Turp JC, Komine F, Hugger A. Efficacy of stabilization splints for the management of patients with masticatory muscle pain: a qualitative systematic review. Clin Oral Investig. 2004; 8:179-195 https://doi.org/10.1007/s00784-004-0265-4
Durham J, Aggarwal V, Davies S, Harrison S. Temporomandibular disorders (TMDs): an update and management guidance for primary care from the UK Specialist Interest Group in Orofacial Pain and TMDs (USOT). RCS England. 2013;
Moufti A, Lilico J, Wassell R. How to make a well-fitting stabilization splint. Dent Update. 2007; 34:398-408
Magdaleno F, Ginestal E. Side effects of stabilization occlusal splints: a report of three cases and literature review. Cranio. 2010; 28:128-135 https://doi.org/10.1179/crn.2010.018
Al-Ani Z, Davies S, Sloan P, Gray R. Change in the number of occlusal contacts following splint therapy in patients with a temporomandibular disorder (TMD). Eur J Prosthodont Restor Dent. 2008; 16:98-103
Fujii T, Torisu T, Nakamura S. A change of occlusal conditions after splint therapy for bruxers with and without pain in the masticatory muscles. Cranio. 2005; 23:113-118
Nikolopoulou M, Ahlberg J, Visscher CM Effects of occlusal stabilization splints on obstructive sleep apnea: a randomized controlled trial. J Orofac Pain. 2013; 27:199-205 https://doi.org/10.11607/jop.967
Wassell RW, Verhees L, Lawrence K Over-the-counter (OTC) bruxism splints available on the Internet. Br Dent J. 2014; 216 https://doi.org/10.1038/sj.bdj.2014.452
Gray R, Davies S. Occlusal splints and temporomandibular disorders: why, when, how?. Dent Update. 2001; 28:194-199
Wright E, Anderson G, Schulte J. A randomized clinical trial of intraoral soft splints and palliative treatment for masticatory muscle pain. J Orofac Pain. 1995; 9:192-199
Truelove E, Huggins KH, Mancl L, Dworkin SF. The efficacy of traditional, low-cost and nonsplint therapies for temporomandibular disorder: a randomized controlled trial. J Am Dent Assoc. 2006; 137:1099-1107 https://doi.org/10.14219/jada.archive.2006.0348
Longridge N, Milosevic A. The bilaminar (dual-laminate) protective night guard. Dent Update. 2017; 44:648-654
Blumenfeld A, Bender S, Glassman B, Pinto A. Patterns of use for an enhanced nociceptive trigeminal inhibitory splint. Inside Dentistry. 2011; 7
Shankland W. Migraine and tension-type headache reduction through pericranial muscular suppression: a preliminary report. Cranio. 2001; 19:269-278
Jokstad A, Mo A, Krogstad B. Clinical comparison between two different splint designs for temporomandibular disorder therapy. Acta Odontol Scand. 2005; 63:218-226
Magnusson T, Adiels A-M, Nilsson H, Helkimo M. Treatment effect on signs and symptoms of temporomandibular disorders--comparison between stabilisation splint and a new type of splint (NTI). A pilot study. Swedish Dent J. 2004; 28:11-20
Stapelmann H, Türp J. The NTI-tss device for the therapy of bruxism, temporomandibular disorders, and headache–Where do we stand? A qualitative systematic review of the literature. BMC Oral Health. 2008; 8
Bereznicki T, Barry E, Wilson NHF. Unintended changes to the occlusion following the provision of night guards. Part two: management. Br Dent J. 2019; 226:649-656 https://doi.org/10.1038/s41415-019-0261-3
Fleten A, Gjerdet N. Accidental swallowing of an incisal splint. Den Norske tannlaegeforenings tid. 2004; 114:638-639
Yadav S, Karani J. The essentials of occlusal splint therapy. Int J Prosthet Dent. 2011; 2:12-21
Chen HM, Liu MQ, Yap AU, Fu KY. Physiological effects of anterior repositioning splint on temporomandibular joint disc displacement: a quantitative analysis. J Oral Rehabil. 2017; 44:664-672 https://doi.org/10.1111/joor.12532
Naeije M, Te Veldhuis A, Te Veldhuis E Disc displacement within the human temporomandibular joint: a systematic review of a ‘noisy annoyance’. J Oral Rehabil. 2013; 40:139-158
Lundh H, Westesson PL, Kopp S, Tillstrom B. Anterior repositioning splint in the treatment of temporomandibular joints with reciprocal clicking: comparison with a flat occlusal splint and an untreated control group. Oral Surg Oral Med Oral Pathol. 1985; 60:131-136 https://doi.org/10.1016/0030-4220(85)90280-4
Conti PC, Correa AS, Lauris JR, Stuginski-Barbosa J. Management of painful temporomandibular joint clicking with different intraoral devices and counseling: a controlled study. J Appl Oral Sci. 2015; 23:529-535 https://doi.org/10.1590/1678-775720140438
Davies SJ, Gray RJ. The pattern of splint usage in the management of two common temporomandibular disorders. Part III: Long-term follow-up in an assessment of splint therapy in the management of disc displacement with reduction and pain dysfunction syndrome. Br Dent J. 1997; 183:279-283 https://doi.org/10.1038/sj.bdj.4809495
Eberhard D, Bantleon HP, Steger W. The efficacy of anterior repositioning splint therapy studied by magnetic resonance imaging. Eur J Orthod. 2002; 24:343-352 https://doi.org/10.1093/ejo/24.4.343
Davies SJ, Gray RJ. The pattern of splint usage in the management of two common temporomandibular disorders. Part I: The anterior repositioning splint in the treatment of disc displacement with reduction. Br Dent J. 1997; 183:199-203 https://doi.org/10.1038/sj.bdj.4809466
Manns A, Miralles R, Pena M. The effect of different occlusal splints on the electromyographic activity of elevator muscles: A comparative study. J Gnathol. 1988; 7:61-73
Gray R, Davies S, Quayle A, Wastell D. A comparison of two splints in the treatment of TMJ pain dysfunction syndrome. Can occlusal analysis be used to predict success of splint therapy?. Br Dent J. 1991; 170:55-58
Rinchuse DJ, Rinchuse DJ, Kandasamy S. Evidence-based versus experience-based views on occlusion and TMD. Am J Orthod Dentofacial Orthop. 2005; 127:249-254 https://doi.org/10.1016/j.ajodo.2004.02.012
Tavera AT, Montoya MC, Calderon EF Approaching temporomandibular disorders from a new direction: a randomized controlled clinical trial of the TMDes ear system. Cranio. 2012; 30:172-182 https://doi.org/10.1179/crn.2012.027
Baad-Hansen L, Jadidi F, Castrillon E Effect of a nociceptive trigeminal inhibitory splint on electromyographic activity in jaw closing muscles during sleep. J Oral Rehabil. 2007; 34:105-111 https://doi.org/10.1111/j.1365-2842.2006.01717.x
Daud A. TMD treatment – a splint alterantive.: Dentistry Magazine; 2017
Ernst M, Schenkenberger AE, Domin M Effects of centric mandibular splint therapy on orofacial pain and cerebral activation patterns. Clin Oral Investig. 2020; 24:2005-2013 https://doi.org/10.1007/s00784-019-03064-y
Lotze M, Lucas C, Domin M, Kordass B. The cerebral representation of temporomandibular joint occlusion and its alternation by occlusal splints. Hum Brain Mapp. 2012; 33:2984-2993 https://doi.org/10.1002/hbm.21466
Raphael K, Marbach J, Klausner J Is bruxism severity a predictor of oral splint efficacy in patients with myofascial face pain?. J Oral Rehabil. 2003; 30:17-29
Solberg WK, Clark GT, Rugh JD. Nocturnal electromyographic evaluation of bruxism patients undergoing short term splint therapy. J Oral Rehabil. 1975; 2:215-223 https://doi.org/10.1111/j.1365-2842.1975.tb00915.x
Temporomandibular disorders. Part 4: appliance therapy Martin James Funmi Oluwajana Emma Foster-Thomas Charles Crawford Emma Foster-Thomas Peter Clarke A Johanna Leven Dental Update 2024 49:7, 707-709.
Authors
MartinJames
Specialty Registrar in Restorative Dentistry, University Dental Hospital of Manchester
Appliances have been used in the management of temporomandibular disorders (TMD) for many years, and over this time designs have waxed and waned in popularity. The majority of appliance designs have few studies to support their use and what evidence is available, is often of low quality. This article, the fourth in a series of six, reviews the mechanisms of action, evidential support for, and provides advice on when to use commonly used appliance designs.
CPD/Clinical Relevance: There are a plethora of splint designs in use, but it is essential that the evidence supporting each is understood so that the most appropriate design is used for each individual situation.
Article
Martin James
Appliance therapy has been used in TMD management for over a century, and despite being commonly prescribed, there remains a lack of conclusive evidence to support the efficacy of one design over another.1 The aim of this article is to describe and discuss the most commonly used occlusal appliances in the management of TMDs, to present their supporting evidence and to provide some pragmatic guidance to general dental practitioners.
The literature on this topic is heterogeneous in terms of methodology and outcome measures, and this variation continues into the use of nomenclature. To avoid ambiguity and misunderstanding, standardized terms are used throughout this article (Table 1).
Term
Synonyms
Stabilization splint (SS)
Michigan splint, Tanner splint, hard acrylic splint, occlusal splint, Fox appliance, centric relation appliance
SS are considered by many as the gold standard of appliance therapy for patients with a diagnosis of myofascial pain. In general, they are used alongside other conservative measures such as self-management, physical therapies and pharmacological treatments.2 Unfortunately, the literature on SS not only varies in quality, but is difficult to interpret and presents contradictory outcomes.3,4
A Cochrane review of 12 randomized controlled trials (RCTs) showed no significant advantage of an SS over any other active treatment (acupuncture, bite plates, biofeedback/stress management, visual feedback, relaxation, jaw exercises and placebo appliance) and only weak evidence for their effectiveness versus no treatment.3 Another Cochrane review, this one identifying five suitable RCTs investigating splint therapy for sleep bruxism, showed SS had no benefit over other treatments (placebo splints, mandibular advancement device and transcutaneous electric nerve stimulation) or no treatment.5
With the lack of high-quality randomized controlled clinical trials, lower-level evidence must be considered to support clinical decision-making. Fricton et al4 undertook a more inclusive systematic review and meta-analysis of 47 RCTs: they found a statistically significant difference with SS, almost 2.5 times more likely to improve symptoms than a placebo appliance (covering the palatal aspect of the teeth and not interfering with the static or dynamic occlusal contacts). Interestingly, the same study found the difference between SS therapy and no treatment to be non-significant.
SS can be difficult and time consuming to fabricate, fit and adjust correctly. They are, therefore, infrequently constructed in UK general dental practice.6 Step-by-step guides are available and the features well defined to effectively provide a temporary and removable ideal, mutually protected, occlusal scheme.7 In summary these:
Should be constructed on the arch with the least teeth to allow the maximum number of occlusal contacts;
Provide full occlusal coverage with contact on every tooth simultaneously on the terminal hinge axis (THA)/in centric relation (CR);
Provide posterior disclusion in anterior and lateral excursions;
Provide canine guidance in lateral excursions where achievable or group function on the first premolar if not;
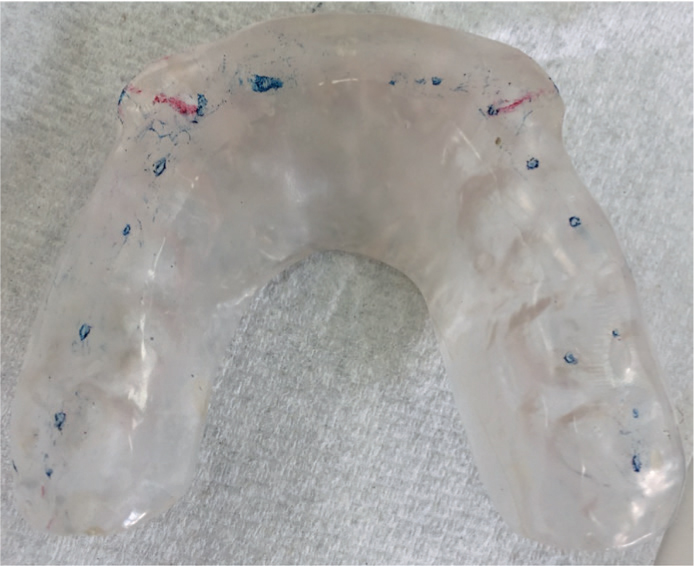
Provide shared incisal guidance in anterior excursions (Figure 1).
Figure 1. A balanced stabilization splint: static contacts are present on each tooth on TMH/in CR, marked in blue, and dynamic contacts with anterior guidance shared by the incisors and lateral guidance on the canines, marked in red.
The reasons why SS may cause relief of TMD symptoms is less clear, but possible actions are summarized in Table 2.
Splint type/mechanism of action
SS
Soft/bilaminar splint
ABS
ARPS
LOIS
Positioning the mandibular condyles centrally in the glenoid fossa
T
Positioning of the mandible where the muscles are at their most relaxed position
T
Eliminating posterior interferences that cause deviations or hinder harmonious jaw movement
E
E
E
Reduction of neuromuscular activity
E
E
E
Creation of stable occlusal relationships with uniform tooth contacts
T
T
Sharing the occlusal forces throughout the dental arch
T
T
T
Increased cognitive awareness
E
E
E
E
E
Central changes to pain anticipation and processing
Even conservative treatments have complications, and there are isolated case reports of anterior open bite development during SS wear.8 A plausible mechanism for this rare complication is a change to the rest position of the condyle through changes in the disc position and/or resting muscular tension.9,10 There is also evidence from small sleep studies that an SS may increase the number of apnoeic/hypopnoeic events in patients with obstructive sleep apnoea (OSA), but the clinical relevance of this is questionable.11 Considering the significant morbidity associated with OSA, it would be prudent to screen patients and liaise with the general medical practitioner prior to provision of an SS.
Although the evidence supporting SS is equivocal, most experts agree that their use is at least anecdotally beneficial and patients are generally accepting of wearing an SS so long as the treatment protocol is explained. This is particularly true if they have not had sufficient symptomatic control from other conservative measures. Patients who do not get symptomatic relief from a well-made SS should be further assessed, ideally by an experienced clinician, to confirm the diagnosis and, if necessary, for alternative treatment options to be considered.
Soft and bilaminar splints
Soft splints are usually constructed out of thermoplastic polyvinyl material using a vacuum or pressure former over the study model. Owing to the simplicity of construction, they are very popular.12 Nevertheless, there are concerns about both their resilience and texture, which may potentially encourage increased bruxism and thus worsen symptoms.13 Clinically, it should be confirmed that the appliance is well fitting and provides full coverage, but no occlusal adjustments are conducted. Regular review is essential to assess compliance, effectiveness and identify complications early.
Significant improvements in signs and symptoms have been reported in patients with TMD following treatment with a soft splint.14 There are also completely contradictory reports of soft splints increasing muscular activity.15 Studies on both sides of the argument generally have small sample sizes and short-term follow-up, therefore cannot be relied upon to support an evidence-based recommendation. The possible mechanisms of action of soft and bilaminar splints are summarized in Table 2.
Considering the significant difference in clinical and laboratory time and skill required to construct SS, there have been investigations of various qualities to discover whether similar results can be achieved with simpler designs. One RCT failed to detect a difference between SS, soft splints or homecare instruction alone, although this outcome may have been due to insufficient participants.16 Comfort and compliance is an often-cited reason for a preference for soft splints; however, this is not borne out in the literature, with 38% compliance reported after only 9 weeks.17
The bilaminar splint is similar in design and construction to the vacuumed-formed soft splint, with the exception that the blank used in production is a two-layered ethylene-vinyl acetate, one soft and the other hard. This results in a splint that is as simple in the clinical and laboratory stages as a soft splint, but is more durable.18
Even with little high-quality evidence to support their use, there is a role for soft or bilaminar splints, but they cannot be applied as a panacea. Their role probably lies in emergency TMD management when time will be needed to execute a more definitive strategy, and in the protection of teeth or restorations from parafunctional activity.
Anterior bite splint (ABS)
This category of appliances contains a vast range of designs, but importantly, they all share the common feature of providing static and dynamic occlusal contacts on the anterior teeth only (Figure 2). The most popular proprietary variant is the Nociceptive Trigeminal Inhibition Tension Suppression System (NTI/NTI-tss; NTI-TSS Inc, Mishawaka, IN, USA), known in the UK as the Sleep Clench Inhibitor (Sci, S4S (UK) Ltd, Sheffield), which can be fabricated chairside or in a laboratory (Sci+).19 NTI was first described as a treatment for migraines and tension-type headaches and showed benefit compared to a placebo appliance (whitening tray).20 While not fully understood, several mechanisms of action of ABS have been proposed/tested (Table 2).
Figure 2. A Nociceptive Trigeminal Inhibition Tension Suppression System appliance in situ: static and dynamic contacts are only present anteriorly due to the partial coverage design. Image courtesy of Hussain Rashid.
Several RCTs have investigated the effect of various ABS against SS with inconsistent findings ranging from no difference21 to the superiority of the SS.22
Full-time wear of an ABS should be actively discouraged alongside regular review. This is due to the risk of occlusal changes of which there are reports from both normal clinical practice and well-supervised controlled trials demonstrating how rapidly this may occur.22,23 Occlusal derangements caused by partial coverage splints can be exceptionally difficult to manage.24 There are also isolated reports of increased tooth mobility and sensitivity.21
Very serious complications of medical emergencies resulting specifically from NTI wear have also been reported with four cases of aspiration21 and one of ingestion, which became lodged in the oesophageal entrance.25
An evolution of the ABS exists whereby the anterior device is affixed to a full coverage vacuum-/pressure-formed appliance, similar to an Essix retainer, and addition of a vacuum-/pressure-formed splint in the opposing arch. This splint type is sometimes referred to as a B-Splint or an SCi+ Dual Arch Slider by its proponents. This modification theoretically reduces the risk of occlusal changes and aspiration/ingestion; however, although there are mentions of this splint design in reviews,26 experimental evidence is elusive.
General conclusions on this splint design echo that of a systematic review on the subject:23
There is sufficient evidence for the role of ABS for emergency TMD management in those with severe trismus, precluding full arch impressions, in whom reduced muscular activity is desirable;
There is insufficient evidence to show advantage or equivalence with SS;
Given the risk of catastrophic occlusal changes, aspiration and ingestion, extreme caution needs to be exercised when using partial coverage devices.
Anterior re-positioning splints (ARPS)
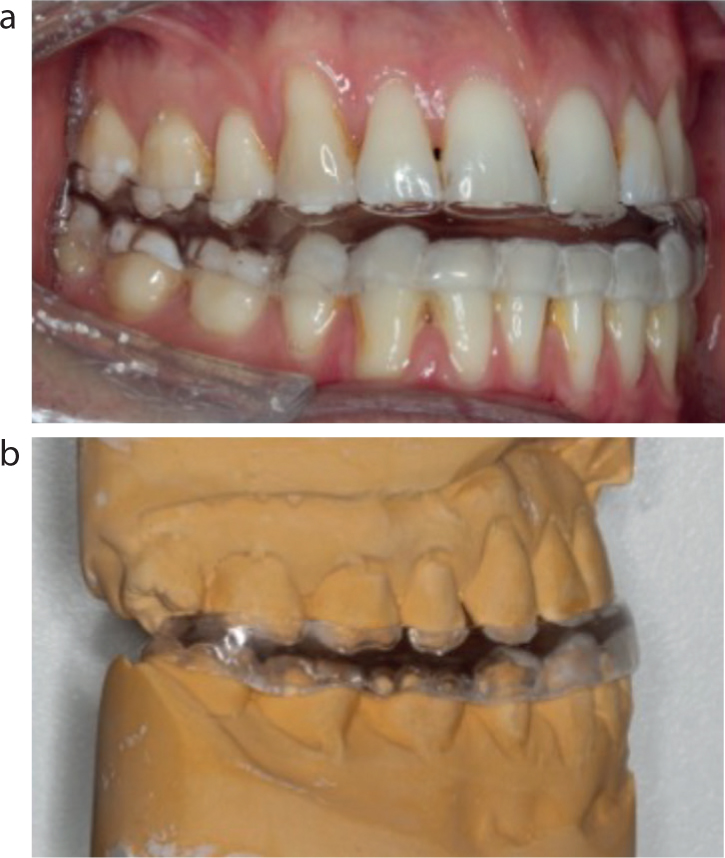
The primary mechanism by which an ARPS functions is to hold the mandible in an anterior position (Figure 3) to ‘recapture’ the articulatory disc so that it lies in the correct relationship with the condyle, allowing its attachments to remodel to this new position (Figure 4). This action has been confirmed with magnetic resonance imaging (MRI) studies27. Potential additional effects are listed in Table 2.
Figure 3.
(a,b) An anterior re-positioning splint in situ: the appliance is retained on the mandibular arch by friction, and 1–2-mm deep indentations for the maxillary teeth guide the mandible repeatedly into a forwards postured position with the disc ‘recaptured’.Figure 4. Diagrammatic representation of anterior disc displacement with reduction. (a) Mandible at rest with the condyle sat on the posterior band of the disc (not the avascular centre). (b) Partial opening with the disc pulled further anteriorly by the lateral pterygoid and impeding further translation of the condyle; the patient may report some restriction to further opening at this point (and closed locking if there is disc displacement without reduction). (c) Full opening with the disc recaptured and the avascular centre of it sitting over the condyle; the patient may report a click at this point as the elastic retro-discal tissues cause sudden recapture. (d) Closing of the mandible into a protrusive position (as if wearing an ARPS) with the avascular centre of the disc still sitting over the condyle; the patient will have no clicking or restriction when opening from this position.
Devices to position the mandible anteriorly have been advocated as a treatment for various different reasons, although they are now generally only used in the management of disc displacements. Disc displacements are generally stable, asymptomatic and not functionally limiting. Even painful or functionally limiting displacements generally improve spontaneously. There is, therefore, rarely a need for active treatment.28 A diagnosis of disc displacement is often comorbid with myofascial pain due to the insertion of the superior belly of the lateral pterygoid into the articular disc; spasm of this muscle may cause joint clicking and myalgia masquerading as arthralgia. It is for this reason that it is prudent to manage myofascial pain prior to considering ARPS therapy for an isolated disc derangement.
The spontaneous improvement in disc displacements makes proving the efficacy of any therapy more difficult. Without a non-treatment control group, it is impossible to prove that any outcome is due to the effect of an appliance, and not just the passage of time. RCTs by Lundh et al29 and Conti et al30 found 6 weeks full time ARPS wear to successfully resolve a joint click in 91% of cases (significantly better than either an SS or no treatment) and gave an 81% reduction in joint pain (significantly better than counselling only). The former study, however, also showed that at 11 and 46 weeks after treatment the click had returned in 86% of those successfully treated, so at 1 year, there was no significant difference from the no-treatment group. Relapse is variable and dependent upon the outcome measure. Up to 90% of patients self-reported continued symptomatic control at 3 years, but only 40% of discs remained in the optimal position when examined by MRI 3 months after treatment.27,31
An ARPS is fabricated in a mandibular position that ‘recaptures’ the disc and, therefore, can only be constructed for patients with disc displacement with reduction, but not without.32 The appliance must also only be used in patients who have ceased growth as otherwise the ARPS would act as a functional orthodontic appliance leading to a reduced overjet, creation of a reverse overjet and/or bilateral posterior open bite. The wear regimen of an ARPS is critical, with a significantly better success rate after 3 months of full-time wear than either daytime only or night-time only.33
In summary, the ARPS is a useful appliance for improving joint clicking and pain in patients with disc displacement with reduction. The appliance, however, is bulky, uncomfortable, requires full-time wear and has unpredictable long-term results. In general, spontaneous improvements in disc displacement occur, therefore the ARPS should be reserved for patients who have a severe click that is affecting their quality of life, and where there has been exclusion or management of myofascial pain.
Localized occlusal interference splint (LOIS)
Also known as an interceptor splint, the localized occlusal interference splint (LOIS) is primarily used in patients with signs or symptoms of awake bruxism and it functions as a habit breaker. The simple design uses stainless steel ball clasps to create contact on the canine or premolar teeth only, preventing all other teeth from touching (Figure 5). This theoretically increases the force on the proprioceptive fibres of the periodontal ligaments, which makes parafunctioning uncomfortable and hence, discouraged. Other modes of action may also contribute (Table 2). LOIS will be unsuccessful in patients who parafunction in extreme excursions. The splint should be worn all day initially to allow identification of the times of day when parafunctioning occurs, and then the splint wear can be tailored to those times. It is essential that the appliance is not worn at night, as conscious discomfort is required to prevent damage.
Figure 5. A localized occlusal interference splint in situ. Static contact is onto the stainless steel ball clasps on the canines only; however, the patient may be able to achieve tooth–tooth contact in extreme excursions; the appliance is retained by wrought clasps between the premolars.
There is little experimental evidence on the effectiveness of the LOIS; however, its use has been shown by electromyography (EMG) studies to reduce masticatory muscle activity similar to an ABS.34 Additionally, an RCT of 68 patients with myofascial pain treated with LOIS compared with SS found no significant difference in patient-reported symptom control.35
Given the simplicity of construction and the evidential support for the LOIS, albeit small, its role in TMD management is exclusively in patients with myofascial pain, awake parafunction and self-reported worsening of symptoms throughout the day or at specific timepoints.
Other intra-oral appliances
The field of appliance therapy for TMD is heavily based on expert opinion owing to the general lack of high-quality experimental evidence.36 This environment is probably the main reason for the huge range of appliance designs that have been suggested in the literature. Table 3 presents a non-exhaustive list of less-common splint designs that lack experimental evidence.
Name
Design and function
Placebo splint or non-occluding splint
Any appliance that does not interfere with the static or dynamic occlusion and therefore is reliant on increased cognitive awareness and the placebo effect
Flat plane splint
A full coverage hard acrylic appliance with contact on every tooth on THA/in CR but with no anterior guidance; aiming to provide a similar effect to an SS, but with less compromise on aesthetics and function to enable full-time wear
A partial-coverage hard acrylic ARPS that covers the mandibular molar teeth only. Designed to be worn full time, this appliance cannot be recommended due to the risk of occlusal derangement
Posterior pivot appliance or decompression splint
A hard acrylic appliance that provides a single posterior contact in each quadrant, theoretically pulling the condyles downward when clenching, decompressing the joint and allowing the disc to re-assume a normal position. The effect is impossible to produce anatomically as the insertions of the masticatory muscles are posterior to the dentition and therefore cannot act anterior to the pivot
Hydrostatic appliance
Bilateral water-filled chambers sit between the posterior teeth theoretically allowing the mandible to optimally position itself
Neuromuscular appliance/orthotic
Proponents of this appliance use EMG-based devices to ‘locate’ the optimal position of the mandible. An orthotic appliance is designed to position the jaw and is usually followed by a full occlusal rehabilitation to make the new position ‘permanent’. Validity studies have concluded that EMG is not sensitive/specific enough to be used as a diagnostic tool in TMD
Extra-oral appliances
Intra-aural inserts (IAI) are a novel TMD treatment, previously marketed as Cerezen (which has been removed from the market). The theorized mechanism of action is that when opened, the mandibular condyles move away from the external acoustic meatus causing an increase in the canal volume. Filling the canal with a hard material in its enlarged state exerts a small amount of pressure on the walls of the ear canal when the jaw is closed, discouraging clenching.37
The only experimental evidence investigating IAI is a single RCT that concluded there was no statistically significant difference between IAI, SS therapy or physiotherapy within the short follow-up.37 There is, however, a high risk that there were insufficient participants to detect a difference between the treatments and, therefore, until further data become available, IAI use cannot be routinely recommended. They may have a role in the management of those who struggle to wear an intra-oral appliance on the understanding that they are currently unproven.
Conclusion
This article has described the appliances used in the management of TMD that have some experimental evidence to support their use, and also briefly described those that do not. The literature in this field is heterogeneous due to:
Recruitment: variation in case definitions and inclusion of single or multiple diagnoses;
Methodology: inconsistency in the description of the appliances, placebos and the control of confounding factors such as analgesia and physiotherapy;
Outcome measures: different combinations of signs and symptoms.
These factors make it challenging to quantitatively compare or combine trials in a meaningful way.
In many cases, the limited evidence must be combined with clinical experience to select the most appropriate appliance therapy; this should only be undertaken when a definitive diagnosis has been established, and simple conservative measures have failed to achieve symptomatic control.