Hägg U, Taranger J. Timing of tooth emergence. A prospective longitudinal study of Swedish urban children from birth to 18 years. Swed Dent J. 1986; 10:195-206
Becker A, Chaushu S. Etiology of maxillary canine impaction: a review. Am J Orthod Dentofacial Orthop. 2015; 148:557-567
Stivaros N, Mandall N. Radiographic factors affecting the management of impacted upper permanent canines. J Orthod. 2000; 27:169-173
Peck S, Peck L, Kataja M. The palatally displaced canine as a dental anomaly of genetic origin. Angle Orthod. 1994; 64:249-256
Ericson S, Kurol J. Resorption of incisors after ectopic eruption of maxillary canines. A CT study. Angle Orthod. 2000; 70:415-423
McNair A, Morris D.London: British Orthodontic Society; 2010
Counihan K, Al-Awadhi EA, Butler J. Guidelines for the assessment of the impacted maxillary canine. Dent Update. 2013; 40:770-777
Husain J, Burden D, McSherry P.: Royal College of Surgeons (Eng), Faculty of Dental Surgery; 2016
Parkin N, Bazargani F, Benson PE, Atwal A. Interventions for promoting the eruption of palatally displaced permanent canine teeth, without the need for surgical exposure, in children aged 9 to 14 years (protocol). Cochrane Database Syst Rev. 2017; (10)
Naoumova J, Kurol J, Kjellberg H. Extraction of the deciduous canine as an interruptive treatment in children with palatal displaced canines – part I: shall we extract the deciduous canine or not?. Eur J Orthod. 2015; 37:209-218
Bazargani F, Magnuson A, Lennartsson B. Effect of interceptive extraction of deciduous canine on palatally displaced maxillary canine: a prospective randomized controlled study. Angle Orthod. 2014; 84:3-10
Parkin N, Benson PE, Thind B, Shah A, Khalil I, Ghafoor S. Open versus closed surgical exposure of canine teeth that are displaced in the roof of the mouth. Cochrane Database Syst Rev. 2017; (8)
Woloshyn H, Artun J, Kennedy D, Joondeph D. Pulpal and periodontal reactions to orthodontic alignment of palatally impacted canines. Angle Orthod. 1994; 64:257-264
Parkin N, Freeman J, Deery C, Benson P. Esthetic judgements of palatally displaced canines 3 months postdebond after surgical exposure with either a closed or an open technique. Am J Orthod Dentofacial Orthop. 2015; 147:173-181
Bazargani F, Magnuson A, Dolati A, Lennartsson B. Palatally displaced maxillary canines: factors influencing duration and cost of treatment. Eur J Orthod. 2013; 35:310-316
Thornton L. Anterior guidance: group function/canine guidance. A literature review. J Prosthet Dent. 1990; 64:479-482
Bishara S. Impacted maxillary canines: a review. Am J Orthod Dentofacial Orthop. 1992; 101:159-171
Robinson S, Chan M. New teeth from old: treatment options for retained primary teeth. Br Dent J. 2009; 207:315-320
Pjetursson B, Tan W, Tan K, Brägger U, Zwahlen M, Lang N. A systematic review of the survival and complication rates of resin-bonded bridges after an observation period of at least 5 years. Clin Oral Implants Res. 2008; 19:131-141
Wei Y, Wang X, Zhang Q, Li X, Blatz M, Jian Y, Zhao K. Clinical performance of anterior resin-bonded fixed dental prostheses with different framework designs: a systematic review and meta-analysis. J Dent. 2016; 47:1-7
Heinlein W. Anterior teeth: esthetics and function. J Prosthet Dent. 1980; 44:389-393
Chen P, Yu S, Zhu G. The psychosocial impacts of implantation on the dental aesthetics of missing anterior teeth patients. Br Dent J. 2012; 213
Rosa M, Lucchi P, Ferrari S, Zachrisson BU, Caprioglio A. Congenitally missing maxillary lateral incisors: long-term periodontal and functional evaluation after orthodontic space closure with first premolar intrusion and canine extrusion. Am J Orthod Dentofacial Orthop. 2016; 149:339-348
Cobourne M, DiBiase A., 2nd edn. London: Elsevier; 2015
Mirabella D, Giunta G, Lombardo L. Substitution of impacted canines by maxillary first premolars: a valid alternative to traditional orthodontic treatment. Am J Orthod Dentofacial Orthop. 2013; 143:125-133
Thiruvenkatachari B, Javidi H, Griffiths S, Shah A, Sandler J. Extraction of maxillary canines: esthetic perceptions of patients smiles among dental professionals and laypeople. Am J Orthod Dentofacial Orthop. 2017; 152:509-515
With the exception of third molar teeth, the maxillary canine is the most frequently impacted tooth, with the majority of these being palatally ectopic. When patients present with impacted canines there can often be several treatment options available to them. These could include interceptive treatment, exposure and alignment of the canine, extraction of the impacted tooth or acceptance of the deciduous canine. It is important that treatment decisions determining the ‘fate’ of palatally impacted canines should be taken on a case-by-case basis.
CPD/Clinical Relevance: The clinician should understand that several options might be available to the patient presenting with a palatally ectopic maxillary canine, in order to allow an informed choice of treatment.
Article
Leonie Seager
The maxillary canine tooth is usually one of the last teeth of the permanent dentition to erupt, normally between the age of 11 and 12 years.1 With the exception of third molar teeth, the maxillary canine is the most frequently impacted tooth, with a prevalence between 0.2%−2.8%, affecting female subjects 2.3−3 times more frequently than males.2
The majority of maxillary impacted canines are also ectopic, with literature showing 61% to be palatal and 35% buccal to the line of the arch.3
Aetiology of maxillary palatally impacted canines
The exact aetiology of palatal maxillary canine ectopia is unknown, although four distinct groupings of causation have been described:2
Local hard tissue obstruction;
Local pathology;
Departure from or disturbance of normal incisor development;
Genetics.
It is thought that the strongest influence for palatal canine impaction relates to local factors. The ‘guidance theory’ suggests that the lateral incisor is an important contributor to canine ectopia owing to a loss in guidance for the eruption path of the canine, which is the longest in the dentition, at a distance of 22 mm. This theory is supported by a significantly increased incidence of maxillary canine impactions in patients with missing, peg-shaped or microdont lateral incisors.2
However, genetics as a primary aetiological cause of canine impaction has also been considered4 due to its association with not only other dental anomalies, but also the presence of sex differences, population differences and familial occurrences. It is most likely that the aetiology of palatally ectopic canines is multifactorial.
It is also important to consider that buccally impacted canines should be described as separate aetiological entities from palatally impacted canines. Buccal impaction is usually associated with inadequate arch space, and eventual eruption of the canine will occur once space is made available. This is in contrast with palatally ectopic canines, which usually occur even in the presence of adequate arch space, and require surgical treatment and the application of orthodontic traction for eruption.4
Risks and consequences of canine impaction
A palatally impacted canine usually requires treatment for a variety of reasons, including the avoidance of possible pathological sequelae such as tooth resorption, cyst formation and infection.
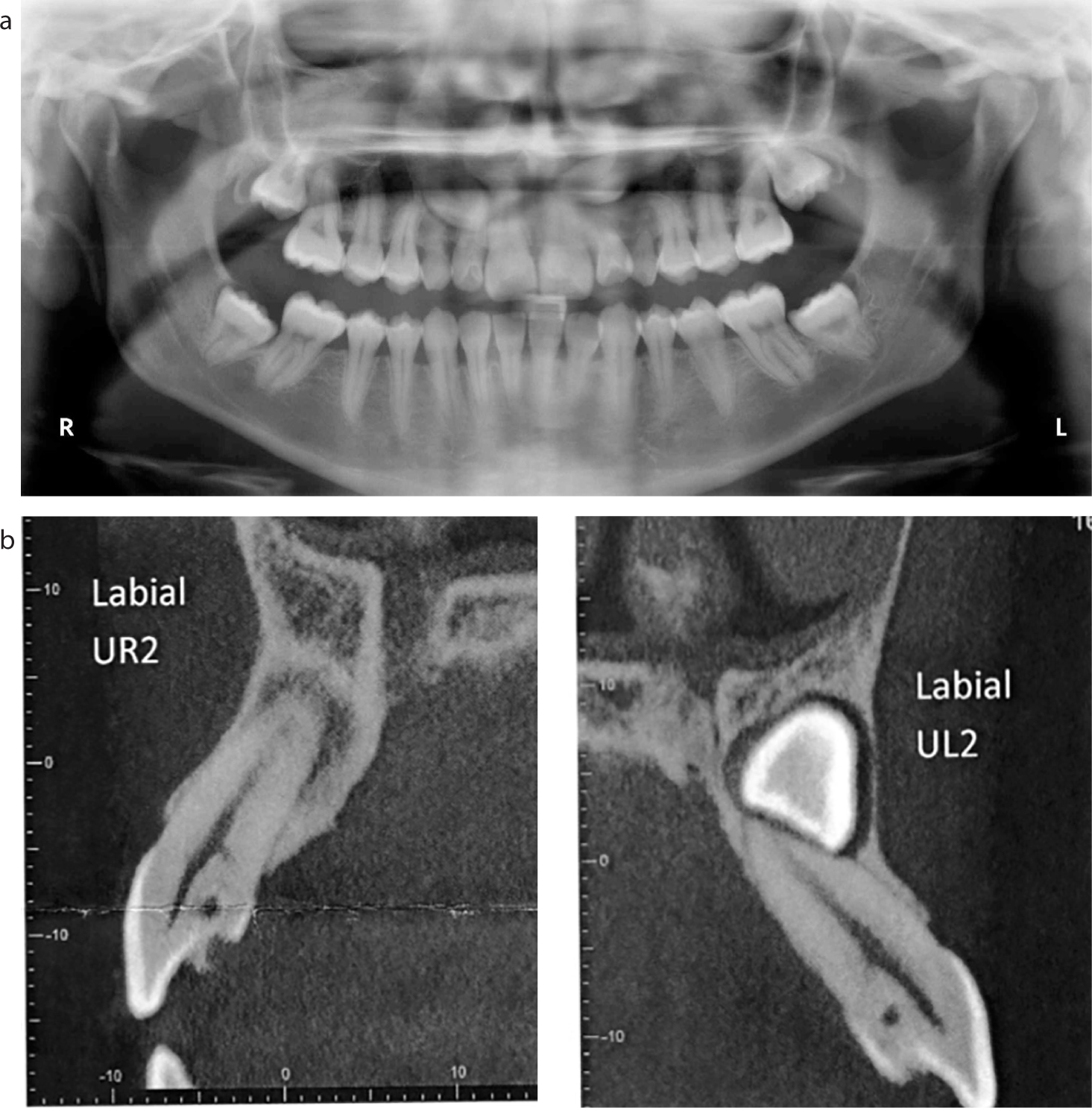
Root resorption of the adjacent lateral incisor as a result of canine impaction can be considerable, take place rapidly and unpredictably, and with a female preponderance. Cone Beam Computed Tomography (CBCT) studies have shown a 48% incidence of root resorption affecting the lateral incisors,5 a much higher percentage than that shown on plain films. Figure 1 demonstrates a case where root resorption of the lateral incisor was suspected on plain film and confirmed by CBCT.
Figure 1. Radiographic images demonstrating root resorption of lateral incisor due to an impacted canine: (a) plain radiograph; (b) part of CBCT image.
Canine impaction can also result in other negative sequelae such as:
Migration of the adjacent teeth and loss of arch length;
Cyst formation;
Ankylosis of the ectopic canine;
Spacing and centreline shifts.
Periodic radiographs, due to these potential complications, are recommended and the patient should be warned of the most common risks regarding the possibility of root resorption to adjacent teeth and cyst formation, should they choose to leave the tooth in situ.
Diagnosis
The accurate diagnosis of palatally impacted canines is obviously crucial before accurate and appropriate treatment planning can take place. It is recommended that palpation of unerupted canines should be a key part of a child’s dental examination so that appropriate referral to an orthodontist at a suitable age can take place should the canine(s) not be palpable. A favourably positioned canine is usually palpable buccal to the resorbing deciduous tooth by the age of 10−11 years. With regards to this and further information regarding radiographic diagnosis, the reader is referred to the British Orthodontic Society’s document Managing the Developing Occlusion.6 The subsequent process of then classifying the severity of the impaction, once it has been diagnosed, is also outside the scope of this article and the reader is directed to appropriate literature to ensure that they are proficient in diagnosing and classifying an impacted ectopic maxillary canine.7
Treatment choices
In line with the diagnosis and management of all patients, a comprehensive history as well as an examination is necessary upon patient presentation, as other factors may well influence the choice of treatment selected for treating the palatally impacted canine. Patient factors, such as the desire to undergo orthodontic treatment, should be considered as important as dental factors.
Making treatment decisions for cases with an impacted canine can often be difficult and, in many cases, several management options are available to the patient. On one hand, the desire to align the tooth, which is perceived to be important to both aesthetics and function, should be weighed against the knowledge that canine alignment treatment is likely to be time-consuming and potentially complex.
There can be several potential treatment choices available and these should be presented and discussed with the patient including:
Interceptive treatment should the patient present at the appropriate age.
No orthodontic or surgical treatment and acceptance of the dentition as it was at presentation with either:
– Maintenance of the deciduous canine, should it still be present, and with the understanding that it is likely to be exfoliated in the future;
– Acceptance of a gap in the canine region should spacing be present;
– A prosthetic replacement if space is available in the canine region.
Surgical exposure of the canine and orthodontic treatment to align it. This option might need to be taken in combination with extraction of an adjacent tooth if there are space requirements needed to align the canine.
Extraction of the impacted canine and orthodontic movement of the first premolar into its position.
Extraction of the impacted canine and acceptance of a gap or prosthetic replacement of the canine if there is space within the arch.
Autotransplantation of the canine. Whilst surgical exposure and alignment of a palatally impacted canine is usually possible, and is widely considered to be the gold standard treatment, it can substantially increase the overall treatment time and complexity, with the success of the result being heavily influenced by whether the treatment aims were achieved without the occurrence of any damage to the adjacent teeth.
These options will now be discussed in further detail in order to assist the reader in understanding the different options which might be presented to the patient and why a particular treatment choice may have been selected.
Interceptive management
Interceptive intervention involves the extraction of the deciduous canine in an appropriate aged patient, also often in combination with space creation mechanics, such as the use of a fixed appliance, headgear or expansion appliances such as Rapid Maxillary Expansion (RME) or a Quadhelix.
The impact of these interceptive approaches in preventing or altering canine ectopia has been considered in depth and the Royal College of Surgeons guidelines support the practice of extraction of the deciduous canine in order to try and change the path of development of the palatally displaced canine, the aim being an uneventful eruption of the canine into the dental arch.8 The evidence base for this recommendation is low as the 2012 Cochrane Systematic Review on the subject judged that there was ‘no reliable evidence with regard to the effects of primary canine extraction’. However, this Cochrane review has now been withdrawn and a new protocol submitted.9 This new review will hopefully help further guide clinicians by combining the findings of recently published randomized controlled studies, building upon the evidence base for effective interceptive intervention. These recent studies have demonstrated a 40% reduction in canine impaction when the deciduous canine was extracted,10 although variability in whether the permanent canine subsequently spontaneously erupted was high and the importance of the interception taking place when the patient is between 10 and 11 years old is emphasized.11 The criteria of subsequently ensuring that space is created within the arch, in combination with extraction of the deciduous canine in order to increase the effectiveness of the intervention, may also be important. As with all interceptive treatments, appropriate patient selection in terms of what the patient wants and is able to cope with should also be taken into account. If active orthodontic treatment is contra-indicated, or the patient is adamant that he/she would not be willing to consider fixed appliances later, then removal of the deciduous canine may also not be ideal, as it may commit the patient to later active treatment and remove the treatment option of accepting the deciduous canine long term. This should be borne in mind, particularly if the permanent canine is diagnosed as being unfavourably positioned and the deciduous canine has a minimally resorbed root and thus might be considered of favourable long-term prognosis.
Interceptive extraction of the deciduous canine undertaken at the correct time and in the right case should therefore be considered. It would be recommended that clinicians keep abreast of the literature in this area and take into account any recommendations made when the latest full Cochrane review is published, to ensure that they are following evidence-based practice.
Comprehensive management
Alignment of the canine
Alignment of a palatally ectopic canine will usually involve surgical uncovering of the tooth (exposure), followed by the use of fixed appliances to apply traction to the tooth to ensure its eruption and ultimate alignment within the dental arch. Two techniques are currently in use in the UK:
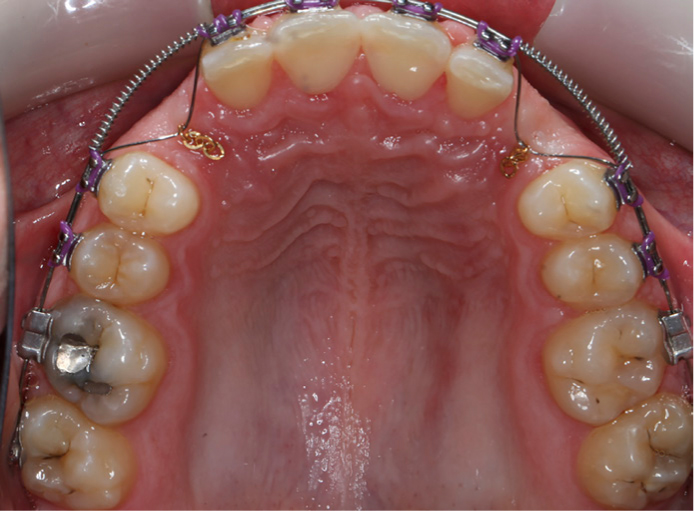
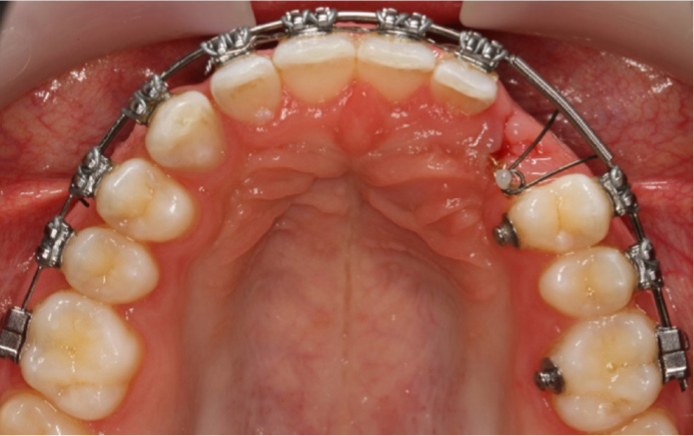
Closed exposure − involving surgical uncovering of the tooth, bonding of a gold eyelet and chain to the tooth and subsequent re-covering of the tooth and suturing of the mucosa with the tooth being moved into position covered by the palatal mucosa by the use of various mechanics such as ‘piggybacks’ (Figure 2) and/or ballista springs (Figure 3). Distalizing mechanics may also be used first to ensure that the crown of the impacted canine is away from the lateral incisor root prior to attempting orthodontic alignment (Figure 4).
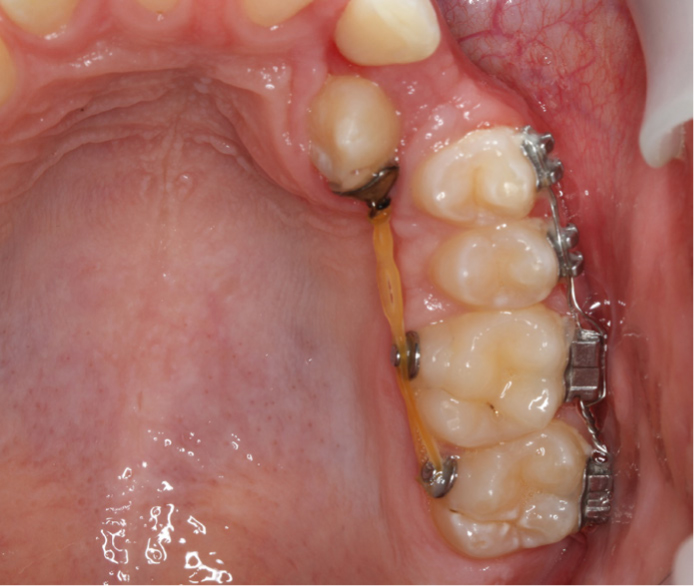
Open exposure − involving removal of the overlying palatal mucosa so that the tooth is visible. The orthodontist then bonds an attachment directly onto the tooth and is able to visualize the tooth as it is moved into position, often utilizing the same mechanics as those used in closed exposure cases (Figure 5).
Figure 2. Bilateral closed exposure of impacted canine with ‘piggyback’ mechanics to gold chains demonstrated.Figure 3. Balista spring mechanics.Figure 4. Distalizing mechanics used in a closed exposure case.Figure 5. An example of a bilateral open exposure case.
A recent Cochrane review12 consolidated the evidence base comparing the two techniques and concluded that currently ‘the evidence suggested that neither open nor closed surgical technique for exposing palatally displaced maxillary canine teeth is superior’. However, the evidence included in the review was described as being at high risk of bias. The review highlights that several ongoing clinical trials have been identified and will hopefully add to the evidence base in the future. Exposure and alignment of the impacted canine is considered to be the gold standard choice in the UK at this time and, whilst much of the evidence underlying this treatment choice is derived from case reports,8 clinical experience demands a respect for the excellent results that can be achieved by the surgical exposure and orthodontic alignment of a palatally impacted maxillary canine (Figures 6a and b). Nevertheless, the view of this treatment being the ‘gold standard’ to be undertaken in the majority of patients presenting with palatally ectopic canines is now being challenged, especially in the light of demands for quicker treatment times, reduced treatment risks and balancing resource efficiency with patient-centred outcomes.
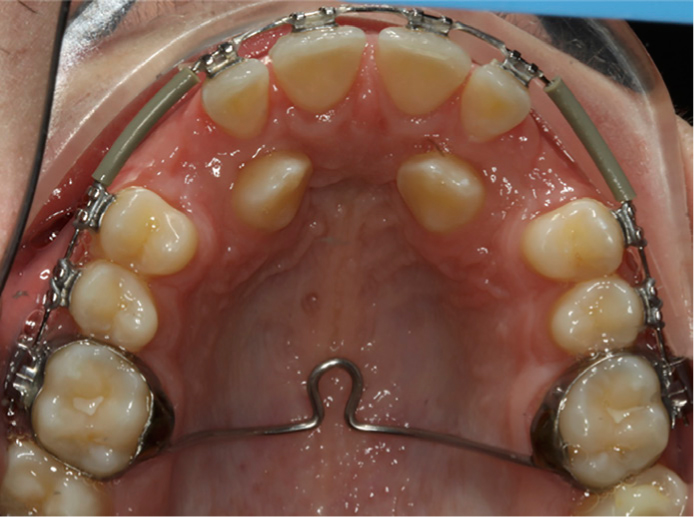
Figure 6.
(a). Pre-treatment image showing the retained ULC in situ. (b) Post-treatment image following alignment of palatally impacted UL3.
The generally perceived benefit of aligning an impacted canine tooth is that a more acceptable occlusal result is achieved (ie canine guidance or mutually protective occlusion rather than group function), as well as optimizing the aesthetic result in terms of achieving dental symmetry, proportions of the upper anterior dentition and an ideal emergence profile. The canine tooth is also arguably a desirable tooth to have functioning within the arch, as it is often seen to be one of the last-standing teeth in the partially dentate when all others have failed.
Despite canine alignment usually being considered as the preferred treatment choice by the orthodontic profession, adverse outcomes have been reported following orthodontic treatment to align an impacted maxillary canine. These include differences in tooth colour, alignment, vitality of the canine tooth, probing pocket depth, crestal bone and gingival margin height,13 as well as aesthetic differences between a previously palatally impacted canine, which had been aligned, and its contralateral partner, which had followed a normal path of eruption.14 This is demonstrated in Figure 7 where obvious torque discrepancies are evident post-treatment. However, there is also no evidence available which reports on the cosmetic importance of the canine and whether these findings have any effect on the patient’s satisfaction with treatment outcome.
Figure 7. Post-treatment image demonstrating aesthetic differences between a previously palatally impacted UR3 and the contralateral canine which erupted uneventfully without orthodontic assistance.
Aligning a palatally ectopic canine will also add time onto the expected length of average orthodontic treatment, with treatment expected to take at least 2−3 years from initial bond-up to brace removal. This can be further compounded the more unfavourably the canine is positioned, as well as by an advancing patient’s age.15 This may increase the risks associated with orthodontic treatment as well as testing patient co-operation and compliance, and the patient may demand that the brace is removed before the orthodontist is wholly satisfied with the canine’s position and/or torque. The presence of a canine-guided occlusion has also not been shown in the literature to confer any great advantage over functional occlusion,16 despite it being the popular choice and treatment aim for both orthodontists and prosthodontists.
Other possible treatment options
Alternative options to the alignment of a palatally ectopic canine include accepting the shape/size of the deciduous canine, if still present (or bonding resin composites to it to alter its appearance if space allows), accepting any residual spacing present, or substituting the first premolar tooth for the canine. Possible reasons for selecting an alternative treatment option to canine exposure and alignment could include:
The wish to avoid the occurrence of complications or reduce treatment time;
An unfavourable position of the impacted canine tooth;
Suspected ankylosis of the impacted canine tooth;
A severe arch length discrepancy where the first premolar has almost completely replaced the unerupted canine and therefore extraction of a unit would be required in order to align the impacted canine anyway.
Retention of the deciduous canine
It is commonly considered that the long-term prognosis of a deciduous canine would be poor, regardless of its root length or aesthetic acceptability of its crown.17 This view, however, is increasingly being challenged and many dental professionals have encountered patients where deciduous canines have been successfully retained for several decades in terms of function and aesthetics. Therefore, although literature confirming how long a deciduous tooth can be expected to survive, its acceptability to patients, as well as its impact on function is scarce, it can still be worthwhile to consider this treatment approach.18
There is also no evidence regarding how the retention of a deciduous canine may affect the aesthetics of the smile. The deciduous canine crown, in comparison to its permanent successor, is smaller in size but also lighter in colour. It is also likely to display an element of wear, although often if the deciduous canine lacks wear and exhibits a good size in relation to the permanent incisors, its presence may not be obvious at the patient’s dental check-up. This can sometimes contribute to a late diagnosis of a palatally ectopic permanent canine tooth.
One benefit of retaining the deciduous canine, especially if the root and coronal structure, as well as its function and aesthetics, are acceptable, is that, as well as minimal maintenance being required, bone and soft tissue architecture will be preserved. Figure 8 shows an OPG in a case where it was decided to retain the URC and extract the palatally impacted UR3. The OPG indicates a poor prognosis of alignment for UR3 as well as excellent root structure to the URC, which hopefully will correlate to intra-oral longevity. Should an aesthetic improvement be required to the deciduous canine, this can be easily achieved with composite additions.18 The patient should be warned that, when the primary tooth fails, it is likely that there may be insufficient space for an ideal-size prosthetic replacement, as the deciduous canine is notably smaller than its permanent counterpart (Figures 6a and b).
Figure 8. OPG radiograph of a case where it was decided to retain the URC and extract the impacted UR3.
The patient may also be restricted in what prosthesis can be supplied in the future, as it is likely that inadequate bone or space will be available for a dental implant. A resin-bonded bridge is therefore likely to be the restoration of choice and, with a 10-year survival of 65%, it should be anticipated that the patient may require several replacements during his/her life-time, depending on the patient’s age at the time when the deciduous canine is lost.19 A minimally invasive, cantilevered design appears to be the bridge design demonstrating the lowest clinical failure rate.20
Gaps
Should the patient’s deciduous canine be subsequently lost, he/she may also choose to accept a gap in the canine region. Although there are no studies that have specifically examined the impact of a gap in the canine area, since the canine tooth is positioned in the aesthetic zone, it can be postulated that it will have a significant impact on the patient’s aesthetic concerns and a prosthesis to fill a gap will most likely be requested if an anterior tooth is missing.
Results of previous research have indicated that edentulousness can have serious negative psychological and social quality of life implications, and it may therefore be a fair extrapolation that any missing maxillary tooth of the anterior segment may have a similar impact,21 although the replacement of these teeth with prostheses such as implants can subsequently improve psychosocial health.22 Therefore, it is highly likely that most patients would be unwilling to accept spacing in the canine region.
Premolar substitution
An alternative option of premolar substitution may seem particularly attractive when extractions would otherwise be required in order to make space for the subsequent alignment of the canine, as in a situation where the patient presents with severe arch-length discrepancy and the first premolar has almost completely replaced the position of the unerupted canine. In addition to a shorter treatment time, there is also no current evidence that the alignment of a canine over its substitution by a premolar for the sole purpose of attaining canine guidance leads to improved function. Indeed, research has shown that there is no increased risk of temporomandibular joint disorder in cases presenting with missing lateral incisors where space has been closed and first premolars substitute for canines.23
One of the reasons why it is postulated that the premolar might successfully be substituted for the canine is that the anatomy of the premolar crown has a buccal surface similar to the canine in terms of its convexity and cusp shape and therefore lends itself naturally to an effective camouflage (Figure 9). However, it also generally has a lower gingival margin and is usually narrower than the canine. Proponents of this treatment option therefore describe how the premolar can be effectively camouflaged, utilizing techniques24 such as:
Placing the premolar root more buccal in the maxilla to create a canine eminence;
Rotating the crown mesio-palatally to increase the mesiodistal tooth width, hide the palatal cusp and improve the occlusal relation with the mandibular canine;
Grinding the palatal cusp to reduce prominence;
Intrusion of the premolar to increase the gingival margin height combined with subsequent restorative build-up of cusp height.
Figure 9. Post-treatment image demonstrating bilateral premolar substitution for canines.
However, there is little evidence available to advise the clinician on whether any of these techniques make a difference in patient-related or aesthetic outcomes, with the majority of the literature being based on case reports.25 However, a more recently published retrospective study has aimed to investigate whether there is any difference in the perceptions of patients’ smiles treated by extracting either maxillary canines or first premolars, and has utilized investigating the judgement of not only orthodontists and dentists, but also laypeople.26 This study found no significant difference in the smile attractiveness between canine extraction and premolar substitution for any of the groups, suggesting that aligning canines may not necessarily give the best cosmetic result. This finding has potentially important ramifications as the smile aesthetics is often a primary motivating factor to those seeking orthodontic treatment. However, whilst premolar substitution might therefore seem like a good option in terms of smile aesthetics, research into the long-term survivability of a premolar functioning in a canine position is non-existent. This knowledge is arguably vital if the clinician is going to inform the patient about which option may give the best long-term functional as well as aesthetic result, and discuss the life-time consequences of such an orthodontic plan.
Conclusion
This article has set out to describe some of the options available for the management of a palatally ectopic maxillary canine, along with the evidence base behind the ‘success’ of these options. The importance of being able to explore and discuss each option in depth with the patient, following accurate diagnosis of a palatally impacted canine, is essential and forms the basis of informed consent. GDPs and orthodontists should realize that the traditional gold standard of aligning an ectopic palatally displaced canine might not be the only ‘fate’ available and, in certain situations, selecting a different option might be in fact in the patient’s best interests.