Peck C, Goulet J-P, Lobbezoo F Expanding the taxonomy of the diagnostic criteria for temporomandibular disorders. J Oral Rehabil. 2014; 41:2-23
Soames RW. Skeletal system. In: Gray H, Williams P, Bannister L (eds). New York: Churchill Livingstone;
Alomar X, Medrano J, Cabratosa J Anatomy of the temporomandibular joint. Semin Ultrasound CT. 2007; 28:170-83
Shaffer S, Brismée J-M, Sizer P, Courtney C. Temporomandibular disorders. Part 1: anatomy and examination/diagnosis. J Man Manip Ther. 2014; 22:2-12
Dworkin S. The OPPERA study: act one. J Pain. 2011; 12:T1-T3
Maixner W, Diatchenko L, Dubner R Orofacial pain prospective evaluation and risk assessment study – the OPPERA study. J Pain. 2011; 12:T4-T11.e2
Slade G, Bair E, Greenspan J Signs and symptoms of first-onset tmd and sociodemographic predictors of its development: the OPPERA prospective cohort study. J Pain. 2013; 14:T20-T32.e3
Aggarwal V, McBeth J, Zakrzewska J, Lunt M, Macfarlane G. The epidemiology of chronic syndromes that are frequently unexplained: do they have common associated factors?. Int J Epidemiol. 2006; 35:468-76
Hoffmann R, Kotchen JM, Kotchen T Temporomandibular disorders and associated clinical comorbidities. Clin J Pain. 2011; 27:268-74
Phillips C. The cost and burden of chronic pain. Rev Pain. 2009; 3:2-5
Cousins M, Brennan F, Carr D. Pain relief: a universal human right. Pain. 2004; 112:1-4
Suvinen T, Reade P, Kemppainen P Review of aetiological concepts of temporomandibular pain disorders: towards a biopsychosocial model for integration of physical disorder factors with psychological and psychosocial illness impact factors. Eur J Pain. 2005; 9:613-633
Engel G. The need for a new medical model: a challenge for biomedicine. Science. 1977; 196:129-136
McNeill C. Management of temporomandibular disorders: concepts and controversies. J Prosthet Dent. 1997; 77:510-522
Fillingim R, Ohrbach R, Greenspan J Psychological factors associated with development of TMD: the OPPERA prospective cohort study. J Pain. 2013; 14:T75-T90 https://doi.org/10.1016/j.jpain.2013.06.009
Slade G, Fillingim R, Sanders A Summary of findings from the OPPERA prospective cohort study of incidence of first-onset temporomandibular disorder: implications and future directions. J Pain. 2013; 14:T116-T24
Sanders A, Slade G, Bair E General health status and incidence of first-onset temporomandibular disorder: the OPPERA prospective cohort study. J Pain. 2013; 14:T51-T62
Svensson P, Jadidi F, Arima T Relationships between craniofacial pain and bruxism. J Oral Rehabil. 2008; 35:524-547
Van Der Meulen M, Lobbezoo F Self-reported oral parafunctions and pain intensity in temporomandibular disorder patients. J Orofac Pain. 2006; 20:31-35
Manfredini D, Lombardo L, Siciliani G. Temporomandibular disorders and dental occlusion. A systematic review of association studies: end of an era?. J Oral Rehabil. 2017; 44:908-23
Bell Y, Jämsä T, Korri S Effect of artificial occlusal interferences depends on previous experience of temporomandibular disorders. Acta Odontol Scand. 2002; 60:219-222
Pullinger A, Seligman D. Trauma history in diagnostic groups of temporomandibular disorders. Oral Surg Oral Med Oral Pathol. 1991; 71:529-534 https://doi.org/10.1016/0030-4220(91)90355-g
Dworkin S, Leresche L. Research diagnostic criteria for temporomandibular disorders: review, criteria, examinations and specifications, critique. J Craniomandib Disord. 1992; 6:301-305
Ghurye S, McMillan R. Pain-related temporomandibular disorder–current perspectives and evidence-based management. Dent Update. 2015; 42:533-546 https://doi.org/10.12968/denu.2015.42.6.533
Kroenke K, Spitzer RL, Williams JB, Löwe B. An ultra-brief screening scale for anxiety and depression: the PHQ–4. Psychosomatics. 2009; 50:613-621 https://doi.org/10.1176/appi.psy.50.6.613
Doufas AG. Pain and sleep.: Elsevier; 2017
Smith M, Haythornthwaite J. How do sleep disturbance and chronic pain inter-relate? Insights from the longitudinal and cognitive-behavioral clinical trials literature. Sleep Med Rev. 2004; 8:119-132 https://doi.org/10.1016/s1087-0792(03)00044-3
Buenaver L, Quartana P, Grace E Evidence for indirect effects of pain catastrophizing on clinical pain among myofascial temporomandibular disorder participants: the mediating role of sleep disturbance. Pain. 2012; 153:1159-1166 https://doi.org/10.1016/j.pain.2012.01.023
Essick GK, Raphael KG, Sanders AE, Lavigne G. Orofacial pain and temporomandibular disorders in relation to sleep-disordered breathing and sleep bruxism.: Elsevier; 2017
Schiffman E, Ohrbach R, Truelove E Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group. J Oral Facial Pain Headache. 2014; 28:6-27
Gonzalez Y, Schiffman E, Gordon S Development of a brief and effective temporomandibular disorder pain screening questionnaire. J Am Dent Assoc. 2011; 142:1183-1191 https://doi.org/10.14219/jada.archive.2011.0088
Epstein JB, Caldwell J, Black G. The utility of panoramic imaging of the temporomandibular joint in patients with temporomandibular disorders. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001; 92:236-239 https://doi.org/10.1067/moe.2001.114158
Petersson A. What you can and cannot see in TMJ imaging – an overview related to the RDC/TMD diagnostic system. J Oral Rehabil. 2010; 37:771-778 https://doi.org/10.1111/j.1365-2842.2010.02108.x
Temporomandibular Disorders. Part 1: Anatomy, Aetiology, Diagnosis and Classification Funmi Oluwajana Pete Clarke Emma Foster-Thomas Martin James Charles Crawford Dental Update 2024 49:4, 707-709.
Authors
FunmiOluwajana
Specialty Registrar in Restorative Dentistry, University Dental Hospital of Manchester; Clinical Fellow, Health Education England Northwest
Temporomandibular disorders (TMD) are the most common causes of chronic pain in the orofacial region. The aetiology of TMD is complex owing to its multifactorial biopsychosocial nature. TMD shares many commonalities, and can be associated with, other chronic pain conditions. The physical and psychological impact of chronic pain on the individual can be far-reaching and should not be underestimated. This article, the first of a six-part series, aims to provide the reader with a background to TMDs as well as an overview of the clinical examination and diagnostic process for patients presenting with TMD-related pain.
CPD/Clinical Relevance: Clinicians should be aware of the signs and symptoms of TMD with which their patients might present and understand the complex nature of chronic pain conditions.
Article
Temporomandibular disorders (TMD) can be defined as a heterogeneous group of musculoskeletal disorders involving the temporomandibular joint (TMJ), masticatory muscles, and associated structures, characterized by pain and functional limitations in the orofacial region.1,2 It is a complex condition, influenced and affected by a variety of factors, with a wide spectrum of possible disorders and diagnoses.
This six-part series aims to explore the various aspects of TMD beginning with the patient presentation and diagnostic process, through the various forms and methods of management, non-surgical, pharmacological and surgical, that may be employed in isolation or in conjunction with one another. The aims of this paper are to discuss the anatomy of the TMJ and the epidemiology of the disorders, to describe the clinical features that a patient may present with, and to guide the practitioner through the diagnostic process.
Anatomy
The temporomandibular joint is an atypical synovial joint that permits a hinging movement and a gliding motion of the surfaces.3 The left and right condyles articulate with the temporal bone but are unable to move independently of each other.3 The TMJ shares some commonalities with other synovial joints such as a disc, fibrous capsule, fluid, synovial membrane and ligaments. However, the features that make the TMJ unique are its articular surface covered by fibrocartilage rather than hyaline cartilage.4
The anatomy of the joint can be considered in three parts: the joint; the ligaments; and the muscles.
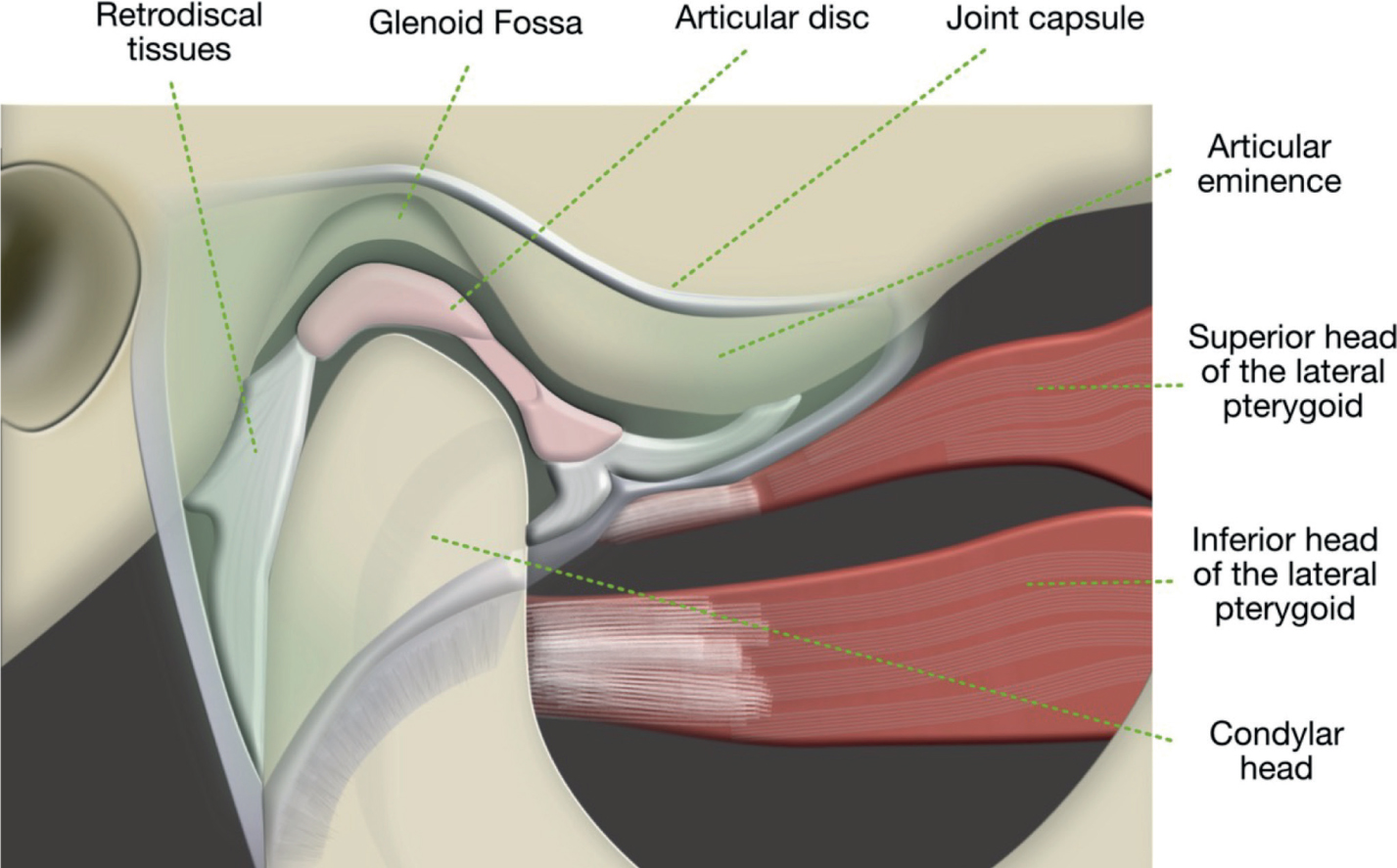
The two articular surfaces, the condylar head and the glenoid (mandibular) fossa, which are lined by a synovial membrane, never actually come into contact with one another. They are separated by the articular disc which divides the joint into two spaces, superior and inferior. The articular disc is a biconcave fibrocartilaginous structure that functions to accommodate the hinging and gliding actions of the condyle. The disc itself is described as having two bands, anterior and posterior. The anterior band attaches to the joint capsule and the superior head of the lateral pterygoid. The posterior band attaches to the fossa and is referred to as the retrodiscal tissue. Unlike the disc itself, the retrodiscal tissue is highly innervated and vascular. As a result, it is often a major contributor to the pain experienced in some disc dysfunctions4.
The fibrous capsule is a dense fibrous connective tissue that completely surrounds the joint. It attaches to the articular eminence, the articular disc and the condylar neck.5
The ligaments
There are several ligaments that act to provide stability and proprioception to the TMJ. The main three are the temporomandibular ligament (collateral ligament), the sphenomandibular ligament and the stylomandibular ligament.
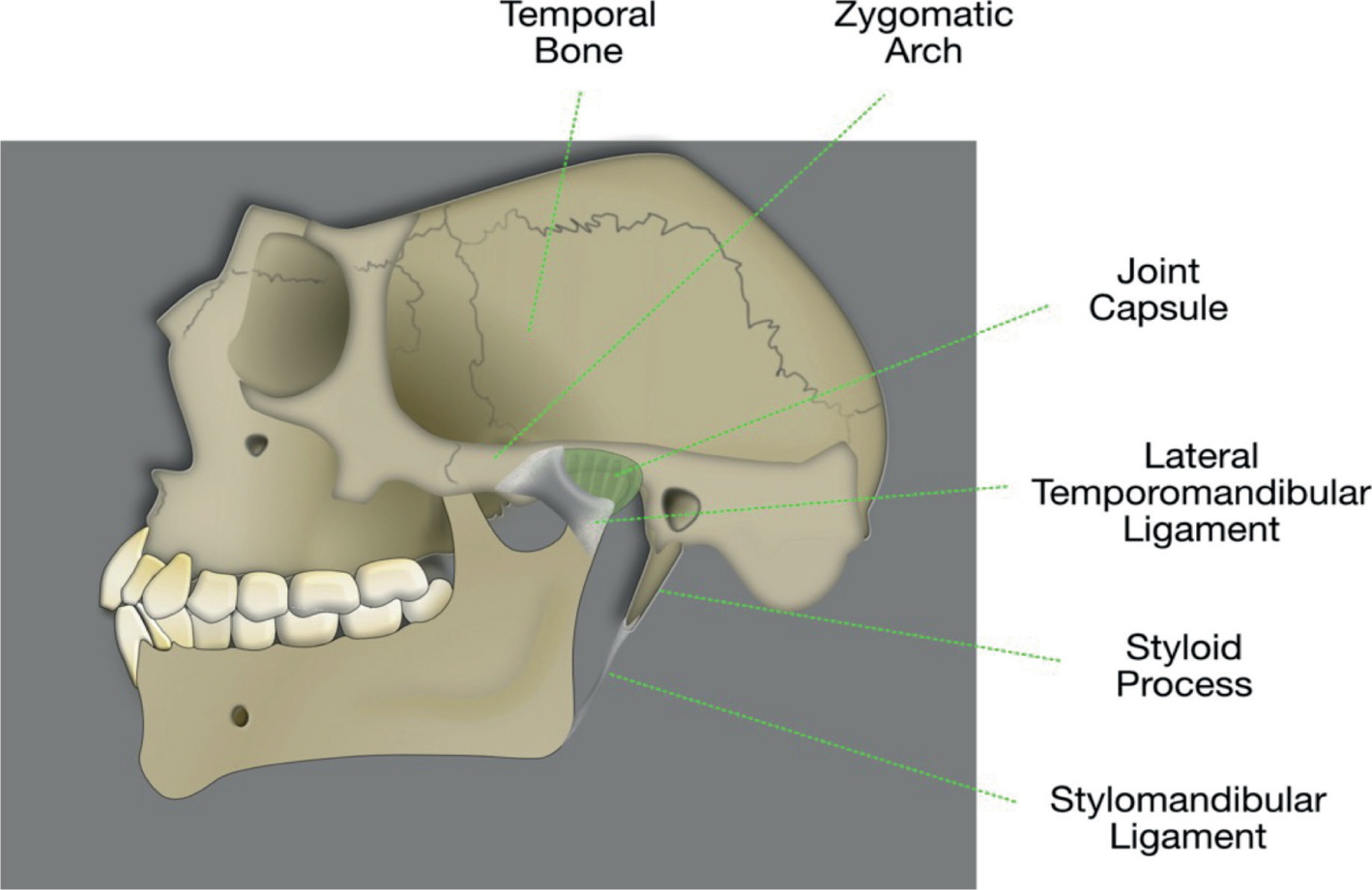
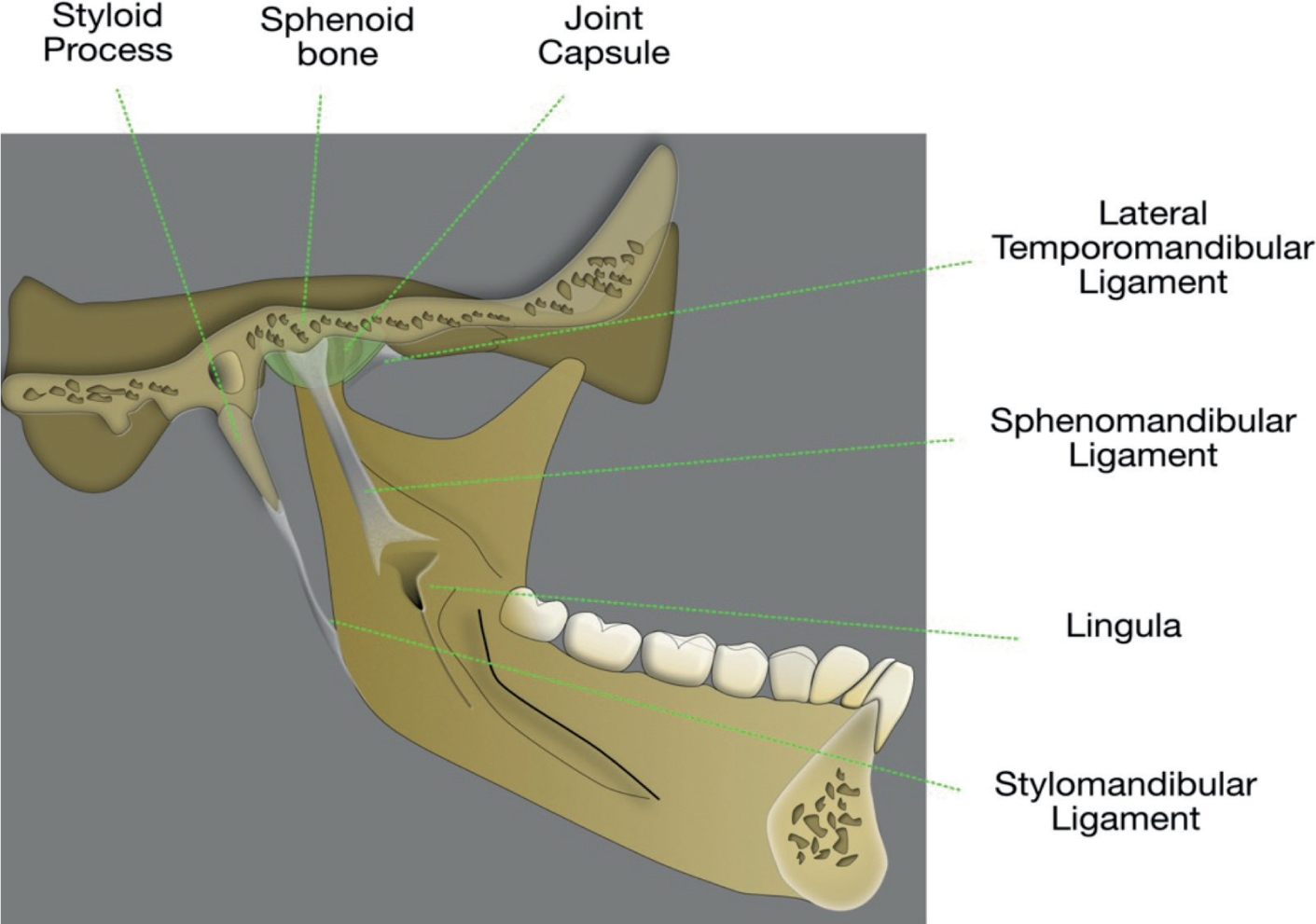
The temporomandibular ligament arises from the outer surface of the articular eminence and inserts into the neck of the condyle. It anchors the disc to the condyle and prevents posterior dislocation of the joint (Figure 2). The sphenomandibular ligament (Figure 3) originates from the sphenoid spine, and inserts into the lingula of the mandible. It helps to prevent excessive translation of the condyle. The stylomandibular ligament (Figure 3) arises from the styloid process of the temporal bone and inserts into the angle of the mandible; its function is unclear.4
Figure 2. Lateral view of the mandible showing the attachment of the temporomandibular and stylomandibular ligaments.Figure 3. Medial view of the mandible showing the attachment of the sphenomandibular and stylomandibular ligaments.
The muscles and movements
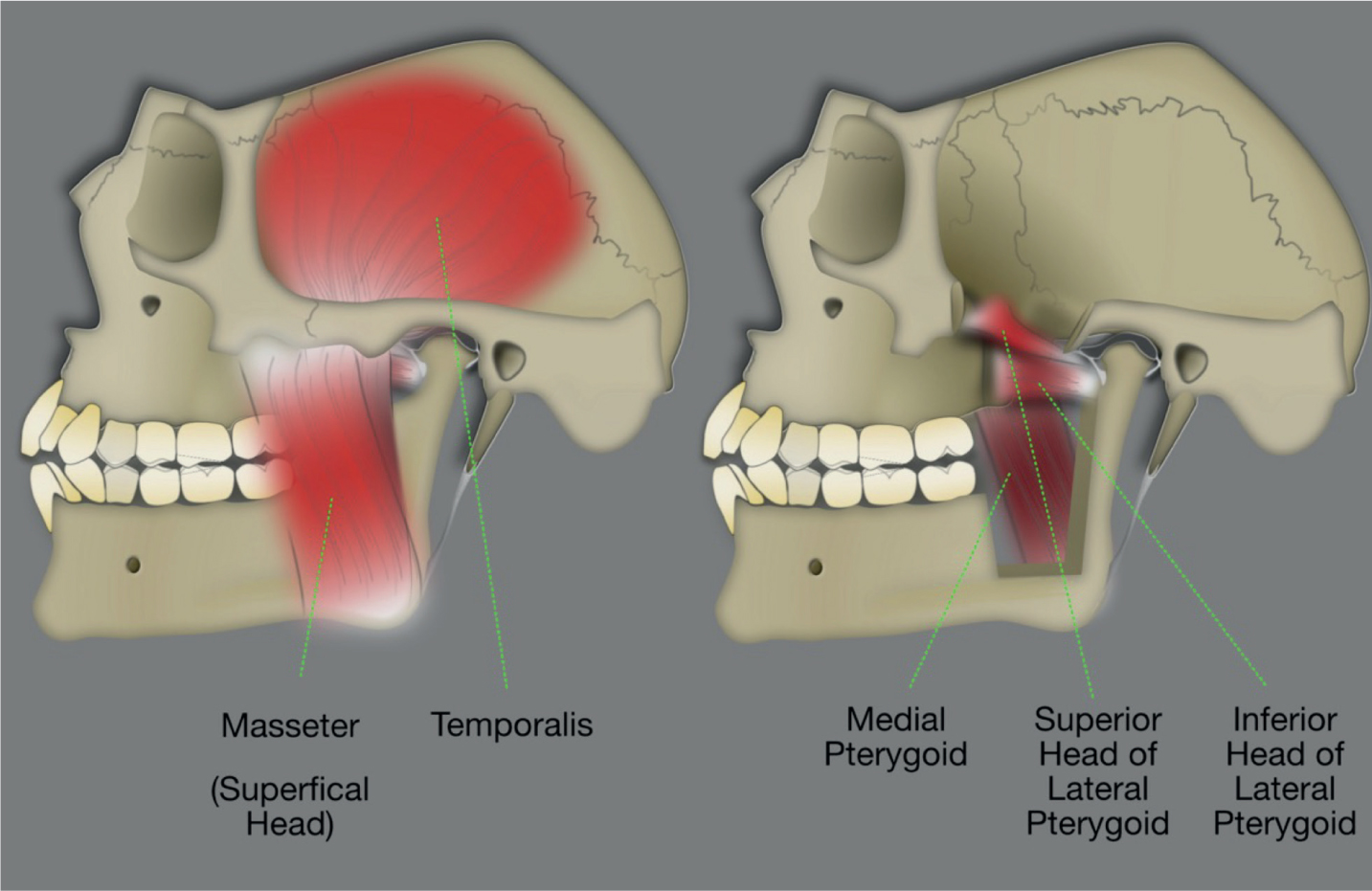
Movements of the TMJ are produced by the muscles of mastication and the supra- and infra-hyoid muscles. Their actions are summarized in Figure 4 and Table 1. The muscles of mastication are the primary depressors (opening) and elevators (closing) of the mandible. They are also used to produce protrusive and lateral movements.4
Figure 4. Anatomy of the muscles of mastication.
Muscle
Origin
Insertion
Action
Masseter
Zygomatic arch
Angle of mandible
Closing
Temporalis
Temporal fossa
Coronoid process
Closing
Lateral pterygoid
Sphenoid bone (superior belly)Pterygoid plate (inferior belly)
Pterygoid bone (deep head)Pyramidal process of palatine bone (superficial head)
Medial angle of mandible
ClosingProtrusion
Epidemiology
TMD constitutes the third most common musculoskeletal pain complaint, behind chronic back pain and headaches, and are the most common causes of chronic pain in the orofacial region.6 The reported prevalence of TMD is between 5–50% as the majority of patients do not report or seek help for their symptoms, with peak incidence occurring in the second and third decades.6,7 The prevalence appears to be only marginally higher in females in the general population,8 rising to 4: 1 in a clinical setting, as females are more likely to seek advice and treatment.6 TMD can be associated with other chronic pain conditions such as fibromyalgia and chronic pain syndrome. In addition, they are often comorbid with bruxism, depressive illnesses and chronic fatigue.9,10
TMD has a significant impact on an individual's daily activities, psychosocial functioning and quality of life that is difficult to quantify. Furthermore, chronic pain has significant cost implications for patients, the health service and the economy.11 Individual responses to pain vary considerably, but for those living with chronic pain as a permanent feature of their lives, its effects on psychosocial wellbeing can be far reaching.12
Understanding the complexities of TMD pain and manifestations is best explained by the biopsychosocial model of pain, which recognizes the dynamic interaction of the biological, psychological and social components of pain.13 First introduced by Engel in 1977, the model proposes that the concept of chronic pain cannot be broken down into discrete physical or psychosocial elements. Rather, it is the interwoven relationship between these elements that is seen to modulate the individual's perception of pain and resultant disability.14
Aetiology
The cause of TMD is complex and multifactorial in nature, with interaction of different biological and psychosocial factors.13 In isolation, factors may be considered as predisposing, precipitating or perpetuating, although it is difficult to make such distinctions in reality.15 Review of the evidence shows that the multifactorial nature of the disease involves multiple mechanisms at the level of muscles, peripheral nervous system and central nervous system. Table 2 summarizes the various factors that have been investigated in relation to the development of TMD. It is important to note that these factors help increase our understanding at a population level, but do not always explain the experiences of the individual.16
Strength of supporting evidence
Factor
Strong
Moderate
Weak–none
Psychosocial
Catastrophizing
Depression
Stress
Cognitive coping abilities
Sleep disorders
Personality disorders
Comorbidities
Fibromyalgia
Headache
Chronic back pain
Chronic pain syndrome
Irritable bowel syndrome
Nervous system
Altered pain regulation
Autonomic nervous system
Peripheral/central sensitization
Functional
Parafunctional habits
Genotype/phenotype
Gender
Genotype
Ethnicity
Age
Trauma
Dental treatment
Craniofacial trauma
Dentoskeletal
Orthodontics
Malocclusion
Psychosocial upset can be involved in the onset and perpetuation of TMD, and may also significantly impact on patient compliance with, and outcomes of, treatment.17 The inability to employ coping strategies in response to pain and the recruitment of maladaptive strategies, such as catastrophizing, have a positive correlation with increased experience of TMD-related pain.13,17,18 Depression, lack of sleep and stress-related disorders may underlie or contribute to the development of chronic TMD.13,17,18
Patients with TMD are frequently found to experience other pain-related comorbidities such as fibromyalgia, headaches, chronic back pain, and irritable bowel syndrome.17,19,20 There are indications that these comorbidities share similar altered pain regulation features and psychosocial risk factors with TMD.17 Furthermore, patients with TMD have been shown to have lower pain thresholds at the site of pain and at other sites. This suggests both peripheral and central pain sensitization.7
The relationship between TMD and parafunctional habits (bruxism and clenching) has historically been reported as a significant cause and effect relationship. However, the association between them is highly inconsistent.17 The literature is unable to demonstrate a dose–response between bruxism and TMD because most bruxists do not report intense levels of TMD pain.21,22 However, this is not to say that parafunctional activity is not of significance in some patients.
Similarly, occlusal interferences, malocclusions and orthodontics seem to be of minor importance in the aetiology of TMD.23 No consistent pattern between occlusal variables and TMD have been shown,17 in fact, there is some evidence to suggest that it is the adaptive capacity of the patient in relation to occlusal changes that influences the development of TMD.24 Similarly, the possibility that orthodontic treatment may lead to the initiation or deterioration of TMD, or that orthodontic tooth movement can be used to improve TMD, has been refuted by scientific evidence.25
Trauma, in the form of macrotrauma to the head and neck (eg head injury), or microtrauma (eg dental treatment) may contribute to the development of TMD in predisposed patients.26 Acute myofascial pain following a dental intervention from direct muscle damage or stretch injuries can be managed conservatively if the intervention is early.17 However, chronic TMD can develop if inflammatory or degenerative changes occur and the patient has other biopsychosocial risk factors.26
Clinical features
Presenting symptoms
Patients with TMD may present with any or all of the following signs and symptoms:
Pain in one or more of the muscles of mastication-localized or generalized; with or without radiation;
Pain in the TMJ produced by palpation or jaw movements;
Clicking, popping or crepitus of the TMJ, with or without locking;
Decreased mouth opening with or without interference with eating;
As with any presenting complaint, a full history, including a pain history, and examination should be undertaken. The history should capture the onset and progression of the patient's symptoms and any relevant risk factors.16
An up-to-date medical history may provide evidence of TMD pain as part of a widespread pain condition or other related comorbidities.28 Given the multifactorial biopsychosocial nature of TMD, an investigation into the patient's social history is important. While the GDP is not expected to conduct a full psychological assessment, by lending a sympathetic ear, the practitioner may be able to glean information that is relevant to the TMD diagnosis and management.16
Brief screening tools are available to help practitioners correctly identify those patients who might benefit from more formal assessment for anxiety and depression. The Public Health Questionnaire 4 (PHQ-4) is an ultra-brief screening instrument that provides responses to two questions related to depression, and two questions related to anxiety, on a Likert scale. Based on the outcome of the questionnaire, the clinician should discuss onward referral to the patient's GP for further assessment.29
Sleep
Sleep and pain perception are both critical biological functions that ordinarily operate together in a well-orchestrated physiological balance.30 The relationship between sleep and pain is complex, but current clinical and experimental evidence supports a bidirectional, dynamic and reciprocal relationship between the two.30,31 Disturbed sleep is a recognized risk factor for pain20,30,32 and similarly, chronic pain has been evidenced as a risk factor for sleep disturbance.30
The role of sleep-disordered breathing conditions, such as obstructive sleep apnoea (OSA), in the initiation or persistence of TMD are not fully understood, but current evidence suggests that there is an association between TMD and OSA.20,33
During history-taking the clinician may choose to ask about sleep quality and tiredness, or the patient may report poor sleep. Given the association between OSA and TMD, and the potential harmful and serious consequences of OSA and daytime sleepiness, these patients may benefit from screening for sleep-disordered breathing conditions and onward referral. The Epworth Sleepiness Scale is a validated assessment tool for this. Scores have been shown to correlate significantly with results from objective sleep measurement studies.34
Articulatory system examination
The TMJ should be palpated bilaterally at its lateral pole, and any pain noted, as well as any joint sounds and the range of movement. A stethoscope placed directly over the TMJ may be useful for hearing joint sounds. Maximum mouth opening less than 30 mm is a ‘red flag finding’ and should be investigated further.16 Other worrisome findings that may come to light during the history and examination are listed in Table 3. Onward referral and investigation is warranted because they may indicate the presence of a more sinister pathology.1,16
The presence of muscle tenderness of the temporalis, masseter and lateral pterygoid should be noted. The temporalis and masseter should be manually palpated and the lateral pterygoid should be assessed by the resisted movement test.16
Intra-oral examination of the patient's occlusal scheme should be undertaken, as well as a hard and soft tissue assessment to reveal any signs of parafunctional activity, such as excessive tooth surface loss (attributable to attrition), evidence of tooth or restoration fracture, tongue scalloping or frictional keratosis/linea alba of the buccal mucosa.16
The Research Diagnostic Criteria for TMD (RDC/TMD) was originally published in 1992 and more recently updated in 2014 to the DC/TMD (Diagnostic Criteria for TMD).27,35 It provides a standard and operationalized evidence-based manner in which to examine the articulatory system (axis 1) and to screen for psychosocial comorbidity (axis 2).1,35 The complete assessment tool is highly detailed, but a six-item self-complete screening tool for painful TMDs was developed in tandem with DC/TMD. This has been found to have 99% sensitivity and 97% specificity for correct identification of the presence or absence of TMD and therefore may be of use in a busy general practice.36
Imaging
The role of imaging in the diagnosis and management of TMD is generally adjunctive to the clinical diagnosis as opposed to a definitive diagnostic tool.16 For most patients, imaging is not required.
Where there is suspected bone pathology, the initial imaging modality of choice should be plain radiography, normally a panoramic radiograph (sectional, if appropriate).37 Acute fractures, dislocations and severe degenerative disease are often visible in this way.38 Computed tomography, traditional or cone beam, is superior to plain radiography in detecting more subtle bony changes.39
Magnetic resonance imaging (MRI) is the optimal modality for comprehensive joint assessment, allowing detailed examination of the soft tissues. MRI should be reserved for specific cases where:
Symptoms are persistent, non-improving or worsening;
Conservative therapy has been ineffective;
Obstructive internal joint derangement is suspected.39
Before considering the use of any form of imaging, it is important to remember that in a significant proportion of cases there will be no visible pathological anatomical changes, and therefore the use of ionizing radiation must be justified given that it may have no effect on the patient's management. Furthermore, some changes noted on imaging are not always of clinical relevance, especially if function is not affected.16,39 For example, flattening of the condylar head or increase in joint space.
Diagnosis and classification
The DC/TMD identifies three main diagnostic groups:2
Muscle disorders
Local myalgia
Myofascial pain
Myofascial pain with referral
Disc displacements
Disc displacement with reduction (reproducible click)
Disc displacement without reduction, with limited opening (limited opening, no clicking)
Disc displacement without reduction, without limited opening history of previously limited opening)
Other joint diseases
Arthralgia (painful TMJ, no crepitus)
Osteoarthritis (painful TMJ with crepitus)
Osteoarthrosis (non-painful TMJ with crepitus)
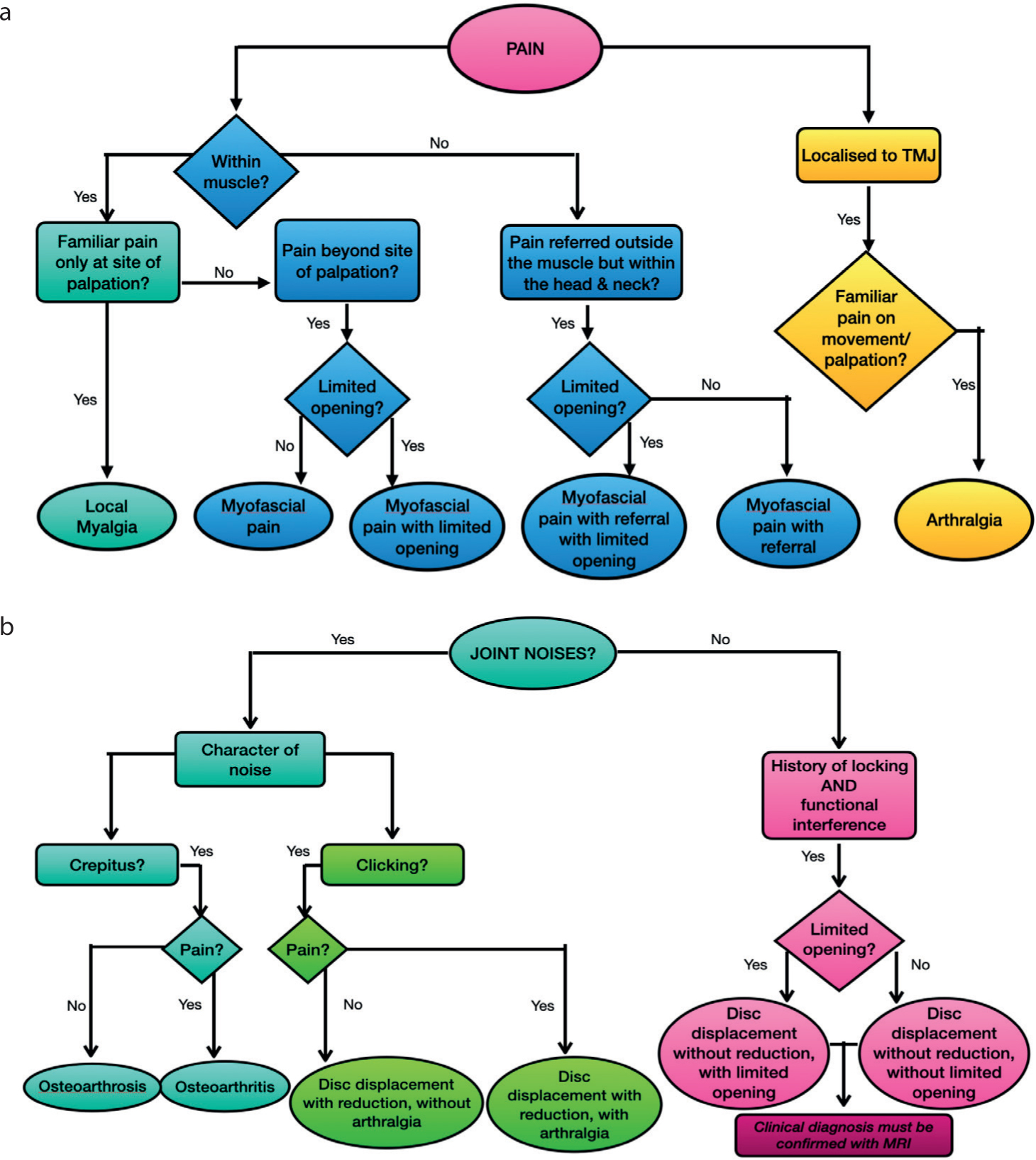
Myofascial pain tends to be the most common presenting diagnosis of a painful TMD. Disc displacements with reduction (clicking joints), with or without pain, are also common complaints. Non-reducing disc displacements are less frequent. Where there is pain in the TMJ without myalgia, and because the cause of pain is difficult to distinguish (eg synovitis, capsulitis, retrodiscitis), it is termed arthralgia. Crepitus with and without pain can indicate degenerative diseases such as osteoarthritis and osteoarthrosis, respectively16. It is also important to note an individual may present with multiple diagnoses at any one time.
The flow diagrams (Figure 5) may help the practitioner to arrive at a diagnosis and implement the appropriate management.
Figure 5.
(a,b) TMD diagnostic tree.1
Acute and chronic TMD
It is important to differentiate between acute and chronic TMD, as it influences the resultant management plan16.
Acute TMD often has an identifiable cause, such as a stressful life event or mechanical trauma (eg localized myofascial pain with limited opening following a difficult lower third molar extraction). It is often of short duration and self-limiting, and normally resolves following rest, a soft diet and simple analgesia.1.
Chronic TMD relates to pain that normally exceeds 3–months duration. The pain may become biopsychosocially destructive, result in depression, or the development of chronic pain behaviours and disability.16
It is therefore important to prevent acute TMD from becoming chronic by identifying patients who are more at risk of developing chronic pain. Potential vulnerabilities and comorbidities may include female gender, more widespread non-specific symptoms, existing psychosocial diagnoses (eg anxiety and depression), and high pain intensities.7,10,18
Conclusion
Temporomandibular joint disorders represent the most common orofacial pain conditions, and can have an overwhelmingly negative impact on an individual's psychosocial wellbeing. They contribute to the high economic burden of managing and living with chronic pain. The accepted biopsychosocial pathophysiology of the disease and significant associations with other chronic pain conditions suggest that early detection and a holistic management approach, which encourages self-management and development of coping mechanisms, can offer good long-term outcomes. The general dental or general medical practitioner are often the first people to whom a patient experiencing TMD will present, and as such, it is hoped that the primary care practitioner will be able to recognize the various TMDs, the associated risk factors and instigate timely management or referral, in keeping with the evidence presented in this series.