El-Naggar A, Chan J, Grandis J, Takata T, Slootweg P. WHO Classification of Head and Neck Tumours.Lyon, France: IARC; 2017
Barnes L. Pathology and Genetics of Head and Neck Tumours.Lyon, France: IARC; 2005
Song Y-L, Zhang W-F, Peng B, Wang C-N, Wang Q, Bian Z. Germline mutations of the PTCH gene in families with odontogenic keratocysts and nevoid basal cell carcinoma syndrome. Tumor Biol. 2006; 27:175-180
Johnson NR, Batstone MD, Savage NW. Management and recurrence of keratocystic odontogenic tumor: a systematic review. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013; 116:271-276
Surgical/orthodontic management of a large mandibular odontogenic keratocyst (OKC) Amarpreet Atwal Hannah Cottom Peter Doyle Jonathan Sandler Dental Update 2024 46:5, 707-709.
Authors
AmarpreetAtwal
BDS (Hons), MJDF, MOrth RCS
Post CCST Orthodontics, University of Sheffield and Royal Derby Hospital
The odontogenic keratocyst (OKC) is the third most common cyst of the jaw. OKCs are benign developmental cysts that are often locally destructive and large at presentation. They are usually identified during radiographic examination and require appropriate treatment planning to ensure optimal care. We present a very challenging case of a 12-year-old boy with a large mandibular OKC. The roots of several teeth were displaced, with both LR3 and LR5 unerupted and severely malpositioned. A multidisciplinary approach was therefore essential in view of the complexity, with joint planning and close liaison of treatment between the surgeon, orthodontist and general dental practitioner (GDP). This was fundamental to ensure the best possible outcome was achieved for the patient.
CPD/Clinical Relevance: This case report aims to increase awareness of OKCs to GDPs and outlines the surgical, orthodontic and restorative challenges faced in the management of such cases.
Article
Odontogenic keratocysts (OKCs) are benign developmental odontogenic cysts, which comprise approximately 10%–20% of all odontogenic cysts of the jaw.1 There is a peak in incidence in the second to third decade, with a greater prevalence reported in men compared to women (2:1).1 They occur most commonly in the mandible, especially the posterior body and angle regions, and almost always occur within bone, although a small number of peripheral OKCs have been reported.1 OKCs may initially appear small and unilocular, but early detection can be difficult, as they are often asymptomatic and growth is preferentially within the marrow spaces of the bone, with little cortical expansion. Therefore, OKCs are often detected later, when they are of a sufficiently large enough size to cause cortical expansion, perforation and affect adjacent structures.
In approximately 5%, OKCs may occur as part of Naevoid Basal Cell Carcinoma syndrome or Gorlin-Goltz syndrome.1 These syndromic cases tend to develop in younger patients, with greater tendency for multifocality and localization to the posterior maxilla.1 The OKC was renamed the Keratocystic Odontogenic Tumour (KCOT) in 2005 by the World Health Organization (WHO).2 At that time it was considered that this nomenclature more appropriately reflected its behaviour and proposed neoplastic nature. This was based on the knowledge that syndromic OKCs show mutation and inactivation of the PTCH1 gene, with a suggestion that the PTCH1 gene could also be important in the development of sporadic OKCs.2, 3 Similar genetic alterations have now been detected in other developmental cysts. Therefore, there is currently insufficient evidence to support a neoplastic nature of OKCs, which have now been reinstated as developmental in the current edition of the WHO Classification of Head and Neck tumours.1
Management of OKCs often involves surgery for complete enucleation of the cyst, but this can be difficult to achieve. Therefore, close monitoring is often undertaken over a five-year period due to the increased chance of re-occurrence.
Case history
A fit and well 12-year-old boy presented to his GDP with a large palpable bony swelling on the buccal aspect of the right body of the mandible. The patient had been aware of the swelling for approximately six months and reported no discomfort. On examination, there was no mental nerve paraesthesia or tooth mobility. The patient was referred to oral and maxillofacial surgery (OMFS) for further investigation of the lesion.
Investigations
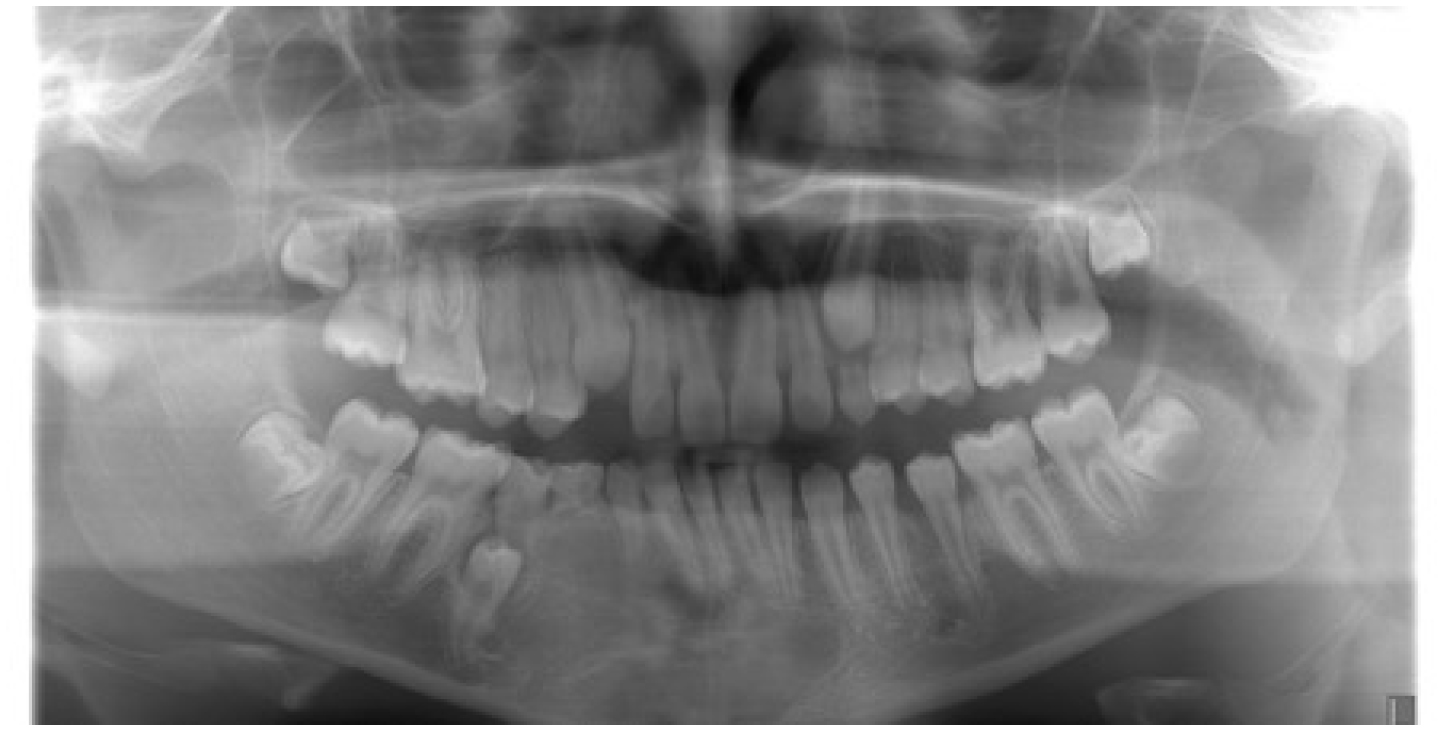
A Dental Panoramic Tomogram (DPT) revealed a large radiolucent lesion affecting the right body of the mandible extending into the left parasymphyseal region (from LR7 to LL3) (Figure 1). The lesion appeared to be unilocular with small incomplete bony septation noted in the region of a displaced LR5. The margins were well-defined, smooth and corticated. The lesion was associated with an unerupted LR3 lying horizontally along the lower border of the mandible and an unerupted LR5, which appeared to be wedged between the roots of LR4 and LR6. There was displacement of the roots of the lower incisors with the crowns of the incisor teeth displaced to the left.
Figure 1. Dental panoramic radiograph showing an extensive radiolucent lesion in the right body and left parasymphyseal region of the mandible.
Further imaging of the lesion with either conventional Computed Tomography (CT) or Cone Beam Computed Tomography (CBCT) was not considered necessary, as there was no evidence clinically or radiographically to suggest cortical perforation or soft tissue involvement.
Differential diagnosis
Due to the clinical and radiographic features of the lesion, the differential diagnoses were:
Dentigerous cyst;
Odontogenic keratocyst;
Ameloblastoma.
The most likely diagnosis was considered to be a dentigerous cyst, in view of the close association of the lesion with the unerupted LR3.
Treatment plan
Examination under general anaesthesia was scheduled. It was decided that if, during surgery, the intra-osseous lesion was obviously cystic, then complete enucleation would be carried out. If, instead, the lesion exhibited a solid or hard tissue component, an incisional biopsy would alternatively be performed. This would permit establishment of the histological diagnosis of the lesion, ensuring that the most appropriate surgical treatment was performed.
Orthodontic opinion was also crucial due to the extensive nature of the lesion and severe malposition of several teeth. It was decided that LR3 would be extracted due to its extremely unfavourable position and intimate relationship with the lesion, both of which precluded orthodontic alignment of the tooth. If possible, LR5 was to be left in situ (unless this compromised the surgical removal of the lesion) so that, once bony healing had occurred, LR4 could be mesialized orthodontically to allow the LR5 either to erupt of its own accord or be aligned following exposure and bonding of the tooth.
Surgical treatment
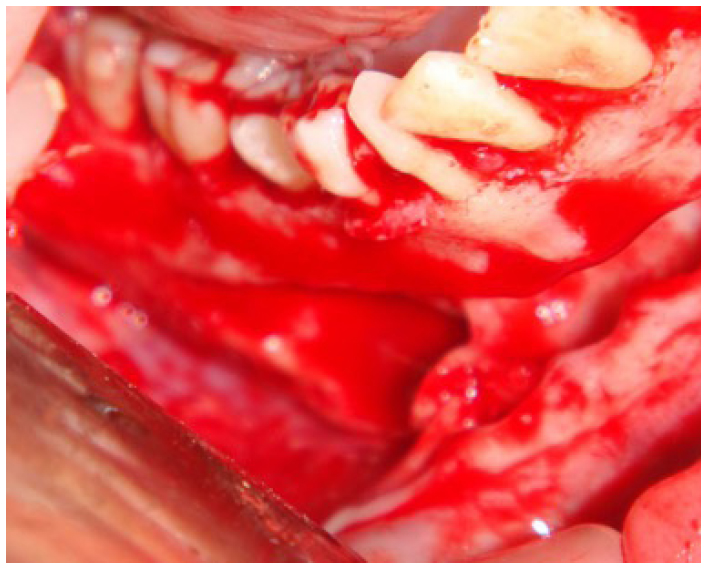
Under general anaesthesia, a buccal mucoperiosteal envelope flap was raised and the overlying bony window removed from LR7 to LL3 (Figure 2). The lesion appeared obviously cystic and therefore it was completely enucleated, together with surgical removal of LR3. The removed tissue was sent to histopathology for examination and analysis.
Figure 2. Operative view of the lesion following raising of a buccal envelope flap and removal of the overlying bone.
Histopathology
Histological examination of the enucleated cyst showed a convoluted cystic cavity lined for the most part by uniform, parakeratinized stratified squamous epithelium, with flattened rete processes. The epithelial lining demonstrated a well-defined, cuboidal to low columnar basal cell layer in areas, with evidence of nuclear palisading and reversed nuclear polarity; all characteristic features of an OKC. No satellite or daughter cysts were identified in the surrounding fibrocollagenous cyst wall and the epithelial lining demonstrated no significant cytological atypia.
Orthodontic treatment
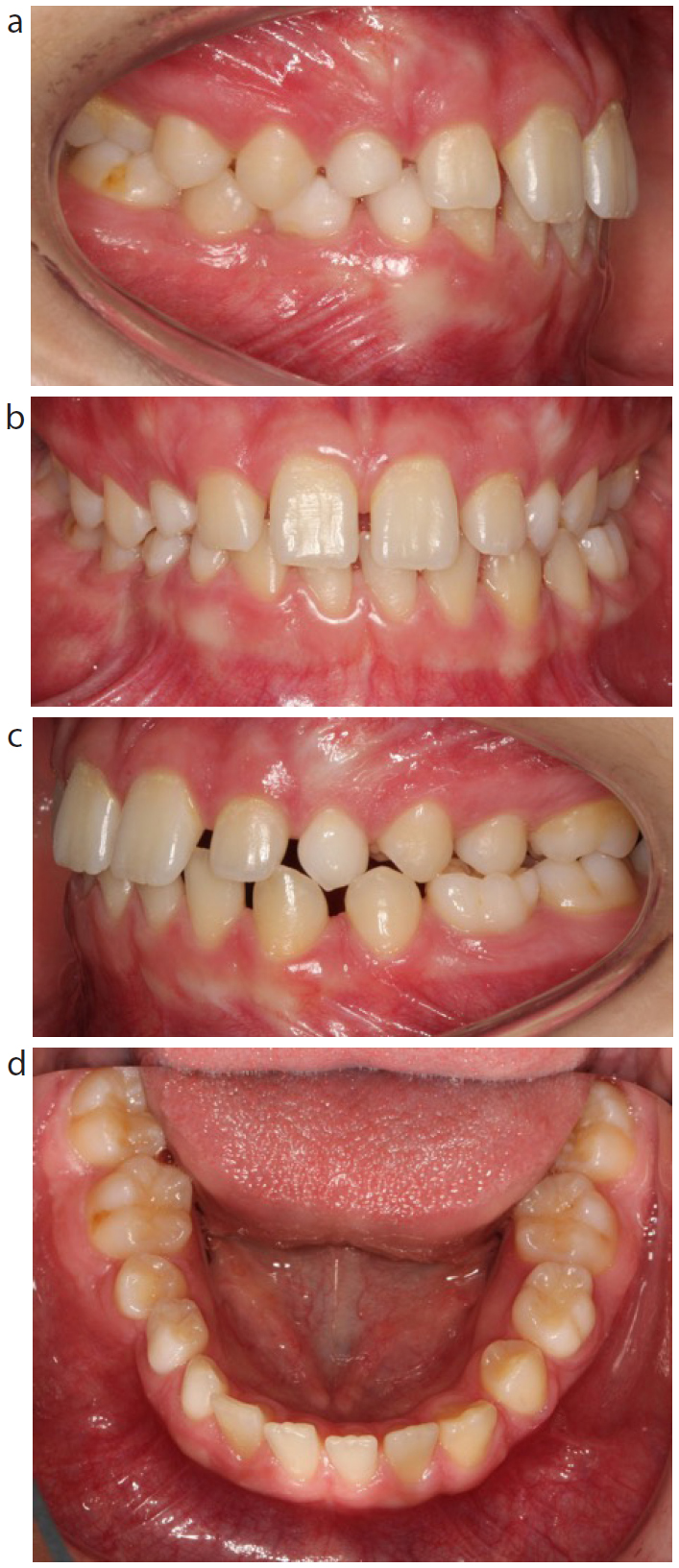
Following evidence of good bony healing, both clinically (Figures 3a–d) and radiographically (Figure 4), orthodontic treatment was commenced. This was approximately one year following successful enucleation of the cyst. All the remaining deciduous teeth, except LRC, were extracted, as LRC was planned to be incorporated into the fixed appliance. The patient was made aware that LRC would eventually be lost and require prosthetic replacement by the GDP.
Figure 3.
(a) Right buccal view prior to orthodontic treatment; (b) front view prior to orthodontic treatment; (c) left buccal view prior to orthodontic treatment; and (d) lower occlusal view prior to orthodontic treatment.Figure 4. Dental panoramic radiograph taken one year post surgery showing good bony infill of the cystic cavity.
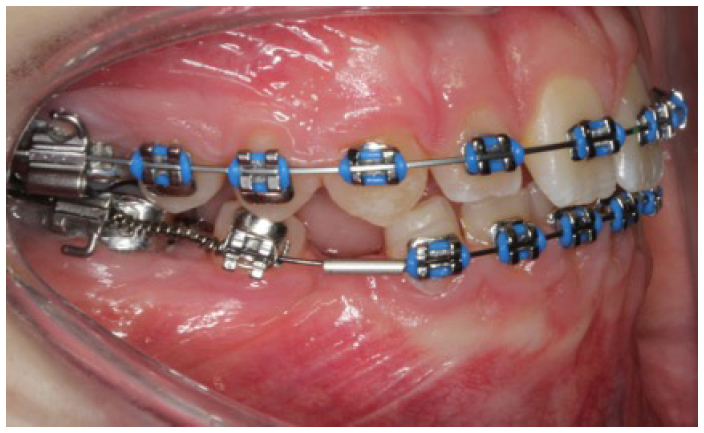
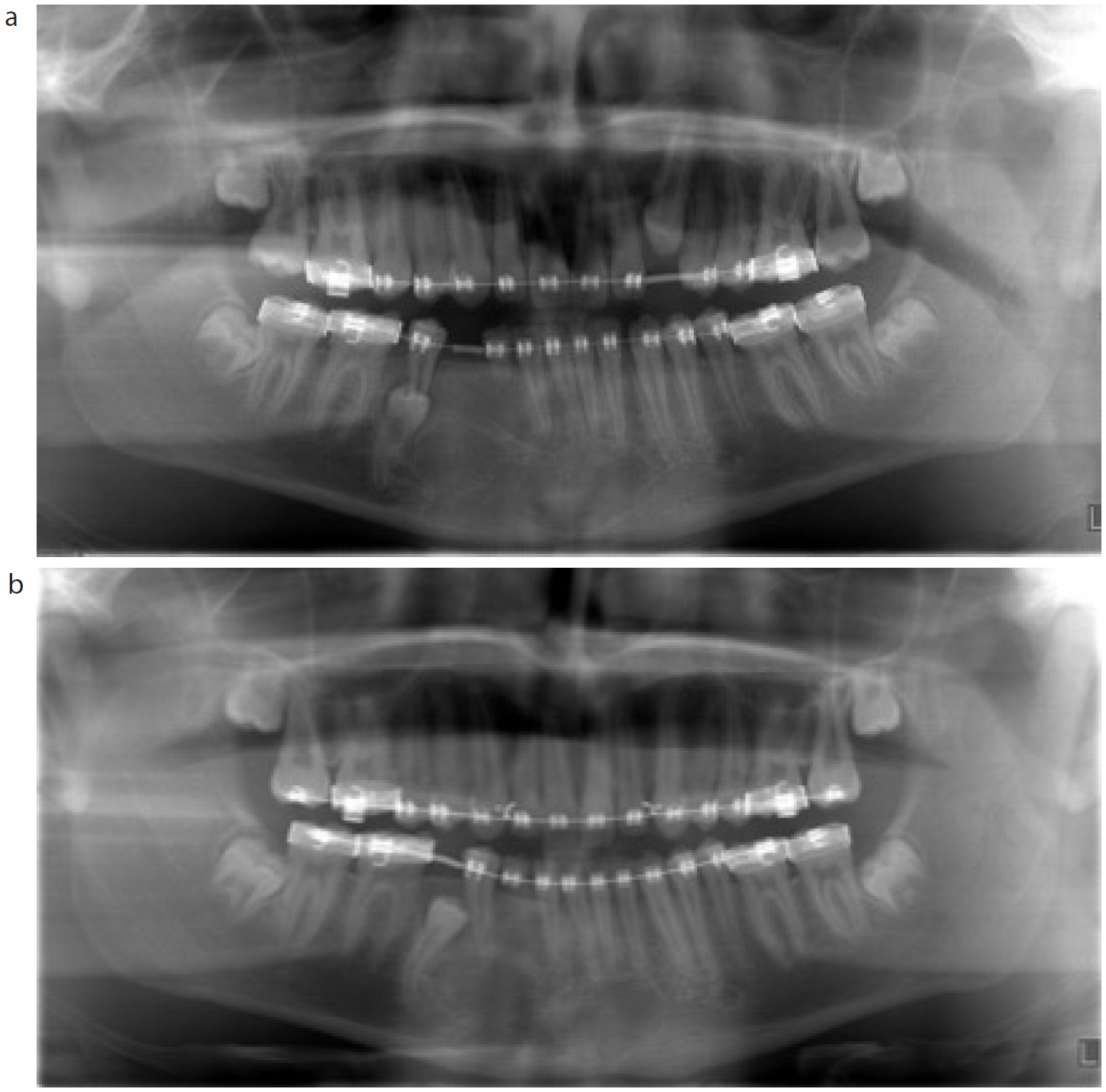
Upper and lower fixed appliances were placed and a compressed Nickel Titanium (NiTi) open coil spring was positioned on a rigid stainless-steel round archwire to start mesializing LR4 (Figure 5). A DPT was taken at the start of treatment (Figure 6a) and six months after mesialization of LR4 to create space to allow LR5 to erupt (Figure 6b).
Figure 5. Fixed appliance to mesialize LR4 with a compressed Nickel Titanium (NiTi) open coil spring.Figure 6.
(a) Dental panoramic radiograph taken prior to mesializing LR4. (b) Dental panoramic radiograph taken following mesialization of LR4.
LR5 did not erupt, but improved somewhat in position. The tooth was therefore exposed via a closed exposure technique under local anaesthetic, and a gold bracket and chain was attached to the tooth.
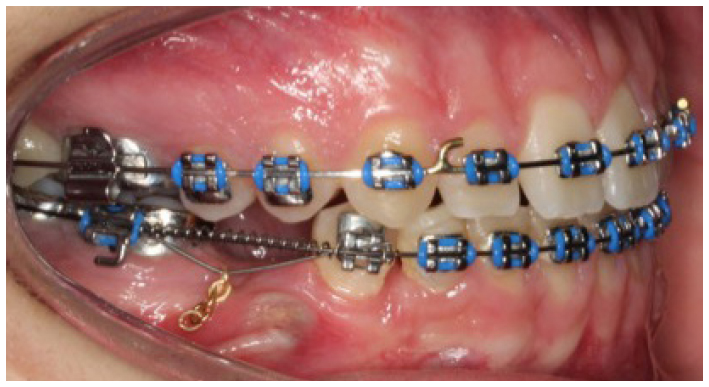
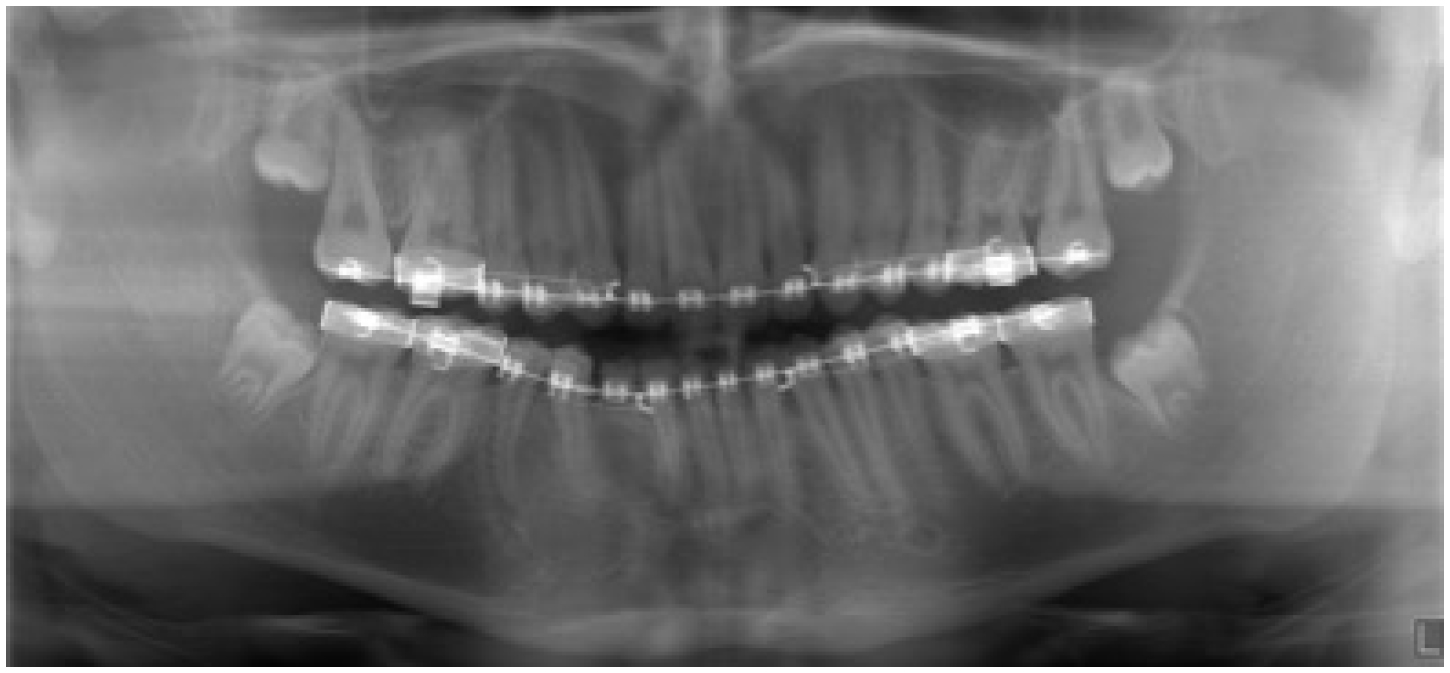
Orthodontic traction was applied to LR5 using piggyback mechanics (ie 0.016” Nickel Titanium (NiTi) piggyback archwire to the gold chain with a 0.016” stainless steel-based archwire) (Figure 7). A DPT was taken following successful alignment of LR5 a few months prior to removal of the upper and lower fixed appliances (Figure 8). It showed continued bony infill of the cyst, good alignment of the crowns and roots of the teeth and good remaining root length of LR4.
Figure 7. Piggyback mechanics with a 0.016” Nickel Titanium (NiTi) archwire to the gold chain attached to LR5 with a lower 0.016” stainless steel-based archwire.Figure 8. Dental panoramic radiograph taken prior to the removal of the upper and lower fixed appliances.
Outcome and follow up
Following natural exfoliation of LRC (Figure 9), the patient was provided with a resin-bonded bridge by his GDP to replace LR3 (Figures 10 a–d) and a new lower orthodontic vacuum-formed retainer was also constructed. The patient is under long-term review, both clinically and radiographically, due to the known propensity for OKCs to re-occur.
Figure 9. Right buccal view following removal of the fixed appliances and natural exfoliation of LRC.Figure 10.
(a) Right buccal view following placement of a resin-bonded bridge in the LR3 region; (b) front view at the end of treatment; (c) left buccal view at the end of treatment; (d) Lower occlusal view at the end of treatment.
Discussion
Syndromic and sporadic OKCs, whilst benign, can be locally destructive and are often large at presentation. They have a tendency to spread preferentially within the medullary cavity of the jaw (in a postero-anterior direction), often without causing significant cortical bony expansion. Patients may present with a variety of clinical features including swelling, pain, discharge, tooth mobility, bony perforation, or they may be, as with this patient, almost completely asymptomatic.
Radiographically, lesions are usually unilocular or multilocular radiolucencies surrounded by smooth or scalloped margins and sclerotic borders. The cysts are epithelial in origin and are considered developmental, arising from remnants of the dental lamina. They are usually identified on radiographic examination following localized destruction and growth within marrow spaces; which may become significant over time. Histological analysis is required to determine definitive diagnosis. Histologically, these cysts have a characteristic lining of parakeratinized stratified squamous epithelium with corrugated surface parakeratin, cuboidal to columnar basal cells which display nuclear palisading and reversed polarity. Their possible aggressive, locally infiltrative behaviour has been attributed to basal cell budding and greater mitotic potential.4
Treatment is frequently by surgical enucleation, with marsupialization very occasionally performed initially in extremely large lesions, in an attempt to reduce the size of the cyst and avoid jaw fracture during surgery. More aggressive approaches have been described, which include chemical curettage with Carnoy's solution to cause cellular death and bony resection, but these have a greater associated surgical morbidity. Recurrence is attributable to failure to remove the cyst lining completely and/or daughter cysts, with rates of between 8%–25% reported in the literature.5 Much lower rates have been cited following application of Carnoy's solution and resection.5
Orthodontic management of the patient involved a number of challenges. Good bony healing was required prior to commencing orthodontic tooth movement and vigilance was required during treatment by both the orthodontist, surgeon and GDP to detect any clinical or radiographic features that may suggest a re-occurrence of the OKC.
A decision was made to incorporate the LRC into the fixed appliance to prevent a long span of unsupported archwire, which could lead to flexing, breakages and difficulties mesializing LR4. However, this meant that LRC might undergo significant root resorption during orthodontic treatment. Consequently, the patient and his GDP were made aware that a prosthetic replacement would be required to restore LR3 following the loss of LRC. A significant amount of orthodontic tooth movement was required to mesialize LR4, increasing both the risk of root resorption of this tooth and the overall length of orthodontic treatment.
There was a risk that LR5 may have become ankylosed or could have proved difficult to align due to its extremely unfavourable original position close to the lower border of the mandible, almost complete root development and significant curvature at the root tip. A period of six months was allowed for LR5 to erupt spontaneously following creation of space by mesializing LR4 but, unfortunately, this only occurred to a limited extent. There was some improvement in position and therefore this was felt to be a good sign, indicating that the tooth should respond to orthodontic forces. Closed exposure and bonding of a gold chain to the tooth was therefore undertaken.
The alternative treatment plan of extraction of LR5 would have carried a significant risk of morbidity to the patient (ie mandibular fracture, mental nerve paraesthesia, damage to the adjacent roots, atrophy of bone and a large edentulous area to restore), therefore orthodontic alignment of LR5 resulted in the best possible outcome for the patient.
Conclusion
An odontogenic keratocyst should be one of the differential diagnoses of an asymptomatic mandibular swelling;
Orthodontic alignment of severely displaced teeth may not be feasible, in which case such teeth should be extracted;
Following orthodontic space creation, approximately six months should be allowed to observe if an unerupted tooth erupts of its own accord;
Close liaison in planning and treating such patients can lead to good outcomes for the patient.