22:1469-1475
Dumbrigue HB, Lim M V, Rudman RA A comparative study of anesthetic techniques for mandibular dental extraction. Am J Dent. 1997; 10:275-278
Kaufman E, Epstein JB, Cohen G A survey of pain, pressure, and discomfort induced by commonly used local anesthesia injections. Anesth Prog. 2005; 52:122-127
Reitz J, Reader A, Nist R Anesthetic efficacy of the intraosseous injection of 0.9 mL of 2% lidocaine (1:100,000 epinephrine) to augment an inferior alveolar nerve block. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998; 86:516-523
Roberts GJ, Simmons NB, Longhurst P Bacteraemia following local anaesthetic injections in children. Br Dent J. 1998; 185:295-298
Kämmerer PW, Palarie V, Schiegnitz E, Ziebart T. Clinical and histological comparison of pulp anesthesia and local diffusion after periodontal ligament injection and intrapapillary infiltration anaesthesia. J Pain Relief. 2012; 1:1-5
Anneroth G, Danielsson KH, Evers H Periodontal ligament injection. An experimental study in the monkey. Int J Oral Surg. 1985; 14:538-543
Venkat Narayanan J, Gurram P, Krishnan R Infiltrative local anesthesia with articaine is equally as effective as inferior alveolar nerve block with lidocaine for the removal of erupted molars. Oral Maxillofac Surg. 2017; 21:295-299
Thiem DGE, Schnaith F, Van Aken CME Extraction of mandibular premolars and molars: comparison between local infiltration via pressure syringe and inferior alveolar nerve block anesthesia. Clin Oral Investig. 2018; 22:1523-1530
Rayati F, Noruziha A, Jabbarian R. Efficacy of buccal infiltration anaesthesia with articaine for extraction of mandibular molars: a clinical trial. Br J Oral Maxillofac Surg. 2018; 56:607-610
Awal DH, Yilmaz Z, Osailan S, Renton T. Articaine-only buccal infiltrations for mandibular molar extractions: an alternative to inferior dental nerve blocks. Dent Update. 2017; 44:838-845
Kanaa MD, Whitworth JM, Corbett IP Articaine buccal infiltration enhances the effectiveness of lidocaine inferior alveolar nerve block. Int Endod J. 2009; 42:238-246
Kanaa MD, Whitworth JM, Corbett IP Articaine and lidocaine mandibular buccal infiltration anesthesia: a prospective randomized double-blind cross-over study. J Endod. 2006; 32:296-298
Chenchugopal M, Mungara J, Venumbaka NR In vivo evaluation of 4% articaine and 2% lignocaine intraligamentary injection administered with single tooth anesthesia-wand. Contemp Clin Dent. 2017; 8:315-320
Hopman AJG, Baart JA, Brand HS. Articaine and neurotoxicity – a review. Br Dent J. 2017; 223:501-506
McEntire M, Nusstein J, Drum M Anesthetic efficacy of 4% articaine with 1:100,000 epinephrine versus 4% articaine with 1:200,000 epinephrine as a primary buccal infiltration in the mandibular first molar. J Endod. 2011; 37:450-454
Olley RC, Renton T, Frost PM. Observational study investigating tooth extraction and the shortened dental arch approach. J Oral Rehabil. 2017; 44:610-616
This article reviews research and author experience behind Intraligamentary Local Anaesthesia (ILA) and Infiltration Local Anaesthesia (IFA) with Inferior Alveolar Nerve Block (IANB). In particular, the use of ILA with 4% articaine is discussed as an effective anaesthetic technique to replace both IANB and IFA for the purpose of tooth extraction in the posterior mandible. ILA also avoids the possible complications associated with IANB. Other advantages and some shortfalls of the ILA technique are described in relation to primary dental care. The technique for achieving ILA is described.
CPD/Clinical Relevance: The ILA technique with articaine is a simple, swift and effective alternative to IANB and IFA for extraction of posterior teeth in the mandible in primary dental care. ILA has fewer potential debilitating complications than IANB and is likely to be more effective than IFA.
Article
The Intraligamentary Local Anaesthetic (ILA) or ‘Periodontal Anaesthetic’ technique has been described as a misnomer, as it enters the cancellous bone through natural perforations and is, in effect, an intra-osseous, as opposed to a periodontal, local anaesthetic. In addition to the similar Infiltration Local Anaesthetic (IFA) or ‘Supraperiosteal Injection’ technique, the ILA is not commonly taught or used in dental schools for extraction of mandibular posterior teeth. The ‘go to’ method for anaesthesia of posterior teeth in the mandible has often been the Inferior Alveolar Nerve Block (IANB). A recent paper in Dental Update briefly mentions ILA as a useful anaesthetic technique for tooth extraction, that might replace IANB.1 In this review, research behind ILA is discussed in detail and compared with IANB and IFA. The anaesthetic and technique for ILA is also discussed for the purpose of extraction of posterior teeth in the mandible, with relevance to primary dental care.
ILA and IANB for posterior mandible dental extractions
The use of ILA was described in France in the early 20th century as a novel and effective method for achieving local anaesthesia in dentistry, but the technique did not become universally adopted owing to the inadequacy of instruments available at the time.2 Nowadays, modern instruments reduce pressure, pain and reversible changes to the soft tissues on injection, and the technique has limited side-effects when practised lege artis by an experienced operator.2
A meta-analysis of the literature from 1979−2012 compared ILA and IANB techniques for achieving anaesthesia in the mandible.3 Outcome criteria used included failure rates of both techniques, pain during injection, additional second injections, cardiovascular disturbances (CVD), and differences in method. The latter included unwanted side-effects, latency time, amount of anaesthetic agent and the duration of anaesthesia. There was large heterogeneity in methodology and reporting between studies and no clear advantage of one technique over the other was concluded. Indeed, studies involving pulpal testing of healthy teeth show that there are few differences in failure of anaesthesia between ILA and IANB techniques.3
However, more cardiovascular disturbances are reported in studies using IANB.3 In one study, there was significantly more risk of tachycardia, nausea, dizziness, agitation and tremor and a general feeling of unwellness (albeit transient) in patients, following IANB in contrast to ILA.4 This was especially true for 45.9% of the patients with risk factors (most of whom had CVD).4 The meta-analysis therefore brought into question the use of IANB for routine dental treatments and recommended more research.3 In addition, although the risk is very low, due to its method of application and risk of nerve contact, inferior alveolar nerve damage is more common following IANB.1 Furthermore, contact and damage of lingual and alveolar inferior nerves can result in loss of taste of the anterior two-thirds of the tongue. Impairment of buccal nerves could also result in loss of sensation to the ipsilateral side of the lower lip and soft tissue of cheek. However, it should be noted that no reports of permanent paraesthesia complications were found in the meta analysis.3 The reported risk of nerve injuries from IANB remains very low and reportedly ranges between 1:160,571 and 1:4,156,848.5
There are limited studies investigating ILA for extraction of mandibular molar teeth and fewer comparing ILA with IANB. Furthermore, studies are heterogeneous in methodology and definitions of failure.3 A recent prospective randomized study involved extraction of 301 mandibular posterior teeth in 266 patients using ILA or IANB with articaine.6 The study recommended ILA over IANB due to lower pain of injection, shorter latency time (ie quicker onset of anaesthesia), shorter duration of local numbness and requiring lesser amounts of anaesthetic solution.6 There was, however, similar anaesthetic quality during extractions between both ILA and IANB techniques.6 In contrast, another study reports ILA (with prilocaine) to be more painful than IANB (with prilocaine) and results in more pain during extraction of teeth, albeit with no difference in patient preference between ILA and IANB techniques.7 This is in contrast to the aforementioned study6 where the reported lower pain of injection (following ILA in contrast to IANB) is likely to be related to the pressure of application, which was limited to 120 N.6 In this regard, ILA pressure syringe systems can result in less painful anaesthesia than IANB. Conversely, other work in private dental practice using 2% lidocaine (1:100,000 adrenaline) demonstrates that IANB is more painful than ILA and IFA (even following topical anaesthetic application), despite more pressure recorded in application using ILA.8 Overall, outcomes to several studies on ILA and IANB are varied, but show limited differences in patient preference between IANB and ILA. The effectiveness of ILA therefore appears promising. In addition, work investigating the effectiveness of pulpal anaesthesia following IANB has shown the need for supplemental ILA in order to prolong anaesthesia.9 Considering the efficacy of ILA and possible risks of IANB, ILA would appear a safer and effective technique over IANB.
There are limited clear accounts of the deleterious effects of ILA in adults. The risk of bacteraemia has been reported in children following ILA (up to 97%), leading to a suggestion to avoid its use in infective endocarditis patients.10 However, in adults, there is a lack of research. Review papers recommend that ILA be avoided if significant inflammation is present at injection sites, in order to reduce the risk of bacteraemia.11 Other work conducted in monkeys also suggests a risk of tooth elongation and damage to periodontal ligament following ILA, although the histological effects are reversed within a week.12 This is perhaps an advantage rather than a contra-indication for exodontia.
IFA for posterior mandibular dental extractions
To the authors' knowledge, studies comparing IFA and ILA for the purposes of extraction of posterior mandibular teeth are missing. However, work has investigated buccal and lingual IFA using 4% articaine (1:100,000 adrenaline) in adult patients undergoing mandibular first and second molar extraction versus IANB using 2% lignocaine (1:80,000 adrenaline). It showed that there are insignificant differences in pain perception during extractions between IFA and IANB techniques.13 However, another recent prospective randomized study in private dental practice in Germany showed that IFA using 4% articaine and a pressure syringe system was not suitable for anaesthesia in the posterior mandible for tooth extractions, as anaesthesia was achieved in only 35% of cases, in contrast to anaesthesia in all cases using IANB and 4% articaine.14 Another randomized study of 133 patients requiring extractions of posterior mandibular teeth following buccal IFA showed that 4% articaine provided more effective anaesthesia and less pain than 2% lidocaine but, due to limited success rates, the article recommended that IFA could not be recommended over IANB.15
Another recent study in Dental Update, involving 112 patients in hospital in south London, showed that sufficient anaesthesia was achieved for mandibular molar tooth extraction in only 57% of patients using 4% articaine with buccal and lingual IFA.16 The remaining patients required top-up anaesthesia using IANB or additional IFA.16 Similarly, a study demonstrated only 56% effectiveness of pulpal anaesthesia in mandibular first molars following IANB with 2% lidocaine (1:80,000 adrenaline), which can be increased to 92% by supplementation using buccal IFA with 2% lidocaine (1:80,000 adrenaline).17
Based on the aforementioned studies, IFA appears a possible, albeit suboptimally effective, method of achieving anaesthesia for posterior mandibular tooth extractions. Like IANB, IFA often requires further IANB or additional IFA injections. This may relate to the position of delivery of anaesthetic using IFA and the thicker, denser bone in the posterior mandible. Anaesthetic delivery with IFA is not directly to the nerve through a block, or directly to the tooth periodontal ligament through an ILA injection.
Articaine
Articaine is a commonly used local anaesthetic for extraction of teeth using IFA and ILA. For the purpose of achieving pulpal anaesthesia of mandibular first molars using the IFA anaesthetic technique, prospective randomized double blind trials demonstrate the success of 1.8 mL of 4% articaine in almost two-thirds of cases, whilst 1.8 mL of 2% lidocaine (each with 1:100,000 adrenaline) in only around a third of cases.18 Conversely, another randomized study investigating anaesthesia for achieving pulpectomy showed little difference between 2% lidocaine and 4% articaine, each given by ILA, but this study was conducted on children.19 However, in the authors' experience, articaine has been used alone for many years by ILA to provide successful anaesthesia for extraction of posterior mandibular teeth in adult patients.
In regard to articaine concentration, retrospective studies suggest neurotoxicity at 4% (when used as an IANB) compared with other anaesthetics at lower concentrations.20 Nonetheless, this has been suggested as operator and technique dependant and influenced by reporter bias.20 Articaine has relatively low toxicity compared with other anaesthetics at similar concentrations.20
In addition, little difference has been demonstrated in terms of the efficiency of either 1:200,000 or 1:100,000 adrenaline for achieving pulpal anaesthesia.21 However, in a prospective study of 2731 patients in dental practices, more sympathomimetic side-effects were reported in articaine with 1:100,000 than 1:200,000 adrenaline.4
Technique for ILA with 4% articaine for posterior mandibular tooth extractions
Based on the above-mentioned work and author experience, IFA and IANB often rely on supplementation injections for the purposes of posterior tooth extractions in the mandible.22 In addition, there are significant, albeit low, risks using IANB as stated. The authors recently successfully extracted almost 300 consecutive mandibular posterior teeth in primary dental care over 16 years using 4% articaine and ILA alone. ILA offers a method of direct anaesthesia to the tooth to be extracted and may be adopted as the primary method for achieving anaesthesia for non-surgical posterior mandibular tooth extraction procedures.
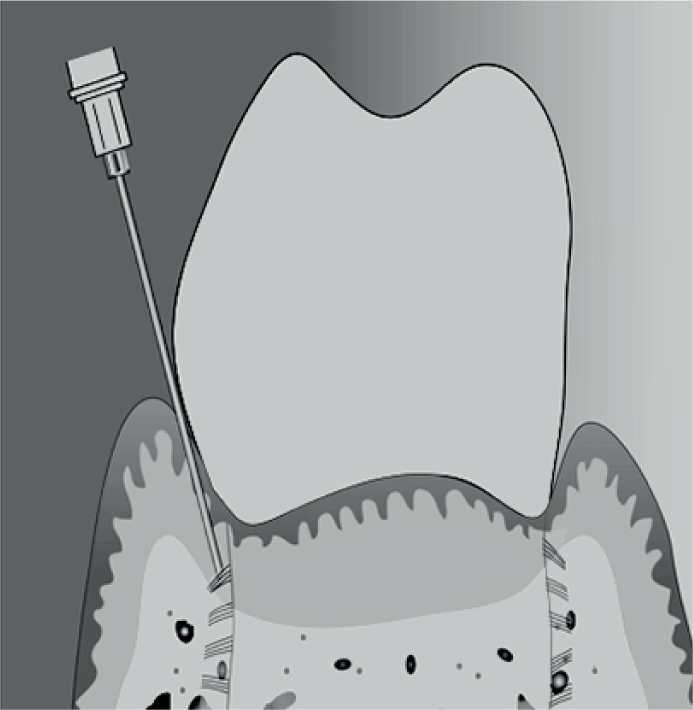
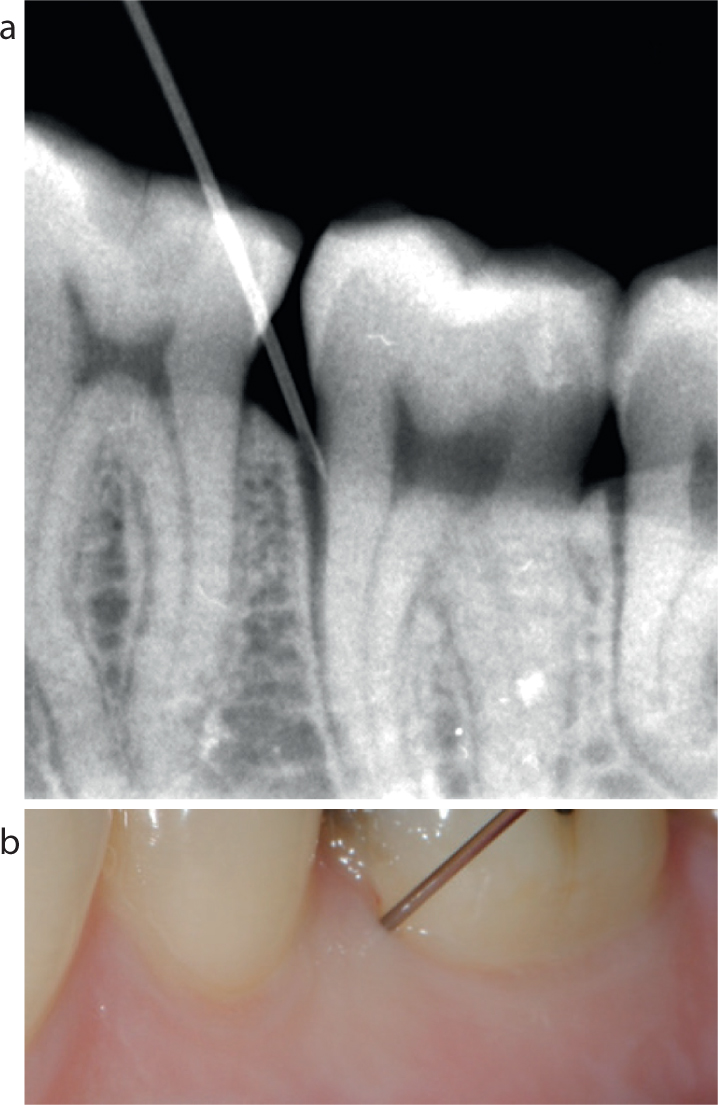
Based on the authors' experience from primary dental care, up to 1.8 mL (approximately 80% of a 2.2 mL cartridge) of 4% articaine hydrochloride (with 1:200,000 adrenaline) (Septanest, 1:200,000, Septodont®) may be given gently into the periodontal ligament of the tooth to be extracted. An intraligamentary syringe with pen grip (Septodont®) using a short 30-gauge needle (Septodont®) can be used, or alternatively a conventional anaesthetic syringe. If the latter, it is important to use gentle pressure using a skilful technique to avoid forcible injection,2 as mentioned previously. The needle bevel must face toward the tooth root. The 1.8 mL is spread over two sites buccal and two sites lingual per tooth until blanching of the mucosa appears circumferentially. Figures 1 and 2 show the position of the needle in the periodontal ligament diagrammatically, radiographically and photographically. The onset of anaesthesia is achieved within minutes (usually up to 5 minutes). The duration of anaesthesia for purposes of extraction is around 30 minutes and, in the authors' experience, few additional top-ups are required. This is likely because anaesthetic delivery occurs immediately adjacent to the tooth to be extracted.
Figure 1. Diagram showing buccal position of the needle in the periodontal ligament for ILA in a mandibular premolar tooth.Figure 2.
(a) Radiograph and (b) photograph showing the buccal-mesial position of the needle in the periodontal ligament, for ILA, in a mandibular molar tooth to be extracted.
ILA offers advantages insofar as small doses are required for extractions, up to 1.8 mL. The authors also find ILA a useful technique for patients with a severe gag response or who suffer trismus. However, ILA may not be suitable for procedures of longer duration. These would require repeat ILA anaesthesia involving multiple tissue injections. Another, albeit small, disadvantage of ILA is that anaesthetic solution may more readily leak into the oral cavity with an unpleasant taste. High volume suction is recommended.
Other suggested problems specific to the use of articaine ILA relate to the risk of osteonecrosis and periodontal damage or paraesthesia. Although periodontal damage is demonstrated in monkeys,12 there is limited clinical evidence for these other complications. In addition, the breakdown in periodontal ligament by ILA is an advantage for extractions.
It has also been suggested that written consent be obtained before administering any anaesthetic,20 perhaps more so for IANB. It is important for risks to be explained. Nonetheless, it is also suggested that, if clinicians took written consent for every anaesthetic administered, they would be overwhelmed by written consent for almost any procedure in dentistry.5
Conclusion
IANB carries more ‘potential’ risk than IFA and ILA. ILA, like IFA, offers safer alternatives to IANB for patients with CVD risks, bleeding diatheses or patients taking anti-coagulants.3 Likewise, the risk of direct nerve damage and paraesthesia is mitigated.
For the purpose of extraction of posterior mandibular teeth in adults, the effectiveness of IANB shows mixed or similar results to ILA and sometimes with the need for supplemental ILA following IANB. Similarly, IFA studies also show mixed and often poor results in achieving adequate anaesthesia for posterior mandibular extractions and often require supplemental IFA or IANB anaesthetic.
Based on this review, ILA offers a relatively safe alternative to IANB and is a more efficient substitute for IFA, for extraction of posterior teeth in the mandible in dental practice. Articaine (4%) is an effective and relatively safe anaesthetic for use with the ILA technique.