Safe prescribing in general dental practice – challenges and solutions Julie Mason Hannah Vallance Sarah Pontefract Jamie J Coleman Dental Update 2025 46:9, 828-835.
Authors
JulieMason
BSc, PhD, MRPharmS, AFHEA
SCRIPT Editorial Manager, University of Birmingham
Professor of Clinical Pharmacology and Medical Education, Institute of Clinical Sciences, College of Medical and Dental Sciences, University of Birmingham, Birmingham, B15 2SP; Honorary Consultant Physician/Associate Medical Director, University Hospitals Birmingham NHS Foundation Trust, Edgbaston, Birmingham, B15 2TT; Director, Yellow Card Centre West Midlands, City Hospital, Dudley Road, Birmingham, B18 7QH, UK
All dental practitioners will treat patients who take medicines. An ageing population, combined with improved management of patients with multiple long-term co-morbidities, has seen a rise in complex medication regimens. Healthcare specialization, a widening drug market and better access to medicines has also contributed to more patients taking multiple medicines for conditions, often managed by a variety of specialists. Whether these medicines are prescribed or bought over-the-counter, dental practitioners must understand the implications that these treatment regimens can have on dental care.
CPD/Clinical Relevance: Prescribing medicines is a small but essential part of dental practice. This paper describes various aspects of prescribing, the potential implications of dental treatment to a patient's medication regimen, and important considerations to reduce the risk of medication errors and improve patient safety.
Article
Julie Mason
In 2017, 4.7 million prescription items in England were prescribed by dentists, accounting for 0.4% of all prescriptions dispensed in the National Health Service.1 With an ageing population and advances in modern medical practice, the general dental practitioner (GDP) will increasingly be faced with patients who have multiple co-morbidities and are prescribed complex treatment regimens. GDPs, like other prescribers, need to have knowledge of the medicines they prescribe to inform prescribing decisions and non–pharmacological interventions. This article highlights some key prescribing considerations and provides links to resources that can support safe prescribing in dental practice.
Multimorbidity and polypharmacy
The UK population is ageing, with more than 11 million people over the age of 65 years.2 With ageing comes a greater likelihood of disease. More than 50% of those aged over 65 years are multimorbid3,4 (ie have two or more long-term conditions), and for those over 85 years this rises to more than 80%.5,6 Multimorbidity can lead to the prescription of multiple medicines, often known as polypharmacy.7 It is of particular concern in this patient group because the physiological changes that occur with age and/or chronic disease (eg decreases in lean body mass, body water, bone mass, renal clearance and hepatic function) can alter the pharmacokinetics and pharmacodynamics of a drug and increase the risk of Adverse Drug Reactions (ADRs), unless treatment regimens are adjusted accordingly. The use of multiple drugs also increases the potential for drug-drug interactions (DDI) and may lead to a cascade of prescribing where signs and symptoms of an ADR or DDI trigger prescription of more medicines where they are not needed,8 known as problematic polypharmacy.7 The safe prescription of medicines requires consideration of many issues.
Considerations when prescribing
Allergy status
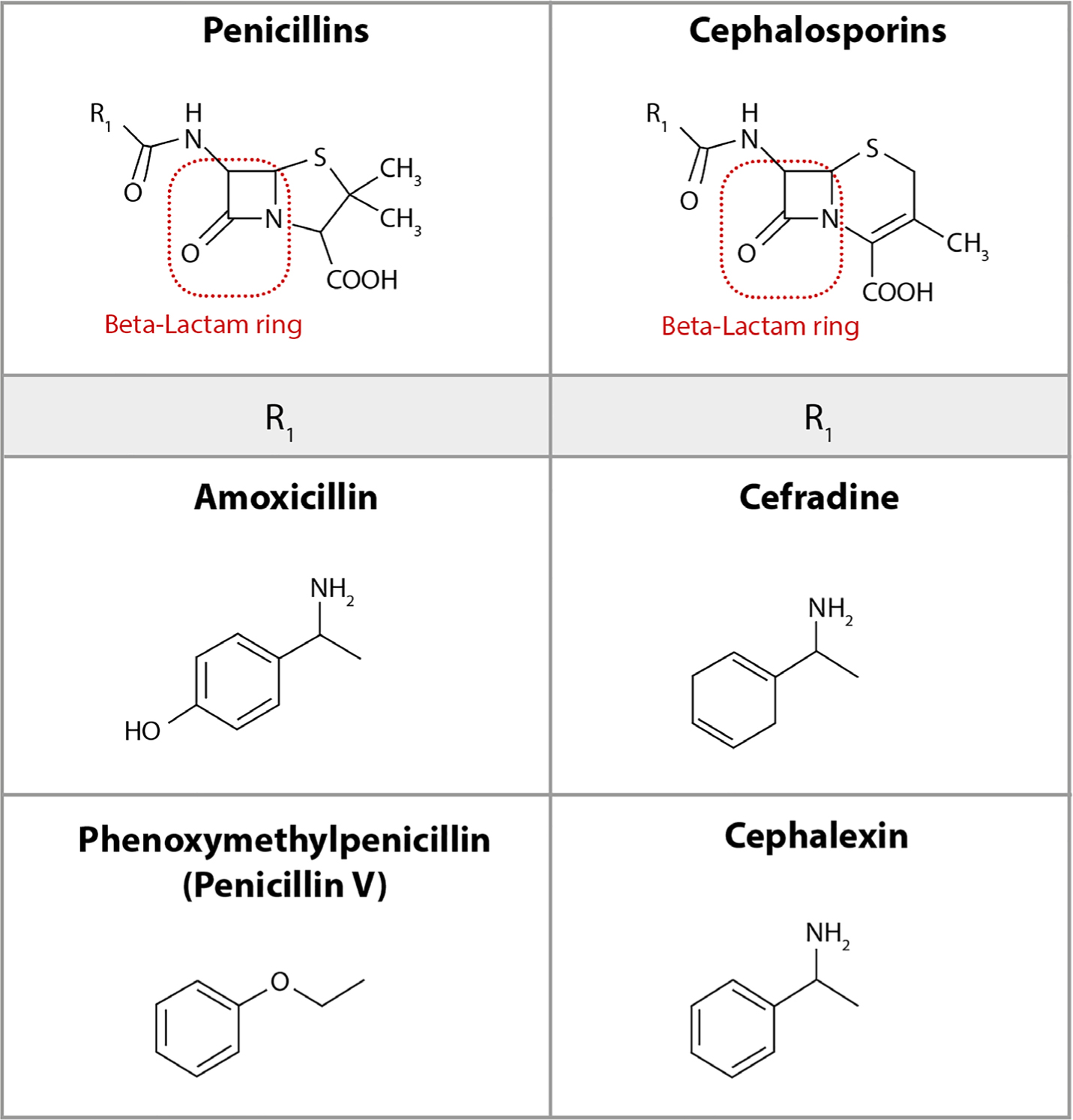
In 2017, amoxicillin was the most common drug prescribed by GDPs in England, accounting for nearly 42% of all items on FP10D.1 The allergy status of the patient should be established before prescribing antibacterials, especially to penicillins (eg amoxicillin, co-amoxiclav) as a true hypersensitivity reaction will limit what can be prescribed. A small proportion of patients with penicillin hypersensitivity may also have a similar reaction to cephalosporins (eg cephalexin, cefradine) known as cross-reactivity (Figure 1).9 Many patients may think that they are allergic to penicillins from previous adverse effects, such as diarrhoea and nausea, but careful questioning may reveal reactions that are neither anaphylactic nor serious in nature.
Figure 1. Cross-reactivity between penicillins and cephalosporins occurs in a small proportion of patients, thought to be due to structural similarities between the two drug classes.
Drug history
Alongside allergy status, it is important to find out what has been prescribed for patients and how adherent they are to their treatment. On average, patients with chronic disease only take about half of their doses as prescribed,10 and it is common for patients to forget to mention contraceptives, injections and inhaled or topical medicines. They may, when questioned, also need to be prompted to tell you about non-prescribed products, eg over-the-counter (OTC) medicines, herbal and complementary therapies, food supplements and recreational drugs. A comprehensive list and an appreciation of how the patient uses these products can help establish whether there are drug-related causes of symptoms or problems and inform dental prescribing decisions.
Hepatic and renal function
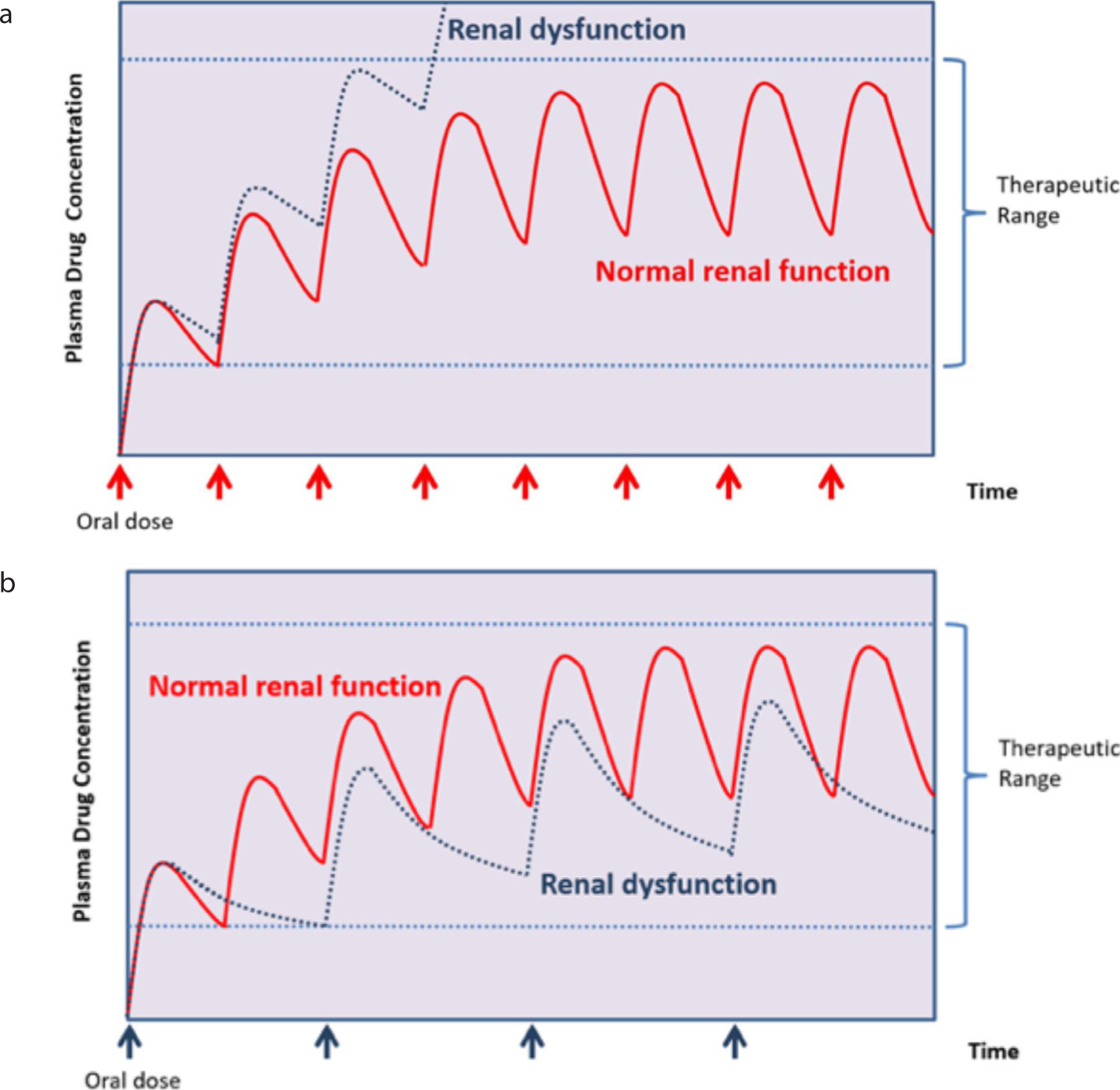
Approximately two-thirds of drugs are excreted via the kidney. If a patient has renal impairment, drugs which are excreted by the kidney, and sometimes their metabolites, can accumulate in the body and increase the risk of adverse effects. The plasma half-life of oral aciclovir, for example, increases from around 3 hours to more than 19 hours in a patient with chronic kidney disease.11 In patients with renal impairment, dose adjustments are required to reduce the risk of accumulation while maintaining a therapeutic effect (Figure 2). Adjustments can be made by decreasing the dose and/or by extending the duration between each dose. Specific drug monographs within the British National Formulary (BNF) state the appropriate approach.
Figure 2.
(a) In renal dysfunction, drugs excreted by the kidney can accumulate in the body, leading to plasma drug concentrations above the therapeutic range and increased risk of adverse drug reactions and toxicities. (b) Dose adjustments can be made by decreasing the dose and/or by extending the duration between each dose.
Patients with hepatic impairment may also require dose adjustments to take account of reduced drug metabolism. The liver metabolizes most drugs that enter the body to enable excretion by the kidneys. Dose adjustment in liver impairment is unpredictable and subject to interpatient variability. Treatment regimens have to be individually tailored to reduce accumulation risk and potential exacerbation of the adverse effects of liver disease. For example, encephalopathy in chronic liver disease can be precipitated by drugs that cause sedation, such as diazepam, or drugs that cause constipation, such as dihydrocodeine. The BNF provides guidance for individual drugs. However, it is often monitoring of outcomes and adverse effects which guides dosing and this frequently requires collaboration with, and follow-up by, doctors and other healthcare professionals.
Drug-drug interactions
The interaction between drugs, prescribed or non-prescribed, can have potentially serious consequences. Hepatic metabolism of drugs may be altered by the induction or inhibition of cytochrome P450 enzymes. Many drugs induce or inhibit these enzymes, which can result in clinically significant changes in plasma drug concentrations of other drugs. For example, carbamazepine is a potent enzyme inducer and increases the metabolism of warfarin, thereby reducing the anticoagulant effect. Inhibiting agents, such as omeprazole, macrolide antibacterials (eg erythromycin, clarithromycin), azole antifungals (eg fluconazole) and metronidazole, can increase plasma concentrations of co-administered drugs, such as warfarin, antiepileptics, some cytotoxic medicines and lithium.
Adverse drug reactions
Patients' previous ADRs should influence prescribing decisions. Susceptibility to ADRs varies dependent on the condition of patients and sometimes on their genetic profile. Many will be aware of the risk of gastrointestinal adverse events associated with non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen and diclofenac, but may not realize that their mechanism of action is to reduce prostaglandin synthesis, which can lead to renal hypoperfusion, fluid retention and acute kidney injury (AKI) in vulnerable individuals, eg patients with compromised renal function. Patients of Han Chinese and Thai family origin are more likely to have the HLA-B*1502 allele which predisposes them to Stevens-Johnson syndrome and toxic epidermal necrolysis with drugs like carbamazepine, and hence should be screened for this allele before it is prescribed for them.
It is also important to recognize that a patient's dental symptoms could be due to an ADR. Oral adverse effects, such as xerostomia, due to anticholinergic medicines like oxybutynin and amitriptyline, are well known to increase the risk of oral disease. Drug-induced gingival enlargement is known to be caused by calcium-channel blockers (eg amlodipine) in patients with poor oral hygiene.12 A more recent example has been the attribution of anti-resorptive (eg RANKL inhibitors such as denosumab) and anti-angiogenic medicines (eg bevacizumab, sunitinib and aflibercept) in causing medication-related osteonecrosis of the jaw (MRONJ) akin to that caused by bisphosphonate (eg alendronic acid) therapy.13,14,15 GDPs play an integral role in pharmacovigilance by reporting suspected ADRs for all prescription, OTC, herbal and homeopathic medicines using the MHRA yellow card scheme (https://yellowcard.mhra.gov.uk/).
Pregnancy and breastfeeding
Where possible, drugs should be avoided in pregnancy owing to potential harmful effects (eg carbamazepine is known to increase the risk of spina bifida and associated defects). If prescribing for a pregnant woman, it is important to establish the stage of pregnancy. Generally, the most vulnerable time of exposure is the first trimester when embryonic organ formation occurs. While desirable, it is not always possible to avoid drug treatment. If pain control is needed, NSAIDs, such as ibuprofen and diclofenac, should be avoided but paracetamol is considered safe if used at therapeutic doses and in short, occasional courses. Some antibacterials (eg penicillins and cephalosporins) are considered safe throughout pregnancy while others should be avoided. Metronidazole, for example, may have teratogenic effects if used in the first trimester and tetracyclines, such as doxycycline, have the potential to discolour the unborn baby's teeth if used in the second and third trimester.
It is important to remember that a drug that is safe to use during pregnancy is not necessarily safe for the breastfeeding patient. Virtually all drugs are excreted into breast milk to some extent and hence have the potential to affect a breastfed baby. Breastfeeding is, however, extremely beneficial to mother and child, and safe approaches to medicine use, such as taking medicines immediately after breastfeeding and avoiding modified release preparations, will allow treatment to continue while minimizing exposure to the child. The BNF provides information on drug use in pregnancy along with advice on use in breastfeeding.
Impact of medicines on non-pharmacological dental treatments
The medicines taken by patients can impact on the oral condition and dental treatment given by the GDP.
New drugs on the block
Anticoagulants and antiplatelets
Since their introduction in 2008, the use of direct oral anticoagulants (DOACs) has increased and they have now surpassed warfarin as the anticoagulant of choice.16 For DOACs there is no test to determine degree of anticoagulation. Procedures with a lower bleeding risk, such as simple extractions, can be conducted if the patient has normal renal function. DOACs have a much shorter serum half-life than warfarin and hence, for procedures with a higher risk of bleeding (eg complex extractions or more than three extractions at once), patients should be advised that, on the morning of the procedure, they should omit morning doses of twice daily DOACs (eg apixaban, dabigatran, etexilate) and delay doses of once daily DOACs (eg rivaroxaban, edoxaban) until four hours after haemostasis. On the other hand, patients taking antiplatelets (eg low-dose aspirin, clopidogrel, prasugrel and ticagrelor) are not recommended to omit doses prior to treatment, even if on dual antiplatelet therapy. Instead, for dental treatments associated with a higher risk of bleeding, a staged approach to treatment (eg multiple visits) should be considered along with local measures to achieve haemostasis (eg absorbable sutures or oxidized cellulose).
Biotherapeutics
Since the introduction of the monoclonal antibodies trastuzumab, infliximab and rituximab in the late 1990s, there has been rapid growth in the number of biotechnology-derived pharmaceuticals reaching the market. It is estimated that, at present, there are about 4000 biopharmaceuticals in clinical development accounting for more than 40% of drugs in the current drug pipeline.17 The majority of licensed biopharmaceuticals target cancer or immune-mediated diseases. Many biotherapeutics for both cancer and immune disease will be given in conjunction with systemic anticancer chemotherapy (SACT) (ie cytotoxic treatments) which leave the immune system compromised and the patient susceptible to infection. Each product will have its own unique safety profile and associated ADRs. Evidence of oral complications with these products is currently limited to case reports,18 and it is difficult to identify which of the adverse effects (eg xerostomia, oral mucositis) are due to concomitant SACT.
Sources of information
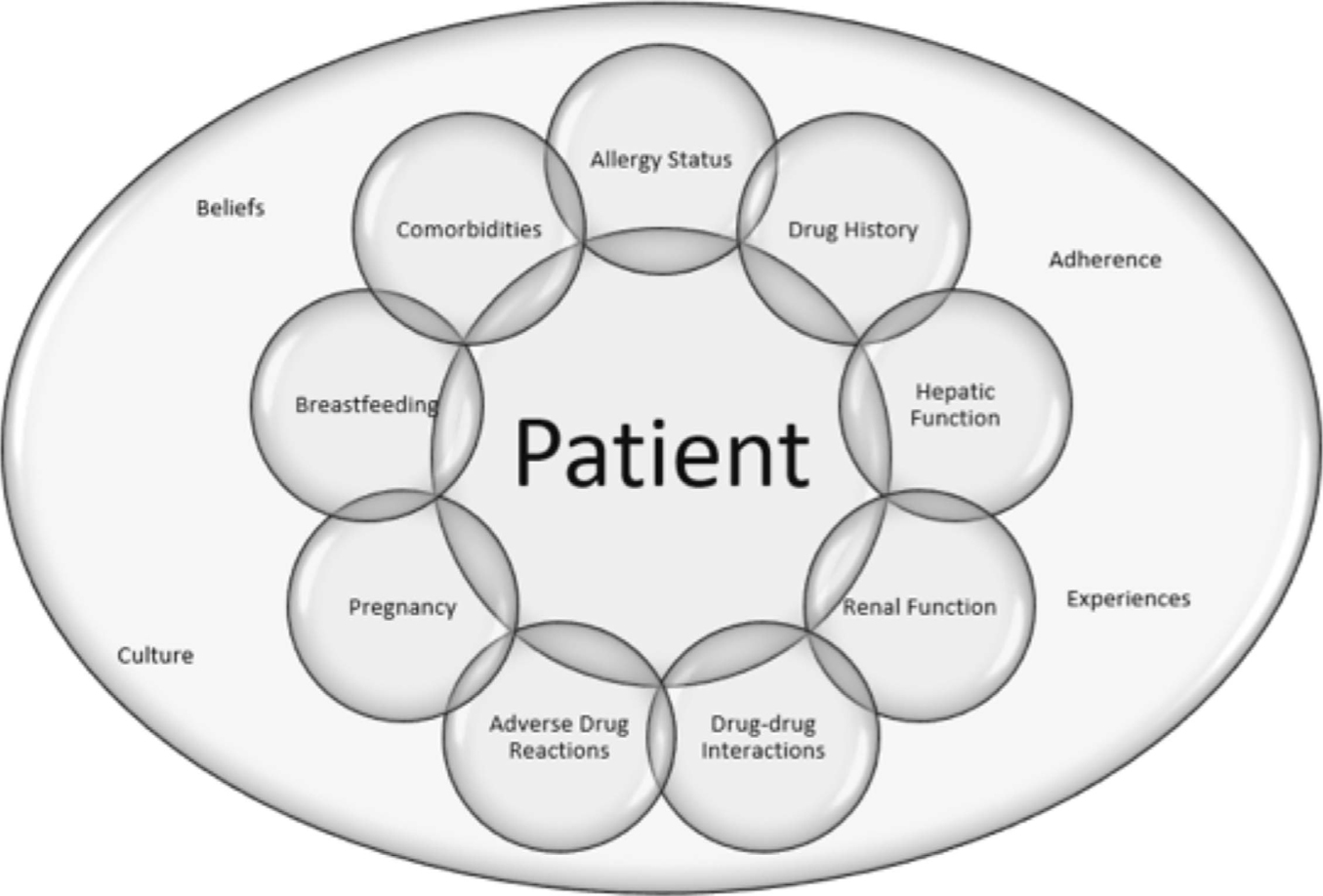
Prescribing is a complex process; patients and their medical needs should always be at the centre of the clinical decision-making process (Figure 3), which should be informed by local and national prescribing policy, protocols, formularies, guidelines and the best available evidence. The BNF treatment summaries, appendices and drug monographs provide information on how to prescribe, dispense and administer medicines safely. Each monograph contains all information relating to that drug, such as the recommended dose adjustments required in renal and hepatic impairment, monitoring requirements, and use during pregnancy and breastfeeding. The online versions of the BNF available at https://bnf.nice.org.uk/ allow you to search for drug-drug interactions while, in the hard copy, these are listed in the appendices. A summary of the licensing information for medicines with a marketing authorization (ie a summary of product characteristics) can be found in the online electronic medicines compendium (eMC) available at https://www.medicines.org.uk/emc. The Scottish Dental Clinical Effectiveness Programme (SDCEP) and the Faculty of General Dental Practitioners (FGDP) provide evidence-based guidance and recommend the most cost-effective prescribing. SCRIPT modules written for dentists bring the evidence together with practical prescribing scenarios to improve safe prescribing in dental patients. SCRIPT modules are available for continuing professional development and are freely available to all foundation trainee dentists in England at https://www.safeprescriber.org/. NHS Medicines Information services are available for simple or complex medication queries. Many hospitals will have a local medicines information service that will have access to specialist resources and information not readily available from usual reference resources. The contact details for regional specialist centres are listed in the BNF. The Specialist Pharmacy Service summarizes advice from UK Medicines Information which is available online at https://www.sps.nhs.uk/. A summary of resources can be seen in Table 1.
Figure 3. Patient-related factors for consideration when prescribing.
Resource
Information provided
Website
British National Formulary (BNF)
Information on how to prescribe, dispense and administer medicines safely. Free online access to the BNF is available through NICE
https://bnf.nice.org.uk/
Electronic Medicines Compendium (eMC)
Summaries of Product Characteristics, Patient Information Leaflets and Risk Minimization Materials for medicines licensed for use in the UK
https://www.medicines.org.uk/emc
MHRA Yellow Card Scheme
Reporting scheme for suspected adverse effects to drugs and medical devices, defective and counterfeit medicines. Provides information on suspected adverse reactions for all licensed drugs in the form of interactive Drug Analysis Profiles (iDAPs)
https://yellowcard.mhra.gov.uk/
NHS Medicines Information Services, UK Medicines Information (UKMi)
UKMi is part of the NHS Specialist Pharmacy Service. Freely accessible, it provides a wide range of information about the practical aspects of using medicines in any healthcare setting
Produces evidence-based guidance for dental practitioners, including a recently updated guide to Drug Prescribing for Dentistry
https://www.sdcep.org.uk/
SCRIPT eLearning
Eight interactive eLearning modules relating to prescribing and therapeutics for dentists. Each module takes around one hour to complete offering verifiable Continuing Professional Development for dental practitioners and a training resource for undergraduate and foundation dentists
https://www.safeprescriber.org/
Conclusion
In an ageing society, there are increasing numbers of co-morbid patients prescribed complex treatment regimens. The therapeutic armoury is growing rapidly with new medicines being introduced to increasingly complex treatment regimens. It is important that dental practitioners know where to find information about medicines and their impact on dental symptoms and treatments.