Glossary of Endodontic Terms.: American Association of Endodontists; 1998
Gorjanovic-Kramberger M. The crowns and roots of the flag of the Homo primigenius and their genetic importance. Anat Anz. 1907; 31:97-134
Bharti R, Chandra A, Tikku AP, Wadhwani KK. ‘Taurodontism’ an endodontic challenge: a case report. J Oral Sci. 2009; 51:471-474
Benazzi S, Nguyen HN, Kullmer O, Hublin JJ. Exploring the biomechanics of taurodontism. J Anat. 2015; 226:180-188
Kupczik K, Hublin JJ. Mandibular molar root morphology in Neanderthals and Late Pleistocene and recent Homo sapiens. J Hum Evol. 2010; 59:525-541
Franciscus RG, Trinkaus E. Determinants of retromolar space presence in Pleistocene Homo mandibles. J Hum Evol. 1995; 28:577-595
Spencer MA, Demes B. Biomechanical analysis of masticatory system configuration in neandertals and inuits. Am J Phys Anthropol. 1993; 91:1-20
Coon CS. The Origin of Races.New York: Alfred A Knopf Inc; 1962
Hamner JE, Witkop CJ, Metro PS. Taurodontism; report of a case. Oral Surg Oral Med Oral Pathol. 1964; 18:409-418
Hillson S. Dental Anthropology.Cambridge: Cambridge University Press; 1996
Blumberg JE, Hylander WL, Goepp RA. Taurodontism: a biometric study. Am J Phys Anthropol. 1971; 34:243-256
Ten Cate AR. The role of epithelium in the development, structure and function of the tissues of tooth support. Oral Dis. 1996; 2:55-62
Hamner JE, Witkop CJ, Metro PS. Taurodontism. Report of a case. Oral Surg Oral Med Oral Pathol. 1964; 18:409-418
Greenberg MS, Glick M. Burket's Oral Medicine – Diagnosis and Treatment, 10th edn. Hamilton, ON, Canada: BC Decker; 2003
Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and Maxillofacial Pathology, 2nd edn. Philadelphia: WB Saunders; 2002
Keith A. Problems relating to the teeth of the earlier forms of prehistoric man. Proc R Soc Med. 1913; 6:(Odontol Sect)103-124
Varrela J, Alvesalo L, Mayhall J. Taurodontism in 45, X females. J Dent Res. 1990; 69:494-495
Mangion JJ. Two cases of taurodontism in modern human jaws. Br Dent J. 1962; 113:309-312
Chaparro González NT, Leidenz Bermudez JS, González Molina EM, Padilla Olmedillo JR. Multiple bilateral taurodontism. A case report. J Endod. 2010; 36:1905-1907
Radwan A, Kim SG. Treatment of a hypertaurodontic maxillary second molar in a patient with 10 taurodonts: a case report. J Endod. 2014; 40:140-144
Taurodontism: an anomaly of teeth reflecting disruptive developmental homeostasis. Am J Med Genet. 1988; 4:85-97
Vaughan MD, Rowland CC, Tong X Dental abnormalities in children preparing for pediatric bone marrow transplantation. Bone Marrow Transplant. 2005; 36:863-866
Reichart P, Quast U. Mandibular infection as a possible aetiological factor in taurodontism. J Dent. 1975; 3:198-202
Tsesis I, Shifman A, Kaufman AY. Taurodontism: an endodontic challenge. Report of a case. J Endod. 2003; 29:353-355
Manjunatha BS, Kovvuru SK. Taurodontism – a review on its etiology, prevalence and clinical considerations. J Clin Exp Dent. 2010; 2:e187-190
Jafarzadeh H, Azarpazhooh A, Mayhall JT. Taurodontism: a review of the condition and endodontic treatment challenges. Int Endod J. 2008; 41:375-388
White SC, Pharoah MJ. Oral Radiology. Principles and Interpretation, 5th edn. St Louis, USA: Mosby; 2004
Terezhalmy GT, Riley CK, Moore WS. Clinical images in oral medicine and maxillofacial radiology. Taurodontism. Quintessence Int. 2001; 32:254-255
Witkop CJ Clinical aspects of dental anomalies. Int Dent J. 1976; 26:378-390
Chaussain-Miller C, Sinding C, Wolikow M, Lasfargues JJ, Godeau G, Garabe'dian M. Dental abnormalities in patients with familial hypophosphatemic vitamin D-resistant rickets: prevention by early treatment with 1-hydroxyvitamin D. J Pediatr. 2003; 142:324-331
Aljamal GA, Hazza'a AM, Rawashdeh MA. Prevalence of dental anomalies in a population of cleft lip and palate patients. Cleft Palate Craniofac J. 2010; 47:413-420
Ruprecht A, Batniji S, el-Neweihi E. The incidence of taurodontism in dental patients. Oral Surg Oral Med Oral Pathol. 1987; 63:743-747
Llamas R, Jiminez-Planas A. Taurodontism in premolars. Oral Surg Oral Med Oral Pathol. 1993; 75:501-505
Dong J, Amor D, Aldred MJ DLX3 mutation associated with autosomal dominant amelogenesis imperfecta with taurodontism. Am J Med Genet A. 2005; 133A:138-141
Price JA, Wright JT, Walker SJ Tricho-dentoosseous syndrome and Amelogenesis imperfecta with taurodontism are genetically distinct conditions. Clin Genet. 1999; 56:35-40
Gomes RR, Calaca da Fonseca JA, Paula LM Prevalence of hypodontia in orthodontic patients in Brasilia, Brazil. Eur J Orthod. 2010; 32:302-306
Seow WK, Lai PY. Association of taurodontism with hypodontia: a controlled study. Pediatr Dent. 1989; 11:214-219
Lai PY, Seow WK. A controlled study of the association of various dental anomalies with hypodontia of permanent teeth. Pediatr Dent. 1999; 1:291-296
Bell J, Civil CR, Townsend GC The prevalence of taurodontism in Down's syndrome. J Ment Defic Res. 1989; 33:467-476
Alpöz AR, Eronat C. Taurodontism in children associated with trisomy 21 syndrome. J Clin Pediatr Dent. 1997; 22:37-39
Jaspers MT. Taurodontism in the Down's syndrome. Oral Surg Oral Med Oral Pathol. 1981; 51:632-636
Alpöz AR, Eronat C. Taurodontism in children associated with trisomy 21 syndrome. J Clin Pediatr Dent. 1997; 22:37-39
Schulman GS, Redford-Badwal D, Poole A Taurodontism and learning disabilities in patients with Klinefelter syndrome. Pediatr Dent. 2005; 2:389-394
Simpson JL, de la Cruz F, Swerdloff RS. Klinefelter syndrome: expanding the phenotype and identifying new research directions. Genet Med. 2003; 5:460-468
Darbyshire PA, Witkop CJ, Cervenka J. Prepubertal diagnosis of Klinefelter syndrome in a patient with taurodontic teeth. Pediatr Dent. 1989; 11:224-226
Guven Y, Rosti RO, Tuna EB Orodental findings of a family with lacrimoauriculo-dento digital (LADD) syndrome. Oral Surg Oral Med Oral Pathol. 2008; 106:e33-44
Martins F, Ortega KL, Hiraoka C Oral and dental abnormalities in Barber-Say syndrome. Am J Med Genet A. 2010; 152A:2569-2573
Lichtenstein JF, Warson R, Jorgenson R The tricho-dentoosseous (TDO) syndrome. Am J Hum Genet. 1972; 24:569-582
Koshiba H, Kimura O, Nakata M Clinical, genetic, and histologic features of the trichoonychodental (TOD) syndrome. Oral Surg Oral Med Oral Pathol. 1978; 46:376-385
Goldstein E, Medina JL. Mohr syndrome or oral facial-digital II: report of two cases. J Am Dent Assoc. 1974; 89:377-382
Nawa H, Oberoi S, Vargervik K. Taurodontism and Van der Woude syndrome. Is there an association?. Angle Orthod. 2008; 78:832-837
Tomona N, Smith ACM, Guadagnini JP Craniofacial and dental phenotype of Smith-Magenis syndrome. Am J Med Genet. 2006; 140A:2556-2561
Gros CI, Clauss F, Obry F Quantification of taurodontism: interests in the early diagnosis of hypohidrotic ectodermal dysplasia. Oral Dis. 2010; 16:292-298
Schalk-van der Weide Y, Steen WH, Bosman F. Taurodontism and length of teeth in patients with oligodontia. J Oral Rehabil. 1993; 20:401-412
Varrela J, Alvesalo L. Taurodontism in 47, XXY males: an effect of the extra X chromosome on root development. J Dent Res. 1988; 67:501-502
Jaspers M, Witkop C. Taurodontism: an isolated trait associated with syndromes and X-chromosomal aneuploidy. Am J Hum Genet. 1980; 32:396-413
Alvesalo L, Varrela J. Taurodontism and the presence of an extra Y chromosome: study of 47, XXY males and analytical review. Hum Biol. 1991; 63:31-38
Hazza'a AM, Al-Jamal G. Radiographic features of the jaws and teeth in thalassaemia major. Dentomaxillofac Radiol. 2006; 35:283-288
Akintoye SO, Lee JS, Feimster T, Booher S, Brahim J, Kingman A Dental characteristics of fibrous dysplasia and McCune-Albright syndrome. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003; 96:275-282
Axelsson S, Bjornland T, Kjaer I, Heiberg A, Storhaug K. Dental characteristics in Williams syndrome: a clinical and radiographic evaluation. Acta Odontol Scand. 2003; 61:129-136
Joseph M. Endodontic treatment in three taurodontic teeth associated with 48, XXXY Klinefelter syndrome: a review and case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008; 105:670-677
Marques-da-Silva B, Baratto-Filho F, Abuabara A Multiple taurodontism: the challenge of endodontic treatment. J Oral Sci. 2010; 52:653-658
Patel S, Dawood A, Mannocci F Detection of periapical bone defects in human jaws using cone beam computed tomography and intraoral radiography. Int Endod J. 2009; 42:507-515
Bean LR, Akerman WY Intraoral or panoramic radiography?. Dent Clin North Am. 1984; 28:47-55
Shifman A, Buchner A. Taurodontism. Report of sixteen cases in Israel. Oral Surg Oral Med Oral Pathol. 1976; 41:400-405
Durr DP, Campos CA, Ayers CS. Clinical significance of taurodontism. J Am Dent Assoc. 1980; 100:378-381
The first article described history, aetiology, molecular signalling mechanism, epidemiology and classification of taurodontism. This final article of the two-part series focuses on the biomechanics and other clinical aspects of taurodontism.
In certain disorders, especially during initial stages, the teeth can appear taurodontic and may complicate diagnosis. These conditions, along with their key features, are highlighted in this article, as are several syndromes relevant to taurodontism. In addition, the sections on imaging and clinical considerations discuss diagnostic methods and management of taurodontic teeth, respectively. Taurodontism, especially in severe forms, can be a root canal challenge. Sometimes, multiple taurodontism is seen in association with various syndromes and perhaps may assist in early diagnosis.
CPD/Clinical Relevance: Taurodontism has clinical implications in various dental disciplines, such as endodontics, surgery, orthodontics and prosthodontics. However, it is most relevant to endodontists as this deviation exclusively affects the internal anatomy of teeth.
Article
The second article of this two-part series aims to review the biomechanics of taurodontic teeth, their diagnostic considerations, relevant syndromes, imaging methods, clinical management and prognosis. The hallmarks of taurodontism are:
Vertically enlarged pulp cavities;
Apically displaced pulpal floor and furcation;
Lack of cervical constriction; and
Short bulbous roots that are sometimes fused with each other.1
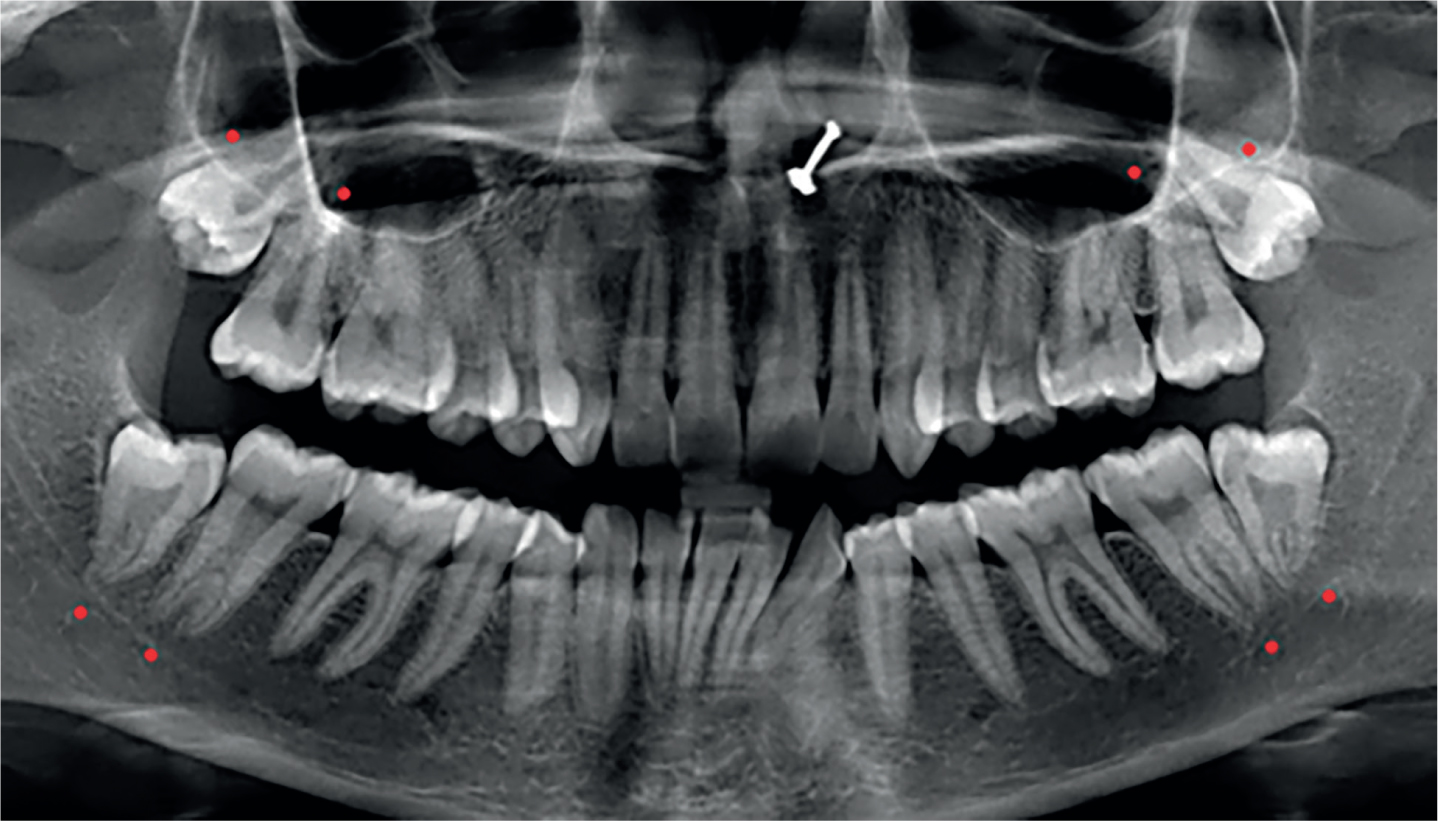
Taurodontism can occur in isolation, or in multiple teeth, unilaterally or bilaterally, in a normal population or associated with syndromes with a varying degree of severity (Figure 1).2 It is most commonly found in molars, followed by premolars and mandibular anterior teeth.3
Figure 1. A panoramic view of a female patient showing multiple taurodontism in maxillary and mandibular molars. Affected teeth (marked red): UR7, UR8, UL7, UL8, LR7, LR8, LL7 and LL8. Patient is non-syndromic.
Biomechanics of taurodontic teeth: Are there any advantages of taurodontism? Why was this anomaly common in the Neanderthals?
Recent research studied the biomechanics of taurodonts on digital models of Neanderthal specimen ‘Le Moustier 1’. This study was conducted to help understand the reasons behind high frequency of taurodontism found in Neanderthals. To evaluate this, four hypotheses were projected as possible factors responsible for taurodontism:
Biomechanical hypothesis (ie adaptation to a specific occlusal loading regimen);
Adaptation to a high attrition diet to prolong tooth longevity and to support the health of periodontal apparatus;
In this experiment, finite element analysis (FEA) and other advanced loading methods were used. The digital models of lower right first molar (RM1), along with reduced and hypertaurodontic models of RM1 of Neandertal specimen ‘Le Moustier 1’ were subjected to loading conditions. In addition, a simulated test was performed to evaluate para-masticatory efficiency of taurodontic teeth. In this test, an object was placed between teeth and pulled in various directions. The results from simulated tests did not reveal any significant biomechanical advantage of taurodontic teeth during para-masticatory function and, hence, rejected the biomechanical hypothesis. The authors of this study concluded that the high frequency of taurodontic teeth in Neanderthals most probably had evolved as an adaptive mechanism to high attrition diet routine or due to pleiotropic effects.4 It could also be a result of genetic drift and bottleneck effects, consequently elucidating the limited morphological discrepancy observed in Neanderthals.
The researchers highlighted another point relevant to modern dentistry, namely that the pulp cavity, when filled with dentine-like restorative material, enhanced tooth stiffness. This in turn had a negative impact on the dental crown as the tensile stresses were also increased, ultimately contributing towards tooth fracture.
Yet, in another study,5 scientists set out to investigate molar root morphology among Neanderthals (Middle and Late Pleistocene), Aterian (Late Pleistocene) and recent Homo sapiens.
They sought to evaluate whether root morphology can act as a differentiating feature among species, and whether variances in root morphology suggest differences in tooth functionality.
Scientists used microtomography imaging to study and quantify internal and external anatomy of specimen molars. The advanced imaging helped researchers in the evaluation of 3D root morphology. Through univariate and multivariate statistical analysis of the specimens, researchers found some similarities and differences between the teeth of Neanderthals (penecontemporaneous) and Aterian (H. sapiens):
Similarities in pulp volume and root length;
Differences such as pyramidal roots and volume of dental tissue.
On the other hand, recent H. sapiens had smaller molar proportions than Neanderthals and Pleistocene H. sapiens, but possessed reduced dental volume similar to Pleistocene H. sapiens and a smaller root to crown ratio relative to Neanderthals. In addition, the first molar's root surface area of Neanderthals and recent H. sapiens happened to be the greatest. Contrary to this, the second molar comprised the largest root surface area in Aterian H. sapiens. These differences among root surface area suggest that a distinct occlusal loading scheme was present in Neanderthals as compared to Pleistocene and recent H. sapiens.5
Studies indicate that the Neanderthals had specific biomechanical alterations in their dentition, which gave rise to their increased masticatory force generated during consumption of highly abrasive foods.6 The Neanderthals had a reduced arch length, either as a result of a posterior shift of anterior teeth coupled with an anterior shift of molars or a reduction in mesio-distal dimension of molars that placed them in a forward position. This resulted in first and second molars being placed in an ideal position for the generation of higher masticatory forces, as an adaptive mechanism to a high attrition diet.6,7
A number of studies debate in favour of selective advantage of taurodontic permanent molars. First, a large pulp cavity is thought to be an advantage among populations that consumed an attrition causing diet, since the large pulp cavity compensates for the occlusal tooth surface loss by laying secondary dentine. Secondly, a deep-seated furcation of taurodont molars secures this region from the oral environment and hence reduces the chances of periodontal disease.8,9,10-11
Diagnostic considerations
Previously, external morphological features have been used to diagnose taurodontism. However, it is difficult to rely on them alone and nowadays internal anatomical characteristics are used to diagnose this anomaly.12 The diagnosis of taurodontism is based on an evaluation of the following three aspects:
Clinical findings;
Internal morphology; and
Radiographic features.
Clinical findings
Teeth affected by taurodontism appear to be similar to normal teeth from a clinical standpoint as they have a normal crown. Since these teeth have an unusually long root trunk developed at the expense of roots, the only feature identifiable is the lack of an inter-radicular area during periodontal probing of multi-rooted teeth. This feature is not identifiable clinically in a healthy dentition unless the area is probed.13,14 Therefore, taurodontism can be stated as a developmental anomaly found by chance during radiographic assessment.15
Internal morphology and radiographic features
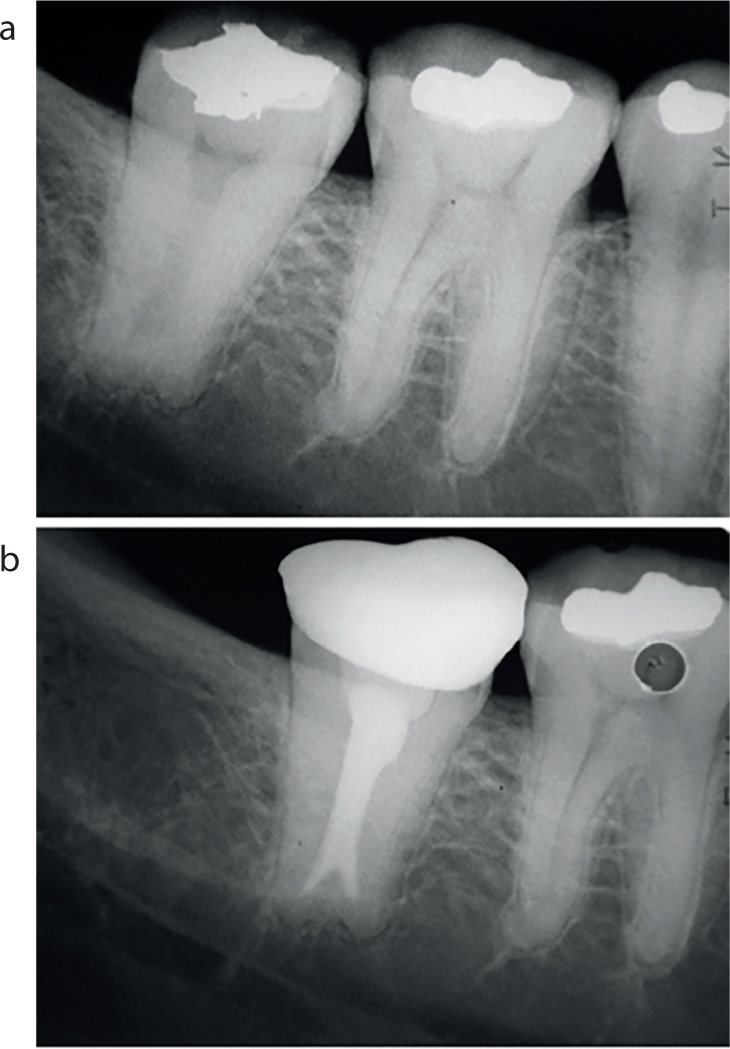
Taurodont teeth demonstrate a number of internal and radiographic features that make them dissimilar from normal teeth and, hence, an endodontic challenge. The following are the characteristics of multi-rooted taurodont teeth (Figure 2):16,17,18,19,20,21,22,23,24-25
Absent or under-developed cervical constriction at the CEJ;
Apical displacement of furcation;
Thin cervical dentine around canal orifices;
Small to absent inter-radicular area;
Short roots and root canals.
Figure 2.
(a, b) Radiographic images showing treatment of a hypertaurodontic second mandibular molar. (Courtesy of John Wiley and Sons. From Parolia A, Khosla M, Kundabala M. Endodontic management of hypo-, meso- and hypertaurodontism: case reports. Aust Endod J 2012; 38: 36–41).
Differential diagnosis
There are certain developmental disorders that mimic taurodontism, such as amelogenesis imperfecta and dentinogenesis imperfecta26 (Figures 3 and 4). Large-sized pulp cavities (characteristic of taurodontism) are also seen during the initial stages of these disorders. However, underdeveloped roots and the presence of an open apex distinguish them from taurodontism27 (Figure 5). Other metabolic disorders that also exhibit large pulp cavities are rickets, hypophosphatasia and pseudo-hypoparthyroidism (Table 1).28,29–30
Figure 3.
(a, b) Clinical and radiographic images of dentinogenesis imperfecta. Apart from characteristic features of this condition (extensive attrition and amber-yellow discoloration), large pulp cavities are evident on radiographs. (c) Large pulp cavities mimicking taurodontism during the early stage of disorder, although taurodontism can occur in association with dentinogenesis imperfecta. (Courtesy of John Wiley and Sons. From Li F, Liu Y, Liu H, Yang J, Zhang F, Feng H. Phenotype and genotype analyses in seven families with dentinogenesis imperfecta or dentine dysplasia. Oral Dis 2017; 23: 360–366).Figure 4. Vitamin D resistant rickets showing physical and dental features. (a) Physical signs: rachitic rosary (pronounced costochondral junction), short stature, stunted growth and bowed legs. (b) Dental radiographic features: periapical radiographs showing widened pulpal space of LR deciduous second molar, mimicking taurodontism. (From Choubey S, Meena D, Bafna Y, Kulkarni S, Swamy N. Diagnosis of a rare genetic disorder in the dental clinic: case report on vitamin d-resistant rickets. Int J Dent Case Reports 2013; 3: 16–19).Figure 5. Oral manifestations of vitamin D resistant rickets. (a) Clinical presentation of a child with partially edentulous maxillary arch (with only three posterior primary teeth) and edentulous mandibular arch. (b) Panoramic radiograph exhibiting hypoplastic alveolar ridges, several absent deciduous teeth, permanent molars with large pulp cavities and short roots with ill-defined lamina dura. (From Rathore R, Nalawade TM, Pateel D, Mallikarjuna R. Oral manifestations of vitamin D resistant rickets in orthopantomogram. BMJ Case Reports 2013; 2013: bcr2012008318).
Developmental Conditions
Differentiating Features from Taurodontism
Amelogenesis imperfecta
Incompletely developed roots, open apices (during initial stages of condition)
Dentinogenesis imperfecta
Metabolic Conditions
Differentiating Features from Taurodontism
Rickets
Teeth have a normal appearance and form with widened pulp cavities
Hypophosphatasia
Pseudo-hypoparthyroidism
Association with systemic syndromes
Taurodontism most frequently occurs in isolation. A polygenic inheritance has been shown to be the cause of various forms of expression and the anatomical features seen in taurodontism.31 However, it can also be seen in association with syndromes.32 Several case reports show a higher prevalence of taurodontism when associated with developmental disorders and how it affects multiple teeth in these patients (Table 2).14,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61–62
Syndromes
Key Oral Features/Manifestations
Cleft lip and palate
Ectopic eruption (primary maxillary anterior dentition), oro-antral fistulas, congenitally missing teeth, malformed and mal-rotated teeth and taurodontism, supernumerary teeth, malocclusion
Amelogenesis imperfecta
Hypoplastic or hypomaturative enamel, enamel defects, taurodontism (infrequently associated)
Hypodontia
Agenesis of permanent teeth (at least 2 and less than 6), taurodontism, diastemas and microdonts
Down's syndrome
Hypodontia (lateral incisors most commonly absent), delayed eruption, altered teeth morphology such as peg laterals, taurodontism, periodontal disease; mainly due to impaired host response, and lower incidence of caries (due to high salivary IgA concentrations directed towards Streptococcus mutans)
Klinefelter syndrome
Periodontal disease, taurodontism, high caries rate, prognathism and reduced facial height
As the name indicates, it affects lacrimal system, ears, dentition and fingers. Oral features: xerostomia, high caries rate, peg-shaped incisors and microdontia, enamel hypoplasia, taurodontism and malformed molars
Cleft lip (common), cleft lip and palate, or only cleft palate, hypernasal voice, bifid uvula, fusion of teeth, taurodontism, hypodontia (mainly premolars), ankyloglossia, syngnathia and high-arched palate
Smith-Magenis syndrome
Hypodontia (commonly premolars), taurodontism, high caries rate, root dilacerations
Hypohidrotic ectodermal dysplasia
Hypodontia, hypohidrosis, hypotrichosis, xerostomia, dysphagia, congenitally missing and malformed teeth, moderate to severe taurodontism, crown/root dysmorphism, microdontia, conical crowns and weak enamel.
Oligodontia
Agenesis of more than 6 teeth, presence of taurodontic molars, reduced dimensions of teeth
Sex chromosomal abnormalities
Taurodontism
Thalassemia major
Absent or faint inferior alveolar nerve canal and thin mandibular cortex, taurodonts, spiky-short roots, diminished lamina dura
McCune-Albright syndrome
Taurodontic teeth, high caries rate, malocclusion, rotated teeth. Generalized spacing between teeth may be present due to expansion of fibro-osseous lesions
Underdeveloped maxilla and mandible, impacted teeth, generalized periodontal disease coupled with extensive bone loss, taurodontism
Wolf-Hirschhorn syndrome (4p-syndrome)
Cleft lip and palate common, taurodontism, agenesis of multiple permanent teeth (mainly premolars and molars), and over-retained primary teeth
Nevertheless, a few case reports have shown multiple taurodontism without syndromes.20,63 The following are the developmental disorders in which taurodonts are frequently seen:
For syndromic patients presenting with taurodontism, it is imperative to constitute a team of professionals and have a holistic approach for their management.
Conventional radiography vs CBCT
Periapical and panoramic radiographs have long been used as the method of choice for both identification and biometric evaluation of taurodontism. However, these radiographs have an inherent problem of providing a limited 2D view20 and, hence, can only assist in formulating initial diagnosis. Other drawbacks of conventional radiography include image foreshortening or elongation, distortion, overlapping, magnification and non-reproducibility. Whereas in panoramic radiographs there is frequently lack of definition, superimposition of structures, teeth appearing rotated (especially premolars) and images sometimes having motion blur due to movement of patient.63,64-65
Therefore, conventional radiography should be used for initial assessment only and a detailed view of taurodonts should be obtained with cone beam computed tomography (CBCT). On evaluating the CBCT image of a hyperdont, special attention should be given to the thickness of the pulpal floor adjacent to root canal orifices, and the number of root canals should also be noted. Furthermore, canal curvatures (especially in bucco-lingual direction) can also be identified through the CBCT image.
While there are not many studies advocating CBCT use for managing taurodonts, in the author's opinion it may be worthwhile for the clinician to obtain a pre-operative CBCT image, especially for hyperdonts. This will aid in the prevention of accidental events, such as perforations in cervical regions and missed root canals. However, it is prudent to adhere to ALARA guidelines and unwarranted use of radiation should be avoided, such as in cases of mild to moderate taurodontism.
Clinical management
Taurodontism mainly affects molar teeth, in both permanent and deciduous dentitions, the former being more common. It has three classes; mild, moderate and severe, based on the degree of apical displacement of the pulpal floor.
When it comes to the management of taurodonts, it may not be much different from normal teeth requiring endodontic treatment. The challenge is to manage the severe form of cases, such as hyperdont molars that show most morphologic deviations of a root canal system, thus influencing endodontic treatment. However, taurodonts can also have clinical implications in prosthodontics, extractions, intentional implantation, orthodontics and periodontics (Table 3).
Clinical Parameters
Concerns/Reasons
Endodontic
Excessive bleeding upon access
Can mislead clinician to see excessive bleeding as perforation
High volume of pulp tissue
Along with mechanical excavation, a high volume and concentration of irrigant may be needed to disintegrate extra pulpal tissue
Irrigation and preparation
Complex morphology may need ultrasonic irrigation
Vertically enlarged pulp chambers and apically displaced furcation
Difficult visualization of the pulpal floor and instrumentation of root canals
It is difficult to confirm in hyperdonts. CBCT and magnification recommended
Obturation
Multiple apical channels can be present, such as in hyperdonts, therefore it is important to seal all and avoid material extrusion. Alternatively, vital pulpotomy can be performed with root canal pulp left intact.
Post placement is discouraged
Short roots and thin cervical region around orifices increase chances of perforation.
Periodontic
Periodontally stable
A long root trunk (especially in hyperdonts) makes furcation lie well below the crest of alveolar bone and less susceptible to bacterial intrusion
Prosthodontic
May not be an ideal prosthetic abutment
Lack of long and divergent roots
Surgical
Extraction is less complicated
Lack of long and divergent roots
Intentional replantation could be a problem
Taurodonts have a bulbous apical area that may pose a problem
Orthodontic
May not be suitable for anchorage
Lack of long and divergent roots
Endodontic management
The anatomical challenges encountered during endodontic treatment are profuse bleeding upon access, difficult visualization of deep pulp cavity and identification of orifices, unpredictable disinfection of complex pulp-radicular system, mechanical preparation of thin cervical areas, short roots and their obturation. Other complications include high chances of perforation, accidental extrusion of irrigant or obturant from short roots, and increased stiffness of a tooth upon filling the large pulp cavity with dentine-like restorative material.4
Vital pulpotomy
In the case of irreversible pulpitis, ordinary root canal treatment is indicated. For complex cases such as hyperdonts, where the pulp cavity extends up to the apex and divides into several portals of exit, the recommended treatment is vital pulpotomy.15,66 However, if periapical pathology is evident then pulpectomy becomes necessary.
Excessive bleeding upon access
A vertically elongated pulpal cavity harbours extra pulpal tissue. Once inflamed, this excess tissue causes profuse bleeding during extirpation and is often difficult to control, raising a false alarm of perforation to the clinician. After coronal pulp extirpation, bleeding usually subsides and instrumentation of apically positioned orifices becomes practical.
Irrigation and preparation
With the advent of modern irrigation systems, such as ultrasonics and water lasers, it would be both effective and time saving to use root canal disinfection in taurodontism. A higher concentration and temperature of sodium hypochlorite (NaOCl) will rapidly disintegrate excess pulpal tissue. This higher concentration might also be useful for disinfecting thin cervical regions, where instrumentation carries a risk of perforation.
Deep-seated orifices
Reaching root canal orifices will require complete removal of coronal pulpal tissue. Owing to the long pulp cavity and apically displaced furcation, the root canals are deep-seated, making them difficult to identify and manipulate with instruments. To accomplish this task, prior knowledge of the anatomy, use of magnification aid and a good skill set are necessary.
Root canal configuration (number, shape, location and negotiation)
Taurodonts demonstrate a wide variation of root canal anatomy such as apically positioned root canals, their number, configuration, and the likelihood of accessory root canals. While instrumenting the short roots, a precise control of working length is essential to prevent extrusion of the gutta-percha. To achieve this, it is best to use a combination approach that involves radiographic estimation, an electronic apex locator, a paper-point test and, finally, a dry-run gutta-percha radiograph. Depending on the severity of taurodontism, each case brings its own unique challenges and may require advanced tools, such as cone beam computed tomography and a dental operating microscope.
Obturation
Root canals in taurodontism can either be short or present in the form of multiple channels exiting from an elongated root trunk, as seen in hypertaurodontism. Obturation in such cases is a challenge and could be carried out by providing an initial apical cork of gutta-percha followed by a back-fill with thermoplasticized gutta-percha (continuous wave compaction). This will completely fill irregularities of the long rectangular pulp chamber of hyperdonts (which extend well below the crest of alveolar bone).
Post-space preparation
Posts can be placed but with caution, especially in hyperdonts. Because these teeth have thin cervical dentine around the orifices, a deep-seated furcal floor and short roots, Tsesis et al have advised against post-placement for reconstruction.24
Restoration of endodontically treated tooth
In taurodonts with reduced crown height (eg due to attrition), or where a post is contra-indicated, a bonded restoration can be used as a core build-up and small tags can be placed inside the canal orifices to improve retention. However, Benazzi et al found that the filling of the entire pulp cavity of taurodonts with dentine-like restorative material increased their stiffness. He suggested that this could contribute towards tooth fracture, as high stiffness increased tensile forces in the crown.4 Additional measures for cases with reduced crown height or limited ferrule include orthodontic extrusion or crown lengthening surgery.
Periodontic management
Overdeveloped root trunk
An elongated root trunk and a below the alveolar crest inter-radicular region might protect a tooth from the oral environment, hence assisting in the prevention of periodontal disease. Moreover, these teeth do not have external surface aberrations and possess a normal anatomical crown.
Reduced surface area of roots
In contrast, short and less diverged roots reduce the surface area of taurodonts, thereby decreasing contact with bone. Hence, this may have a negative impact on the stability of taurodonts within the alveolar socket.
Prosthodontic management
Crown preparation
Due to lack of cervical constriction and a reduced cervical bulge, it might be easier and relatively conservative to perform crown preparation on these teeth.
Prosthetic abutment
Short roots provide a reduced surface area and limited anchorage into the alveolus as compared to long and divergent roots of a normal tooth. Therefore, a hyperdont might not be a suitable abutment for fixed bridge prosthesis.67 The author was unable to find significant data on this hypothesis, therefore, this needs to be confirmed through suitable research.
Surgical management
Intentional replantation
Mesodonts and hyperdonts have a bulbous apical area, which may complicate extraction, resulting in damage to the apical region that is critical to the success of the procedure. Therefore, intentional replantation could pose a challenge and should be done with careful planning.
Extraction
Extraction is less complicated due to an elongated body and short coalesced roots. This is because a long root trunk with shortened roots reduces the firmness of the tooth within the socket.
Orthodontic management
From an orthodontic standpoint, these teeth are not ideal for anchorage purposes due to the lack of long divergent roots that provide strength and reliability.67
Prognosis
The author was unable to find failed endodontic cases of taurodonts in the literature. Therefore, it could be opined that taurodonts do not have an increased failure rate after endodontic treatment as compared to normal teeth after treatment, providing that they are carefully managed. Taurodonts might be, to a certain extent, more resistant to occlusal attrition and pulpal exposure (owing to their large-sized pulp cavity and resultant enhanced ability to lay secondary dentine), as depicted in Neanderthals who consumed a high attrition diet and typically showed taurodontism.
Nevertheless, these hypotheses should be substantiated through appropriate studies. In contrast, these teeth offer more resistance from periodontal disease entering the furcal region because of their long root trunk seated within the alveolar bone.
Summary
This article reviewed the biomechanics of taurodontic teeth and discussed various factors that may influence the functionality of these teeth. The clinician also needs to be heedful of the developmental disorders that could mimic taurodontism, and look out for key distinguishing features prerequisite to formulating a differential diagnosis. Furthermore, multiple taurodontism sometimes occurs in association with syndromes and, perhaps, may assist in early diagnosis.
The author advocates the use of cone beam computed radiography (in addition to radiographs) for handling difficult cases. In such cases, the teeth may take a rectangular or cylindrical shape and can complicate endodontic treatment.