Steele JG, Treasure ET, O'Sullivan I, Morris J, Murray JJ Adult Dental Health Survey 2009: transformation in British oral health 1968–2009. Br Dent J. 2012; 213:523-527
Thomas SJ, Highes C, Atkinson C, Ness AR, Revington PJ Is there an epidemic of admissions for surgical treatment of dental abscess in the UK?. Br Med J. 2008; 336:1219-1220
Freeman R Reforming NHS dentistry. Equitable distribution of affordable dental services is still possible. Br Med J. 2008; 336:1202-1203
Moles DR, Frost C, Grundy C Inequalities in availability of National Health Service general dental practitioners in England and Wales. Br Dent J. 2001; 190:548-553
Vieira F, Allen SM, Stocks RM, Thompson JW Deep neck infection. Otolarngol Clin North Am. 2008; 41:459-483
Ellis H, 11th edn. Blackwell: Oxford; 2006
Handley T, Devlin M, Koppel D, McCaul J The sepsis syndrome in odontogenic infection. J Intensive Care Med. 2009; 10:21-25
Dellinger RP, Levy MM, Carlet JM Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock. Intensive Care Med. 2008; 34:17-60
Robertson D, Smith AJ The microbiology of the acute dental abscess. J Med Microbiol. 2009; 58:155-162
Al-Qamachi LH, Aga H, McMahon J, Leonard A Microbiology of odontogenic infections in deep neck spaces: a retrospective study. Br J Oral Maxillofac Surg. 2010; 48:37-39
A guide to deep neck space fascial infections for the dental team Barry Main John Collin Margaret Coyle Ceri Hughes Steven Thomas Dental Update 2024 43:8, 707-709.
Lecturer and Specialty Registrar, Division of Oral and Maxillofacial Surgery, School of Oral and Dental Science, University of Bristol, Lower Maudlin Street, Bristol, BS1 2LY
Specialty Registrar in Oral and Maxillofacial Surgery, Division of Oral and Maxillofacial Surgery, School of Oral and Dental Science, University of Bristol, Lower Maudlin Street, Bristol BS1 2LY
Professor and Consultant in Oral and Maxillofacial Surgery, Division of Oral and Maxillofacial Surgery, School of Oral and Dental Science, University of Bristol, Lower Maudlin Street, Bristol, BS1 2LY, UK
The majority of serious dental infections can be prevented by early treatment of the local pathology. Patients with potentially life-threatening neck space infections arising from the oral cavity may, however, still present in dental practice. This paper outlines the pertinent surgical anatomy and pathophysiology, signs and symptoms, and key early-stage management of these severe infections.
CPD/Clinical Relevance: The dental team should be able to assess patients presenting with potential neck space involvement from a dental or oral infection. They should be able to instigate appropriate early treatment, and identify those requiring prompt referral for assessment and management.
Article
Despite overall improvements in the oral health of the population,1 reports in the literature suggest an increase in the incidence of patients being managed for the complications of dental abscess by maxillofacial teams in the UK.2 An analysis of in-patient episodes for NHS Trusts in England showed a doubling in admissions and bed days required for the operative management of dental abscess in the period 1998–1999 and 2005–2006.2 The reasons for this are not entirely clear but it may, in part, reflect changes in the delivery of, and access to, dental services in the UK.3 There is also evidence that the incidence of dental abscess is related to socio-economic deprivation.4 These statistics reveal that, in many cases, dental infection is not being addressed at an early stage and, therefore, patients are presenting late with potentially serious sequelae.
One of the most serious and potentially life-threatening complications of dental sepsis is the spread of infection into the fascial spaces of the neck. In adults, odontogenic infections are the most common cause of such a presentation, while in children the tonsils account for the majority of cases.5 Other aetiologies include salivary gland infection, trauma, post-operative infection, and complications related to congenital abnormalities of the neck such as an infected thyroglossal duct cyst.5
Whatever the cause, spread of infection through the potential spaces in the neck poses a risk to the airway. It may also result in systemic compromise and cardiovascular collapse. Furthermore, infection can spread inferiorly into the mediastinal or pleural cavities; or superiorly to the peri-orbital or orbital tissues, and via the facial vein to the cavernous sinus. Patients at risk of these complications may present initially to the dental team. It is important, therefore, that dental practitioners are able to assess these cases and arrange for urgent referral to a maxillofacial team for further management when required.
This paper provides the dental team with the knowledge required to recognize patients with actual or impending neck space infection. The basic surgical anatomy of the fascial spaces is reviewed to provide an illustration of how infection arising in the dental tissues may spread through them. The cardinal clinical signs and symptoms of deep neck space infection are described, with a particular emphasis on those features that merit the prompt input of a maxillofacial team. The principles of the management of deep neck space infections are also described. Table 1 provides a glossary of commonly used terminology.
Term
Definition
Abscess
Localized collection of pus
Cellulitis
Inflammation of the subcutaneous tissues with no significant localization of pus (may later organize to form an abscess)
Sepsis
The presence of the systemic inflammatory response syndrome (temperature <36° or >38°; pulse rate >90 per minute; respiratory rate >20 per minute; and white cell count <4 or >12×109/L) plus confirmed infection
The neck is a complex anatomical region. It serves musculoskeletal functions and as a conduit for blood vessels, nerves, the airway, and upper gastrointestinal tract. Fascia is the loose connective tissue that lies beneath the skin, envelopes the muscles, and invests the internal organs.6 The vital structures of the neck are, therefore, invested in cervical fascia. This is made up of the superficial (lying just deep to the subcutaneous tissue to surround the whole neck and invest the platysma muscle) and deep layers. The deep cervical fascia consists of three layers:
The superficial (or investing) layer of deep cervical fascia surrounds the entire neck and envelopes the sternocleidomastoid and trapezius muscles. This layer divides to form the capsules of the submandibular and parotid salivary glands.
The middle layer extends from the base of the skull into the thoracic cavity to become continuous with the pericardium. This layer invests the pharynx, larynx, trachea, oesophagus, thyroid gland, and strap muscles.
The deep layer surrounds the spine and paravertebral muscles.
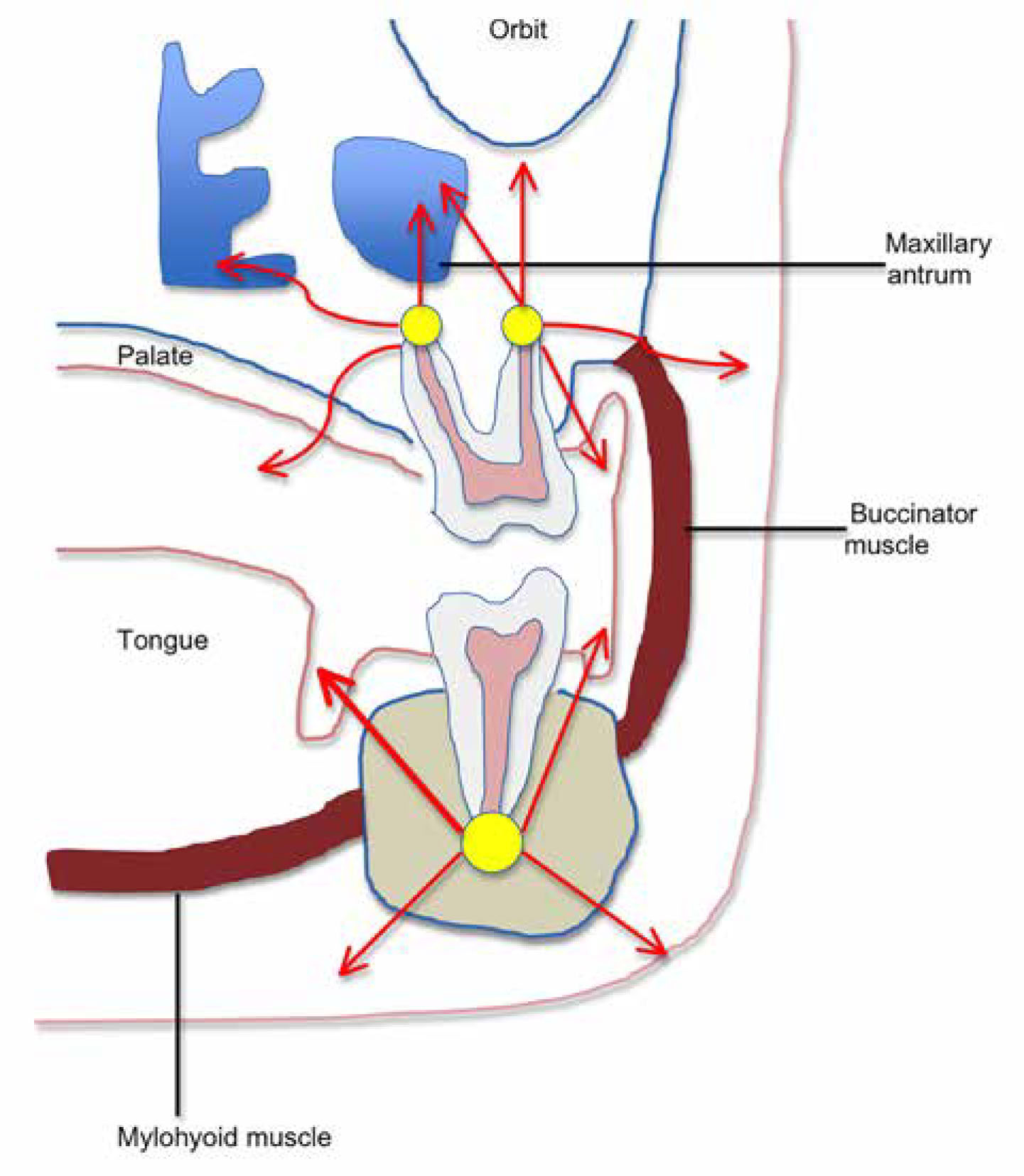
Between these layers of deep fascia are potential spaces containing loose connective tissue. It is within these layers that infection arising in the dental tissues can spread. Table 2 summarizes the fascial spaces of the neck and Figure 1 demonstrates the potential paths of spread of infection of odontogenic origin. If infection spreads inferiorly into the neck, the anatomy of the deep fascial tissues will limit spread to a certain extent, but the complex arrangement of connection between some of the spaces means that, if infection is not controlled, more distant spread is possible.
*The danger space lies between the retropharyngeal and prevertebral spaces and extends from the base of the skull to the diaphragm.
Figure 1. Potential routes of spread of infection of odontogenic origin.
Clinical features of deep neck space infection
Symptoms
In addition to pain around the causative tooth or teeth, patients with neck space infection will feel generally unwell. They may complain of fever and rigors. Particularly worrying symptoms are trismus, dysphagia, dyspnoea, and change in voice. An example of the latter is the ‘hot potato’ voice resulting from elevation of the floor of mouth and tongue in the oral cavity. These all indicate actual or impending airway compromise and patients presenting in this way should be referred for urgent assessment in hospital.
Signs
Vital signs
Septic patients may be tachycardic (pulse rate >90 beats per minute) and pyrexial. If there is an abscess, a swinging pyrexia may be seen. The respiratory rate is a sensitive sign that may increase before an abnormality is seen in other vital signs. A rate of >20 breaths per minute is abnormal in an adult.7
The combination of a high respiratory rate, tachycardia, very high or very low temperature, with a very high or very low white blood cell count is the systemic inflammatory response syndrome (SIRS). Sepsis is defined as the presence of SIRS in addition to a confirmed infective process. Septic shock occurs when a septic patient remains hypotensive despite aggressive attempts at restoring the blood pressure. Importantly, it is well recognized that the prognosis of septic patients is improved when appropriate treatment is delivered promptly.8
Surgical signs
In addition to these general signs of sepsis, there are specific clinical features of neck space infection that reflect the regional anatomy. These features are summarized in Table 3. It is important to recognize that more than one space can be involved. Occasionally, a patient may be systemically very unwell (showing signs of septic shock) without any overt neck swelling or other loco-regional symptoms or signs.
Anatomical Space
Description of Space
Signs and Symptoms of Infection in Space
Sublingual space
Bounded by the mucosa of the floor of the mouth superiorly and the mylohyoid muscle inferiorly.
Swollen, red floor of mouth. Little or no extra-oral sign of swelling. Elevation of the tongue may result in dysarthria, dysphagia and/or dyspnoea.
Submandibular space
Lies between the mylohyoid muscle, superficial fascia, platysma and skin. Contains the submandibular gland and lymph nodes.
Painful, red swelling of the neck immediately below the lower border of the mandible. Involvement of the muscles of mastication results in trismus.
Submental space
Lies between the mylohyoid muscles and the skin, just beneath the chin. Contains submental lymph nodes.
Swelling and erythema of the chin.
Submasseteric space
Bounded by the lateral border of the mandible and the medial aspect of the masseter.
Pain and swelling over the angle of the mandible plus trismus.
Parapharyngeal (lateral pharyngeal) space
Extends from the base of the skull to the level of the hyoid bone. It contains the internal carotid artery, the internal jugular vein, cranial nerves IX to XII and the sympathetic chain.
Examination of the oro-pharynx reveals deviation of the uvula to the opposite side, accompanied by displaced tonsil and lateral pharyngeal surface. There may be trimsus and swelling of the lateral neck. Involvement of vital structures may include internal jugular vein thrombosis, Horner syndrome* and meningitis.
Retropharyngeal space
This space lies behind the pharynx and oesophagus between the skull base and mediastinum.
The patient will be unwell and complain of severe sore throat. There will be dysphagia and limitation in neck movement.
*Horner syndrome is caused by involvement of the sympathetic chain and is characterized by the triad of ptosis (drooping eyelid), miosis (constricted pupil) and anhydrosis (lack of sweating on affected side of face).
Ludwig's angina
Ludwig's angina is a specific diagnosis and is defined as a bilateral cellulitis of the submandibular and sublingual spaces, most often arising from a lower molar tooth. The floor of the mouth contains the sublingual, submandibular and submental spaces with ready communication across the midline. Infection can, therefore, spread to involve all spaces in the floor of the mouth. Clinically, there is a firm swelling of the floor of the mouth and resultant elevation of the tongue. The submandibular and sublingual spaces become tense and tender. There may be accompanying trismus, dysphagia, and respiratory embarrassment. The cellulitis may spread to involve the lateral pharyngeal space. Figure 2 shows the typical clinical appearance in Ludwig's angina. The importance of recognizing this diagnosis is that these patients require immediate referral to hospital for urgent antibiotic therapy and surgical drainage, with or without additional airway support.
Figure 2. Typical clinical appearance in Ludwig's angina.
Investigation of deep neck space infection
Investigation of the patient with a neck space infection will be dictated by the individual clinical scenario and urgency with which hospital management is required.
Investigation in the dental setting
The assessment of the patient in the dental setting should include checking the temperature and basic vital signs (pulse and respiratory rates). A plain radiograph should be obtained if the patient is well enough to tolerate it. In patients with severe odontogenic infection there is often some degree of trismus that makes obtaining intra-oral views difficult. A dental panoramic tomogram can, therefore, provide a good overview of the state of the entire dentition and is likely to reveal the source of any infection. Where possible, the dental practitioner referring a patient into hospital should send the imaging with the patient. This helps save time in the assessment and management of the patient while also avoiding unnecessary repeated exposure to radiation.
Investigation in the hospital setting
Patients admitted to hospital with neck space infection will undergo blood tests, possible further imaging including ultrasound and/or CT scan, and eventual microbiological investigation. Where possible, a sample of pus is obtained for microbiological culture and antibiotic sensitivity testing. Most often, pus is obtained at the time of operation. The acute odontogenic abscess is usually polymicrobial in nature, comprising facultative anaerobes (for example, viridans streptococci and the Streptococcus anginosus group), and strict anaerobes like Prevotella and Fusobacterium species.9,10
Principles of the surgical management of deep neck space infection
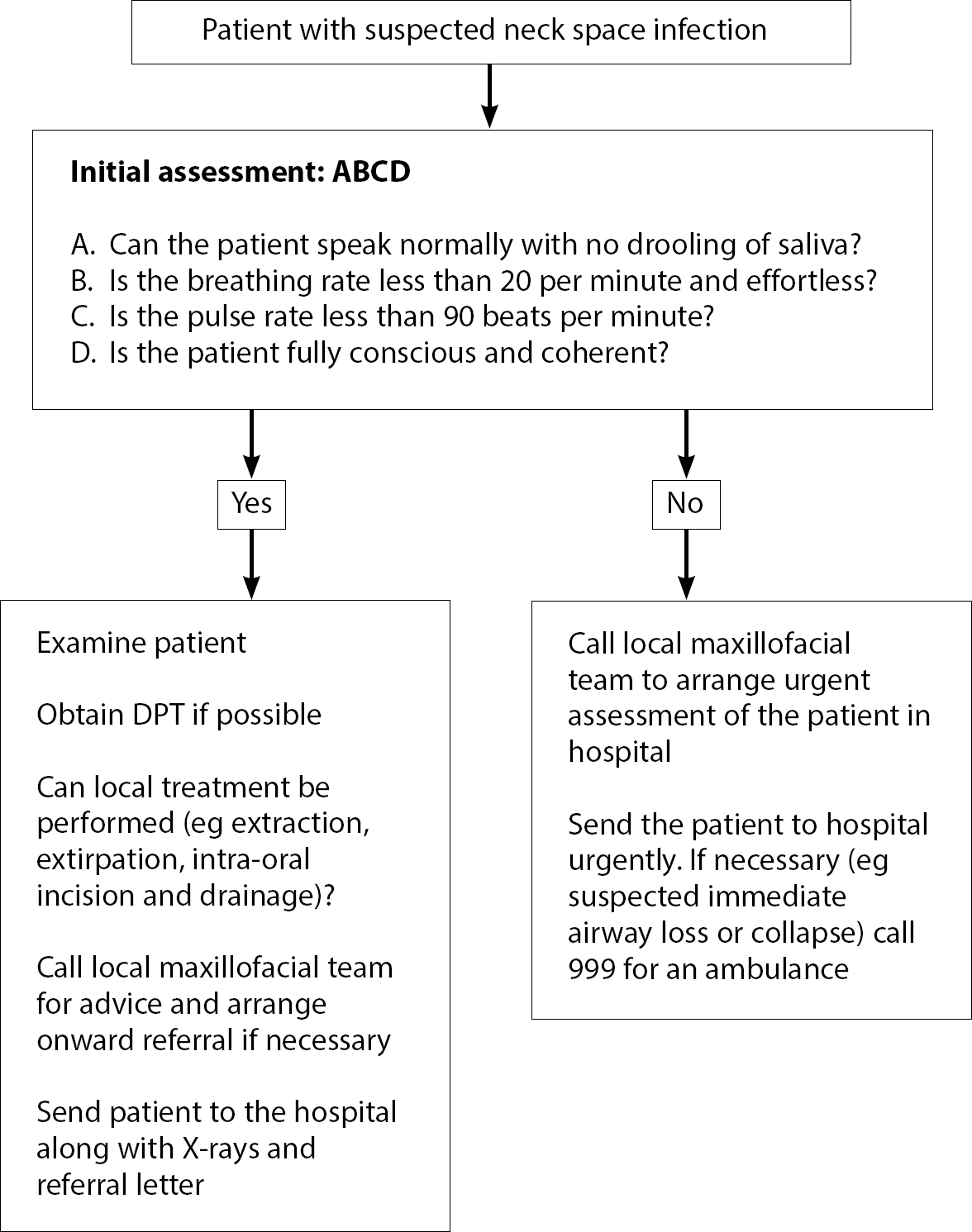
Figure 3 provides a guide to the initial assessment and management of patients with suspected neck space infection. The patient presenting with suspected neck space infection should be assessed immediately for Airway, Breathing, and Circulation (ABC). This gauges the urgency of the need for referral to hospital. A stable patient with localized swelling and minimal soft tissue involvement is likely to be suitable for early, local treatment including pulp extirpation or extraction of the tooth, with or without systemic antibiotics.
Figure 3. Guide to the initial assessment and management in suspected neck space infection.
For those patients referred to hospital, the principles of establishing surgical drainage, removal of the source of infection, and systemic antibiotics also apply. Septic patients will be treated aggressively with fluid resuscitation and early, empirical administration of antibiotics. Drainage of neck space infections will usually take place in the operating theatre under general anaesthetic. Severe airway compromise may necessitate placement of a tracheostomy tube and post-operative admission to intensive care. In Ludwig's angina, there is often no collection of pus, but surgical exploration of the affected spaces is performed to ‘decompress’ the neck. Surgical drains are placed until resolution of the infection. Corticosteroids (eg dexamethasone) may be given to help reduce the oedema associated with these infections.
Summary
It is important to remember that the vast majority of odontogenic infections can be managed using local measures such as extraction of the tooth, extirpation of the pulp, or intra-oral incision and drainage of a buccal space abscess. Antibiotic therapy is indicated where there are signs of systemic infection, but they are not a substitute for removing the source of infection.
Occasionally, infection arising in the oro-dental tissues can spread into the fascial spaces of the neck, leading to potentially life-threatening airway compromise and/or sepsis. This paper has discussed the pertinent surgical anatomy and described the cardinal signs and symptoms of spreading infection that should alert the dental practitioner to a patient who required specialist in-patient assessment and management.