Ziuchkovski JP, Fields HW, Johnston W, Lindsey D. Assessment of perceived orthodontic appliance attractiveness. Am J Orthod Dentofacial Orthop. 2008; 133:S68-78
Phan X, Ling PH. Clinical limitations of Invisalign. J Can Dent Assoc. 2007; 73:263-266
Djeu G, Shelton C, Maganzini A. Outcome assessment of Invisalign and traditional orthodontic treatment compared with the American Board of Orthodontics objective grading system. Am J Orthod Dentofacial Orthop. 2005; 128:292-298
Kravitz ND, Kusnoto B, BeGole E, Obrez A, Agran B. How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Am J Orthod Dentofacial Orthop. 2009; 135:27-35
Chatoo A. A view from behind: a history of lingual orthodontics. J Orthod. 2013; 40:S2-7
Fujita K. New orthodontic treatment with lingual bracket and mushroom archwire appliance. Am J Orthod. 1979; 76:657-675
Fujita K. Multilingual bracket and mushroom archwire technique: a clinical report. Am J Orthod. 1982; 82:120-140
Kurz C, Romano R. Lingual orthodontics: historical perspective. In: Romano R (ed). Hamilton, Ont: BC Decker; 1998
Wiechmann D. A new bracket system for lingual orthodontic treatment. Part I: Theoretical background and development. J Orofacial Orthop. 2002; 63:234-245
Wiechmann D. A new bracket system for lingual orthodontic treatment. Part II: First clinical experience and further development. J Orofacial Orthop. 2003; 64:372-388
Singh P, Cox S. Lingual orthodontics: an overview. Dent Update. 2011; 38:390-395
Fillion D. Lingual straightwire treatment with the Orapix System. J Clin Orthod. 2011; 45:488-497
Øgaard B, Rølla G, Arends J. Orthodontic appliances and enamel demineralization. Part 1. Lesion development. Am J Orthod Dentofacial Orthop. 1988; 94:68-73
Caniklioglu C, Oztürk Y. Patient discomfort: a comparison between lingual and labial fixed appliances. Angle Orthod. 2005; 75:86-91
Sinclair PM, Cannito MF, Goates LJ, Solomas LF, Alexander CM. Patient responses to lingual appliances. J Clin Orthod. 1986; 20:396-404
van der Veen MH, Attin R, Schwestka-Polly R, Wiechmann D. Caries outcomes after orthodontic treatment with fixed appliances: do lingual brackets make a difference?. Eur J Oral Sci. 2010; 118:298-303
Auluck A. Lingual orthodontic treatment: what is the current evidence base?. J Orthod. 2013; 40:dS27-33
Wu AK, McGrath CP, Wong RW, Rabie AB, Wiechmann D. A comparison of pain experienced by patients treated with labial and lingual appliances. Ann R Australas Coll Dent Surg. 2008; 19:176-178
Wiechmann D, Gerss J, Stamm T, Hohoff A. Prediction of oral discomfort and dysfunction in lingual orthodontics: a preliminary report. Am J Orthod Dentofacial Orthop. 2008; 133:359-364
Hohoff A, Seifert E, Fillion D, Stamm T, Heinecke A, Ehmer U. Speech performance in lingual orthodontic patients measured by sonography and auditive analysis. Am J Orthod Dentofacial Orthop. 2003; 123:146-152
Hohoff A, Stamm T, Goder G, Sauerland C, Ehmer U, Seifert E. Comparison of 3 bonded lingual appliances by auditive analysis and subjective assessment. Am J Orthod Dentofacial Orthop. 2003; 124:737-745
Khattab T, Farah H, Al-Sabbagh R, Hajeer M, Haj-Hamed Y. Speech performance and oral impairments with lingual and labial orthodontic appliances in the first stage of fixed treatment – a randomised control trial. Angle Orthod. 2013; 83:516-526
Gorman JC, Hilgers JJ, Smith JR. Lingual orthodontics: a status report. J Clin Orthod. 1983; 17:26-35
Mavreas D, Athanasiou AE. Factors affecting the duration of orthodontic treatment: a systematic review. Euro J Orthod. 2008; 30:386-395
Ling PH. Lingual orthodontics: history, misconceptions and clarification. J Can Dent Assoc. 2005; 71:99-102
Knosel M, Klang E, Helms HJ, Weichman D. Lingual orthodontic treatment duration: performance of two different completely customized multi-bracket appliances (Incognito and WIN) in groups with different treatment complexities. Head Face Med. 2014; 10
Cooper-Kazaz R, Ivgi I, Canetti L The impact of personality on adult patients' adjustability to orthodontic appliances. Angle Orthod. 2013; 83:76-82
Grauer D, Proffit WR. Accuracy in tooth positioning with a fully customised lingual orthodontic appliance. Am J Orthod Dentofacial Orthop. 2011; 140:433-443
The demand for adult orthodontic treatment is an ever-increasing trend that has driven the development of aesthetic orthodontic systems. Lingual orthodontic appliances provide the ultimate in aesthetics and their use has grown with the development of the appliances. The clinical application of different lingual appliances is described and evidence-based patient information is provided.
CPD/Clinical Relevance: Increasing demand for aesthetic orthodontic systems means that lingual appliances are, and are likely to become, more popular in the future. A broad knowledge of their clinical application and useful evidence-based information to give to patients is invaluable for all dental practitioners.
Article
The demand for adult orthodontic treatment is an ever-increasing trend that has driven the development of aesthetic orthodontic systems. A recent survey of British Orthodontic Society members working in high street practices found that 75%, of 430 respondents, reported an increase in adult treatment.1 Assessments of attractiveness and acceptability associated with orthodontic appliances have shown that a significant number of adults requiring treatment refuse it on the basis of the negative appearance associated with many commonly used appliances.2 A study looking at the attractiveness of different orthodontic appliances found both lingual and ‘clear tray’ (aligner) appliances to be rated as significantly more attractive than labial ceramic appliances, which were in turn rated as significantly more attractive than labial metal appliances.3 It was also no surprise to find that, in the hierarchy of attractiveness, lingual appliances were more attractive than ‘clear tray’ aligner appliances.3 The most popular clear aligner system currently on the market is Invisalign (Align Technology Inc, San Jose, USA), which has widespread use in both the specialist and non-specialist community. However, its well-documented clinical limitations,4-6 coupled with its reduced attractiveness, has led many clinicians to develop their use of lingual appliances.
The aim of this article is to give an update of the current clinical applications of lingual orthodontic appliances and, through a review of the evidence, provide advice that can be given to patients considering treatment.
Evolution of lingual appliances
The development of lingual appliances started in 1968 at Kanagawa University, Japan, when Kinya Fujita first submitted his lingual appliance concepts.7 He started the manufacture and use of his system in 19758 and reported on various extraction cases, successfully treated, in 1979.8 An interesting quote from him that is still relevant today was that, despite the patients experiencing discomfort, disturbance to speech and increased treatment time, none of them opted to have their appliances removed for conventional brackets to be placed.9 Around a similar time, Craven Kurz, of UCLA School of Dentistry, USA, was convinced that a lingual-bonded, edgewise appliance was feasible and, in collaboration with the Ormco company, developed their first prototype in 1979.10 The difficulties faced by Dr Kurz and his team were bond failures, patient discomfort and archwire ligation. The Ormco Lingual Task Force was set up in 1980 with a remit to try and address these problems. The development of indirect bonding and modification of the size, shape and profile of the brackets led to the production of the seventh generation Ormco bracket in 1990. The small size of this bracket resulted in an increase inter-bracket span that solved many biomechanical issues with the early brackets. Put simply, efficient tooth movement was possible and, as a consequence, this bracket stayed in favour until 2004.7 It was at this time that a further breakthrough was made with the introduction of the smaller STb (Ormco: Sybron Dental Specialties) bracket by Dr Giuseppe Scuzzo and Dr Kyoto Takemoto. It facilitated the use of light forces with reduced friction and aimed to overcome issues with speech, patient comfort and oral hygiene. A sizeable issue, however, with all the systems at this time was their ability to control teeth in three dimensions, which to an extent limited their clinical application. The person to propel lingual appliances into the mainstream of orthodontics was Dr Dirk Weichman when he used CAD CAM technology to manufacture the first fully customized system (Incognito-3M Unitek, Monrovia, CA, USA) where the bracket bases were perfectly contoured to the individual lingual surfaces of the teeth.11,12 Coupled with the use of robotically bent individualized wires, this system allows the three-dimensional control of individual teeth to produce accuracy and precision in treatment.
Differences to labial appliances
Apart from the glaringly obvious, there are some specific challenges that come with lingual appliances. The lingual morphology of teeth, especially the maxillary incisors, can be unique and irregular, which can make the placement of brackets in ideal positions difficult.13 A non-customized lingual bracket will often not fit flush to the bonding surface of the tooth, leading to reduced bond strength and first order (‘in-out’) inaccuracies. The other, quite sizeable problem, is the differing bucco-lingual thickness of teeth, which once more results in first order problems during treatment. This can be either overcome by the use of multiple finishing bends in the final wire, a fully customized system (preformed wires and brackets), or differing bracket widths, as seen in the lingual ‘straight wire’ system (Orapix Co Ltd, South Korea).14
The nature of the position of lingual appliances means that archwires are often compressed, which leads to a tendency to push, flare, expand and reduce the overbite. This needs to be taken into consideration when choosing the correct appliance system for a patient.
Benefits of lingual appliances
As previously stated,2 lingual appliances have been rated the most attractive of all appliances. This has the benefit of attracting a proportion of patients who would otherwise avoid treatment with conventional appliances. The ability to continue with professional lives unhindered by the aesthetic impact of the appliance itself can be extremely important to some people.
During any orthodontic treatment, the maintenance of excellent oral hygiene to prevent negative periodontal effects and caries is imperative.15 The achievement of satisfactory oral hygiene has been shown not to differ in both labial and lingual appliances.16,17 However, one randomized, controlled, split-mouth study18 showed that buccal surfaces were almost five times more likely to decay than lingual surfaces. Although split-mouth design studies will always have an element of bias, this RCT18 represents the best evidence in this area. The study utilized fully customized lingual appliances that have a bracket base that covers most of the tooth, and so there will have been a bracket base size protective element, meaning that this data should be projected to other forms of lingual appliance with caution. It is rare, if patient selection is appropriate, to get frank cavitation during orthodontic treatment, and it is more likely to see white/brown spot lesions. Although the occurrence of these lesions is always suboptimal, from an aesthetic perspective, the impact is much reduced on the lingual surface compared to the labial, and is less likely to happen as the lingual surfaces of the teeth are more self cleansing, given the action of the tongue and salivary flow. In a review of the evidence base for lingual appliances, it was stated that maintenance of low plaque levels is equally important during lingual and labial appliance therapy in order to maximize periodontal health.19 The research in this field is currently limited, but there does not seem to be an advantage or disadvantage where periodontal health is concerned.
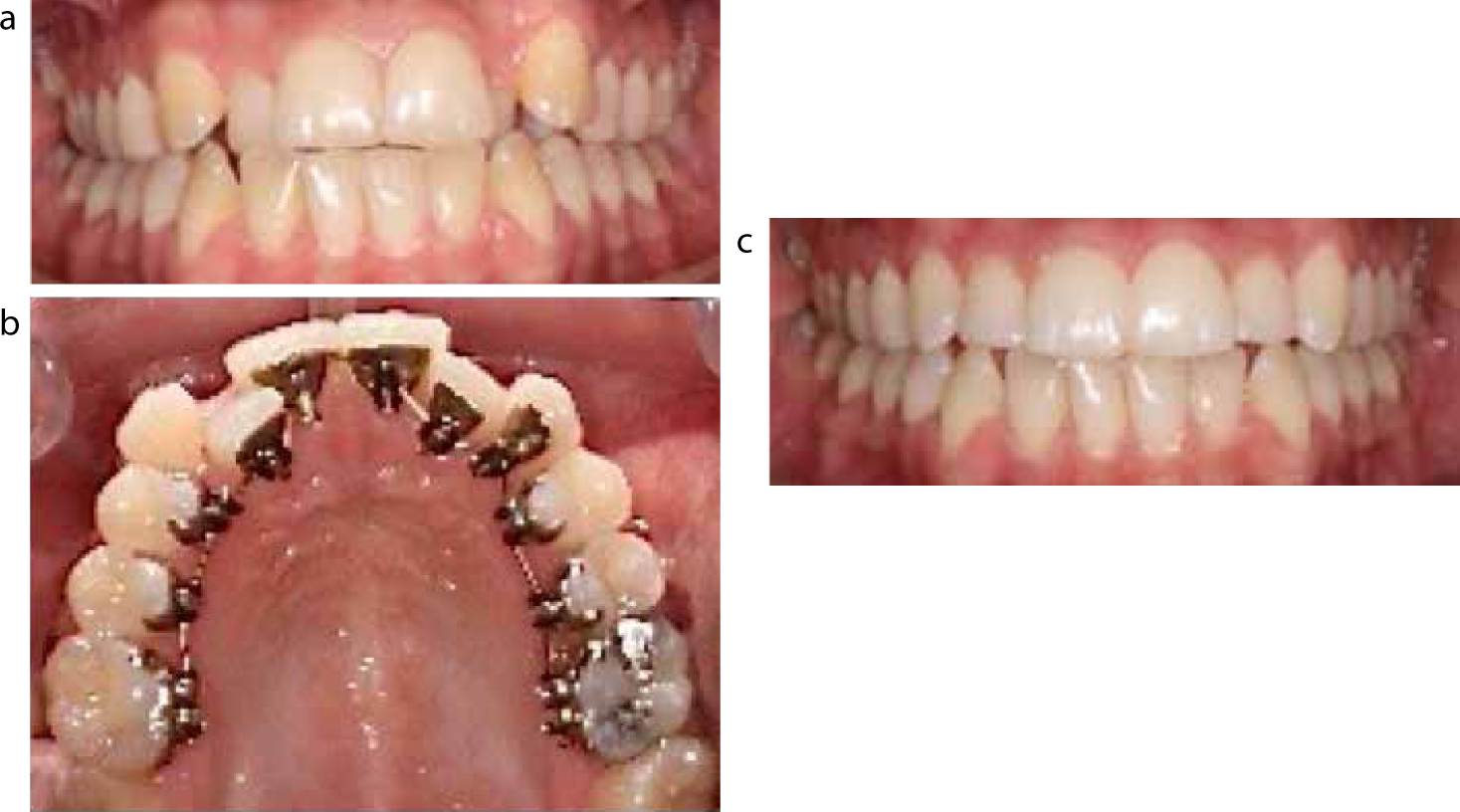
There are mechanical advantages when it comes to the use of lingual appliances, in their ability to reduce overbites due to their bite plane effect. Conversely, the maintenance of overbite can be achieved with fully customized appliances, due to their ability to express anterior lingual crown torque (Figure 1). This is partly due to the orthodontic forces being applied lingual to the centre of rotation of the tooth, but also because the vertical placement of the archwire in the anterior region means torque is expressed efficiently.
Figure 1.
(a) Start of treatment: the patient requested upper only treatment. (b) Upper Incognito (3M-Unitek, Top-Service für Lingualtechnik, Bad Essen, Germany) appliance. (c) Completion of treatment showing torque control of the upper incisors and maintenance of a functional overbite.
Another, more straightforward, advantage to the clinician is that, during the finishing stage of treatment, viewing the labial surfaces of the teeth is much easier than when labial appliances are in situ and so fine detailing can be achieved. There is also a patient-centred aspect to this, as they can clearly see where the final position of the teeth will be rather than ‘looking through the appliance’ to imagine where the teeth will be positioned. It may also be that a patient wishes to complete a course of orthodontic treatment prior to a specific event, such as a wedding. If the timescale before the event is shorter than the treatment is expected to take, then the patient has the option of starting the treatment knowing that, when the event arrives, there will be an improvement, but with the knowledge that the treatment can continue efficiently without the need to remove the appliance for aesthetic reasons.
Risks of lingual appliances
Discomfort from orthodontic appliances is well recognized,20 but the important question to consider is whether pain and discomfort from lingual appliances differs from that due to labial appliances. Studies16,20 attempting to address this question found that pain immediately after the placement of appliances was broadly similar and slowly disappeared after a one-month period. It was found, however, that tongue soreness was higher17 in patients with lingual appliances which, considering the encroachment on the tongue space, comes as no surprise. A further study21 looked at the impact of malocclusion on oral discomfort in patients wearing fully customized lingual appliances. Those patients with jaw retrognathia were more prone to experiencing oral discomfort. The clinician must be mindful of this, along with other factors, when considering a patient's suitability for treatment.
The effect on speech of lingual appliances is something that the clinician always needs to incorporate into any informed consent. During the length of the treatment, the articulation zone behind the incisors is altered, leading to a change in certain sounds and, in particular, ‘s’ sounds. Sonographic studies22,23 have shown that a true deterioration in articulation can occur up to three months after the placement of any lingual appliance, although this effect is less when lower profile customized brackets are compared to prefabricated brackets. All orthodontic appliances can lead to difficulties when eating, however, an RCT24 comparing oral impairments between labial and lingual appliances found more significant masticatory problems with lingual appliances immediately after placement. The same study found that, in patients with lingual appliances, there was still an absence of normal masticatory function at four weeks. The use of customized lingual brackets resulted in less oral discomfort during mastication when compared to other lingual appliances.21
Patients should expect that each routine appointment should take longer for lingual appliances than labial appliances25 due to the impaired visualization for the clinician and small working environment. It is likely that, with experience, the clinician's operative speed will increase. Although the overall duration of orthodontic treatment is related to many factors,26 there is no objective evidence27 that lingual appliance treatment takes longer, and a recent study comparing two different fully customized lingual appliances28 compares favourably with treatment times reported from conventional appliances.
The cost of a lingual appliance is greater than a labial appliance and is related mainly to the increased chairside time and also, if using fully customized appliances, to the laboratory cost. Prices will vary based on the individual clinician and practice location, the difficulty and potential length of the treatment, whether the treatment is single arch versus double, and if a fully customized appliance is being used.
What information should you give your patient?
It would always be beneficial for a clinician to give patient information that is based on high quality evidence. The reality is that, in many fields, there is still further evidence required to ensure that patient information is as accurate as possible. The field of lingual orthodontics is no different. Table 1 presents information that can be passed to the patient by any referring practitioner or clinician completing the treatment, and is based on the best available evidence and clinical experience where the evidence is non-existent.
Subject
Patient information
Appearance of the appliance
In day-to-day function your appliance will not be seen. Towards the end of treatment you may need to wear elastics between the upper and lower teeth and these may have to be attached to a small tooth-coloured button on the outside of your teeth.
Time to complete treatment
This will depend on the individual tooth movement required but it should not take longer than a labial appliance.
Time for appointments
You can expect that your appointments will take longer than for a conventional appliance. Depending on the experience of your clinician a normal review appointment will be around half an hour.
Quality of the result
With the advances in lingual treatment and appropriate appliance selection, the quality of the result will be comparable to labial treatment.
Discomfort
In addition to the discomfort experienced by all orthodontic patients, your lingual appliance is likely to give some increase in tongue soreness. Your discomfort will slowly disappear over one month.
Risks to teeth and gingival tissues
Good oral hygiene and a non-cariogenic diet are equally important during lingual and labial treatment to prevent harmful effects. Decalcification is more likely with labial appliances and, if it occurs with lingual appliances, the aesthetic impact is minimal.
Speech
Your speech will be affected after the appliance is placed and will particularly affect ‘s’ sounds. This will improve in most people in the first week but small changes may last up to 3 months, but could be there throughout treatment.
Cost
It is highly likely that this will be higher than labial treatment but will depend on the type of lingual appliance used and the treatment required
Patient selection and treatment planning
As with all orthodontic treatment, a thorough assessment of a patient's expectations, a medical and dental history and extra-oral and intra-oral examination all come before a diagnosis of the malocclusion. Treatment planning for lingual orthodontic treatment is no different, although there are some specific considerations that need to be taken into account to maximize success.
A study29 has looked at the personality traits and psychological features of adults and if this affects appliance selection and adaptability. It was found that patients with somatization symptoms (distress arising from the perception of bodily dysfunction) and obsessive-compulsive traits (unwanted thoughts, impulses or reactions that are unremitting and irresistible) were those that favoured lingual appliances as their first choice. Both of these traits are common with anxiety and so the clinician must be aware at the outset that patients interested in lingual treatment may have to be carefully managed. With treatments commonly lasting between 1–2 years, a patient's ability to adapt and cope with treatment should always be considered.
If a patient has a degree of retrognathia then this is a good predictor for increased oral discomfort,21 and so the clinician must discuss this with the patient at the informed consent stage of treatment. If this is also coupled with retroclined lower incisors and decreased tongue space, then it may be prudent for the clinician to opt for labial lower appliances. The placement of lingual appliances in retroclined lower anterior teeth may also be technically challenging in addition to the likely increase in tongue discomfort.
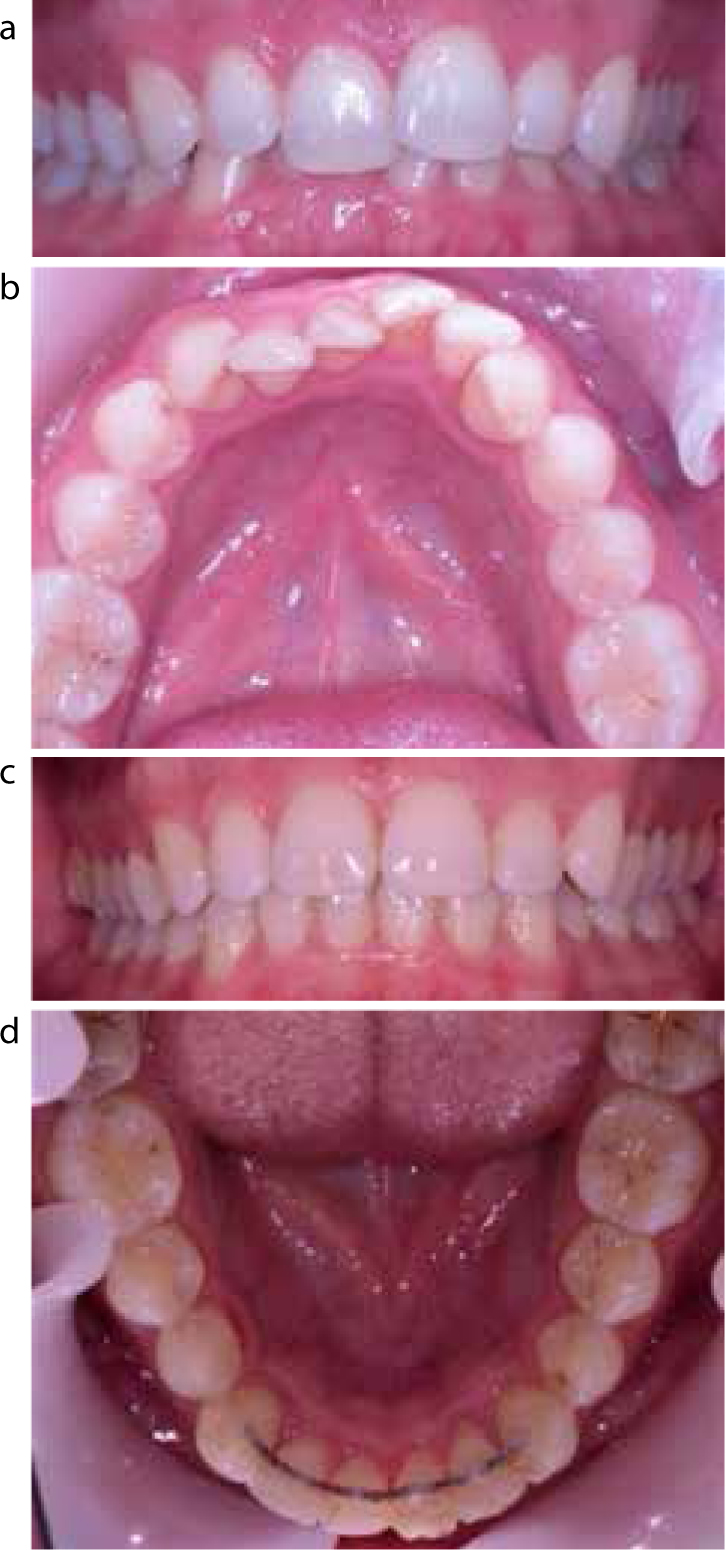
A patient's malocclusion must be looked at in detail when considering the suitability of lingual appliances from a mechanical perspective. All lingual appliances have a tendency to expand, flare and reduce overbites that can be beneficial in deep bite cases (Figure 2), but not when an already minimal overbite needs to be maintained. The real skill to success with treatment is knowing what your selected appliance can achieve. Lingual appliances fall into two broad categories:
‘2-D type’ pre-fabricated appliances that have a limited ability to provide torque to the tooth root;
‘3-D type’ fully customized appliances that have the ability to control teeth in all dimensions.
Figure 2.
(a) Start of treatment: a patient treated with upper and lower 2-D lingual appliances. (b) Start of treatment. A patient treated with upper and lower 2-D lingual appliances. (c) Completion of treatment. Showing the benefits of proclination to treat the Class II division 2 malocclusion. (d) Completion of treatment: proclination of the lower incisors and bonded retainer is shown.
Malocclusions that require limited ‘root torque’ in order to obtain a satisfactory finished result would be suitable to be treated by both types of appliance, whereas malocclusions that require a degree of root control (extractions) would not.
‘2-D type’ lingual appliances
These types of appliances are pre-fabricated and, in order to maximize success, must only be used where limited control of the tooth root is required. Examples of these types of appliances include 2-D (Forestadent, Pforzhiem, Germany – Figure 3) and the self-ligating bracket Innovation–L (GAC, Birmingham, USA – Figure 4). Figure 2 shows a successful case treated with 2-D brackets. The reason for success in the case shown was because proclination and arch expansion was desirable to obtain the treatment goals.
Figure 3. 2-D lingual appliance.Figure 4. Innovation-L self-ligating appliance. A rectangular archwire is shown with multiple finishing bends and labial buttons to enable inter-arch finishing elastics.
The archwires used with these appliances are either pre-formed or individually formed by the clinician. Rectangular archwires can be used in an attempt to impart some root control, although variable distances between the point of force application and centre of tooth rotation, the inability to hold the wire in the bracket slot and the horizontal insertion of the wire mean that the ‘torqueing’ effects are limited. The lack of individuality in both the brackets and the wires means that time consuming finishing bends are often required.
The main advantage of these types of appliances is their ability to keep costs down, which can be passed to the patient as there are no third party laboratory costs involved and any fractured component of the appliances can be replaced from the clinician's armamentarium.
’3-D type’ fully customized lingual appliances
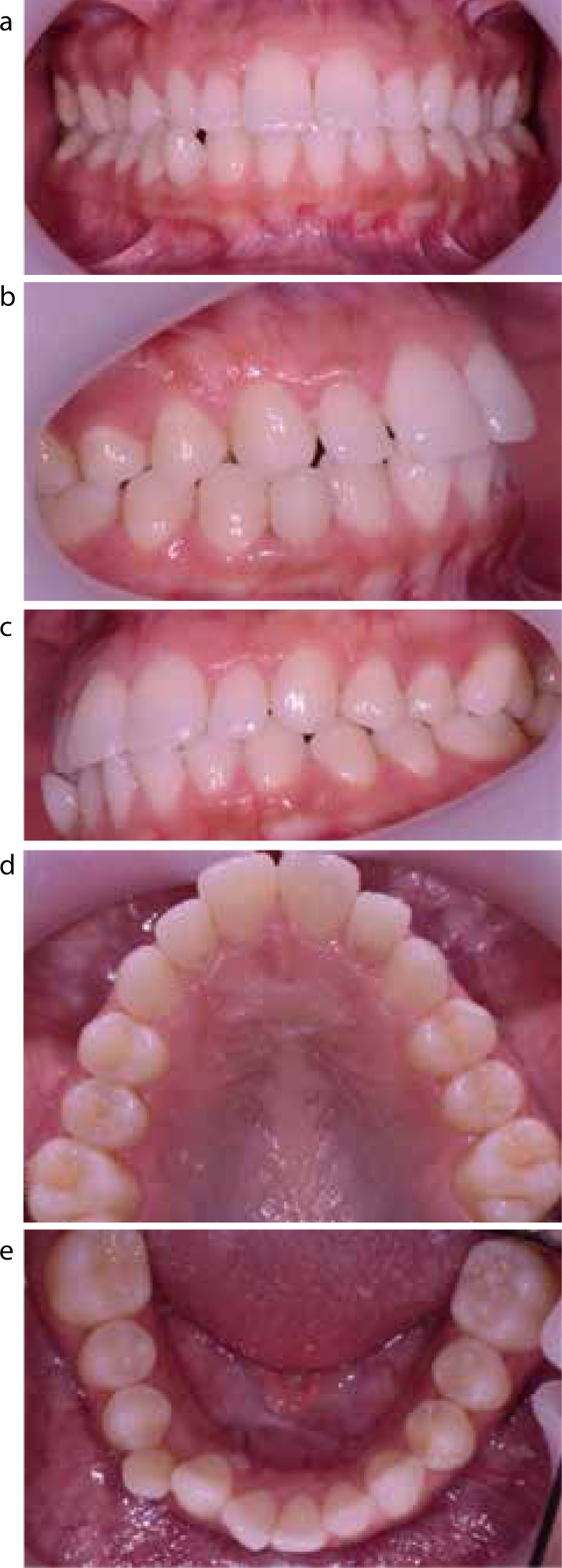
An example of a case treated with one of these types of appliances is shown in Figures 5, 6 and 7. Commonly used examples include Incognito (3M-Unitek, Top-Service für Lingualtechnik, Bad Essen, Germany – Figure 6), Win (DW LingualSystems, Bad Essen, Germany – Figure 8) and the self-ligating system Harmony (American Orthodontics, Sheboygan, USA – Figure 9). Subjective differences in oral comfort, speech, mastication and oral hygiene have been investigated between patients with pre-fabricated and customized lingual appliances. Although all patients experienced discomfort and functional difficulties, these were present to a lesser extent in the customized appliance group.21
Figure 5.
(a–e) Start of treatment: note the developmentally missing lower incisor. The patient had extraction of LRC together with upper and lower Incognito appliances.Figure 6.
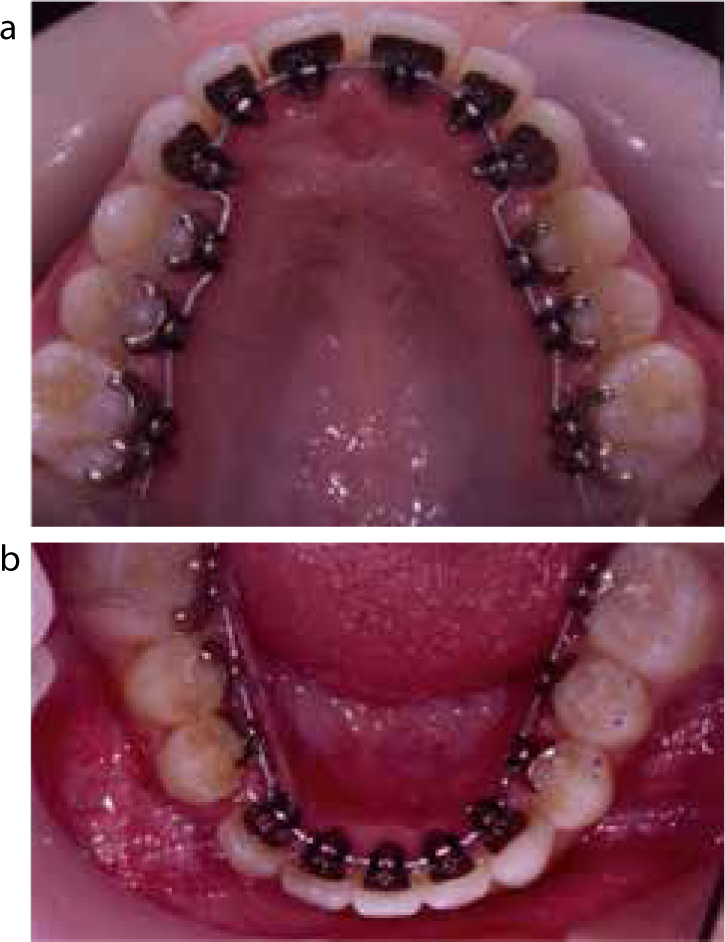
(a) Upper Incognito appliance towards the end of treatment. (b) Lower Incognito appliance showing space closure of LRC space illustrating ‘tip control’ of LR4 and LR3.Figure 7.
(a–e) Completion of upper and lower Incognito treatment.Figure 8. Win appliance.Figure 9. Harmony self-ligating appliance.
Individualized brackets mean that the bonding area can be increased which, in turn, increases the bond strength and can minimize bond failures.19 The problems associated with finishing have also been addressed by more accurate bracket positioning, archwire fabrication and a reduction in torque play between bracket slot and archwire.19 Planned and final tooth position have been studied using computer software to look at the accuracy of fully customized lingual treatment. The appliance was accurate at achieving most of the planned goals at the initial set-up, apart from the full amount of expansion and inclination of the second molars.30
The control given to the clinician with this type of appliance means that, within the caveats already mentioned in this article, all types of malocclusion may be treated. The main drawback with this type of appliance, however, is the manufacturing cost which leads to a proportion of patients being excluded from using the appliance on cost grounds. The relatively recent introduction of the Win appliance has looked to address some of the cost issues and is growing in popularity.
Conclusion
This article illustrates the development of lingual appliances into two broad types that are now being used. To maximize success, the clinician must be aware of the qualities of each appliance in addition to appropriate treatment planning and patient selection.