Banerjee A, Watson TF. Essentials of minimally invasive operative dentistry, 10th edn. In: Banerjee A, Watson TF (eds). New Delhi, India: Oxford University Press; 2016
Khandelwal P, Hajira N. Management of oro-antral communication and fistula: various surgical options. World J Plast Surg. 2017; 6:3-8
Mathews J, Ramamoorthy L, Chandrashekar L. Use of a dental mirror in the examination of oral pemphigus. J Am Acad Dermatol. 2021; 84:e71-e72 https://doi.org/10.1016/j.jaad.2019.10.047
Rieuwpassa IE, Rizal EP, Muis A, Lala HH. Three in one dental mirror: innovation of oral diagnostic instrument. J Dentomaxillofac Sci. 209; 4:75-78 https://doi.org/10.15562/jdmfs.v4i2.943
Oncel M, Apiliogullari B, Cobankara FK, Apiliogullari S. Accidental swallowing of the head of a dental mirror: report of a rare case. J Den Sci. 2012; 7:199-202
Dumbrigue HB, Gurun DC. Use of intraoral photography mirrors as aids for evaluating parallelism of multiple abutment preparations. J Prosthet Dent. 2001; 85 https://doi.org/10.1067/mpr.2001.112798
Technique Tips: A Reflection on Mouth Mirrors: Types, Usage and Modifications Debolina Bishayi Kavya Suvarna Surmayee Singh Arindam Dutta Manuel S Thomas Dental Update 2024 50:9, 707-709.
Authors
DebolinaBishayi
BDS
Manipal College of Dental Sciences, Mangalore, Manipal Academy of Higher Education, Manipal, Karnataka, India
Department of Conservative Dentistry and Endodontics, Manipal College of Dental Sciences, Mangalore, Manipal Academy of Higher Education, Manipal, Karnataka, India
The mouth mirror is an essential tool in the dental armamentarium. Among its many functions, the most significant is being able to visualize aspects of the oral cavity that are not accessible visually with an appropriate operator posture. Various mouth mirrors are available and can differ in their design, head size and reflective surface. While in use, clinicians may encounter multiple circumstances that can hamper the quality of the reflected image. This in turn can negatively influence the diagnosis and treatment delivered. Hence, the purpose of this Technique Tip is to provide information on various designs of mouth mirrors as well as to provide solutions to counter the challenges associated with the use of mouth mirrors.
Clinical relevance: Sharp, bright, reflected images may be provided for dental clinicians using simple methods and other equipment associated with the mouth mirror.
Article
The clinical practice of dentistry requires precision in a restrictive environment, with tissues that may interfere with the clinician's access and visibility. A basic yet very important tool that assists the clinician in visualizing and accessing the oral cavity, whilst maintaining appropriate operative posture, is the mouth mirror.1 Mouth mirrors were introduced in the early 19th century.2 The earliest mouth mirrors were made of highly polished bronze.3 Since then, this widely used instrument in dentistry has evolved and the purpose of this Technique Tip is to provide an overview of the mouth mirror, highlighting various types, their functions, and clinically significant applications of different mouth mirrors available to dental practitioners.
Parts of a mouth mirror
Mouth mirrors, also rarely referred to as odontoscopes or stomatoscopes, have three main parts:
Working end;
Shank;
Handle.
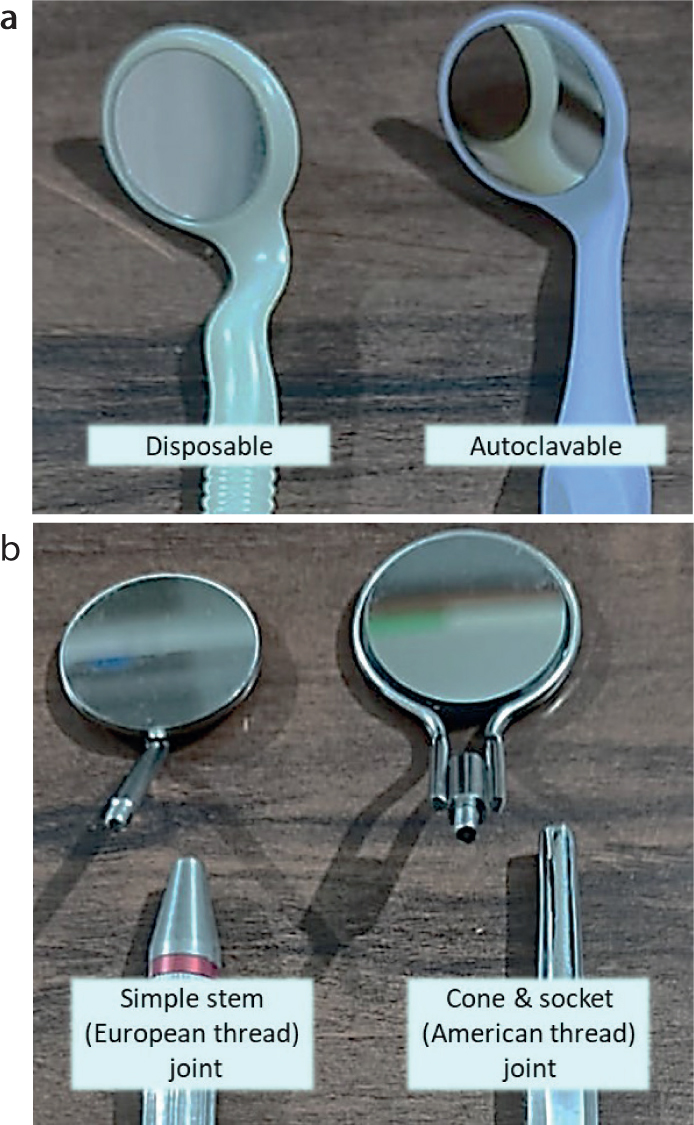
The shank of the mirror connects the working end (rimmed mirror) with the handle. A mouth mirror can be manufactured either as a single unit (the non-detachable mouth mirror) or, alternatively, with the working end attached to the shank, which in turn is detachable from the handle. The non-detachable mouth mirrors, where the rim, shank, and handle are made of polymer, are either disposable or autoclavable (Figure 1a).
Detachable mouth mirrors are usually comprise a metal shank that can be removed from the handle. This feature is useful since the working end can be replaced when the quality of the mirror deteriorates after repeated use, disinfection and sterilization. The joints in these detachable mirrors can be categorized as either simple stem (European thread) or cone and socket (American thread) (Figure 1b).4 The mouth mirror handle can be made of metal with serrations in the grip area to prevent slippage. Silicone handles, which are lighter than metal-based handles, are now available with ergonomic designs. They reduce hand fatigue and improve operator comfort.5,6
Working end classifications
The working end can be classified on the basis of several parameters, such as the shape, size and the nature of the reflective surfaces. The head of a mouth mirror is usually round, but tear-drop, oval and rectangular shapes are also available. Round mirrors can be subcategorized by size. For example, size number 0 is 14 mm, and the size increases incrementally in diameter by 2 mm, with each increase in size until size 8. Sizes 9 and 10 measure 40 mm and 55 mm, respectively. The most commonly used sizes are number 4 and number 5.4,7
Based on the location of the reflective surface on the mirror, they are classified as rear surface mirrors or front surface mirrors. A rear surface mirror has a waterproof reflective coating on the rear surface of the glass (Figure 2a).4 A rear-facing mirror can be identified by placing a gloved finger or any object touching the mirror surface and noticing a gap between the finger and the image (Figure 3a).8 Although mirrors with a reflective coating on the back side can cause image distortion and a double image, they are less prone to deterioration from scratches.
Figure 2. (a) Rear surface mirror with a reflecting surface on the back of the glass results in refraction of incident light, leading to image distortion. (b) A front surface mirror with a single reflection at the top of the surface provides a sharp image.Figure 3. (a) Plane rear surface mirror having flat reflecting surface on the back of the glass. (b) Concave rear surface mirror showing slightly enlarged but distorted image. (c) Front surface mirror with reflecting surface at the top surface showing crisp image. There is no gap between the object and the image in the front-facing mirror, unlike the rear-facing mirror.
The reflective surface of a rear surface mirror can be plane or concave.4 Flat or plane surface mirrors are preferred because they provide a clearer image.1 Concave mirrors, on the other hand, are used to magnify the image (Figure 3b).4 It makes the visible area look larger, which can help with inspection and to provide a better image of the area for diagnosis, but the concavity also causes image distortion.
The front surface mirror has its reflecting surface at the top of the glass with respect to the path of light (Figure 2b).4 These involve only a single reflection (avoiding refraction of the light, which is inevitable in rear reflecting surfaces), resulting in an exact, sharp image with no ghost image or distortion (Figure 3c). Some front-surface mirrors have rhodium plating and these mirrors are said to provide a bright, sharp, distortion-free image. Another variety of front surface mirrors is the crystal mouth mirror, which, as per the manufacturers, is 40% brighter than a rhodium-coated mirrors because it has 43 layers of metal oxide.9 However, such mirrors are also prone to rapid deterioration of the reflective surface, especially damage sustained by scratching.10
The need for mouth mirrors
The mouth mirror is a basic tool used to see inaccessible areas of the oral cavity, enabling better diagnosis and treatment (Table 1). It is a basic tool needed to clearly see the inaccessible areas within the oral cavity, enabling better diagnosis and treatment.7 In addition, a mouth mirror also enables a better ergonomic position for the operator, thereby preventing occupation-related musculoskeletal injuries.7
Table 1. Uses of a mouth mirror.
Part
Purpose
Reflective surface
Indirect vision
Illumination/transillumination
Intra-oral photography
Handle
Percussion testing
Checking tooth mobility
Contouring matrix bands
Head
Cheek/tongue retraction
Identification of hyposalivation
Identification of oro-antral fistula
Apart from indirect vision, the mouth mirror held in the non-dominant hand acts as an extension of the dentist's fingers to aid in soft tissue retraction (Figure 4). Carefully retracted cheek or lips, or even the tongue, will improve the clinician's visibility during clinical examination and subsequent treatment procedures.10 Soft tissue retraction is important while performing operative procedures with high-speed rotary cutting instruments to prevent iatrogenic injury.
Figure 4. Various uses of mouth mirrors.
Additionally, mouth mirrors can reflect the light available from an external source to illuminate the area of interest intra-orally for better visibility.4 The reflected light from the dental mirror can also be used for transillumination to visualize hidden proximal caries and fracture lines, especially in the anterior teeth. The back end of the handle of a mouth mirror has also been traditionally used to contour relatively flat matrix bands to simulate proximal contours before restoring posterior teeth.
The end of the mouth mirror handle may also be used for percussion testing. This is done to determine the inflammatory status of the apical periodontium. Gently pressing the end of two mouth mirrors on the buccal and lingual surface of a tooth is also used to assess the mobility of teeth (Figure 4).11 The temporary adhesion of a mouth mirror to the buccal mucosa or tongue has been suggested by Osailan et al as a sign for the identification of hyposalivation.12 Mouth mirrors have also been recommended to clinically detect the presence of oro-antral communication. Holding a mouth mirror near the opening of oro-antral communication can cause fogging of the mouth mirror.13
Challenges associated with the use of mouth mirrors
One of the most common difficulties faced by a dentist while using a mouth mirror is partial or full image obscurity that might be caused by fogging, droplet retention, scratches or image distortion (Table 2).
Table 2. Challenges associated with the use of a mouth mirror.
Problems
Recommendations
Fogging
Use defogging sprays
Warming the mirror
Using a rubber dam
Droplet retention
Cleaning with surfactant solution
Wetting the mirror surface
Scratches
Use of disposable mouth mirrors
Separate packing while autoclaving
Use of mirror cover
Semi-critical item
Autoclave or dispose to avoid cross-contamination
Image distortion
Avoid using rear reflecting or convex mirrors
Reduced image brightness
Use of mirrors with a high-quality reflective surface
Operator hand fatigue
Appropriate finger rests
Ergonomically designed handle. For example, a thicker handle made of a lightweight material such as silicone
Patient discomfort
Gentle retraction of soft tissues
Avoid resting the head of the mirror on the alveolar surface
Warming a mouth mirror on the patient's buccal mucosa or using warm water brings the temperature of the mirror closer to that of the patient's oral cavity and this can reduce fogging.14 Defogging sprays, which contain surfactants, reduce the surface tension of the mirror surface and thus prevent the condensation of water to reduce fogging.7 Another issue that interrupts the dentist's treatment is droplet retention and debris accumulation.15 By using surfactant solutions that contain sodium dioctyl (Mirror Magic Anti-Fog solution, Zirc Dental Products, Buffalo, MN, USA) and angling the mirror vis à vis the position of the high volume suction, or additionally, even the mirror being wiped by a dental assistant, this problem can be mitigated to an extent.
Scratches on mirror surfaces are another common occurrence, specifically after multiple uses. This affects the clarity of the reflected image on the mirror. Fresh disposable mouth mirrors can be used for each patient to reduce this problem. However, these disposable mirrors are an environmental concern, especially when the dental profession is adopting more sustainable and greener strategies in practice. Clinical procedures where the mirror may be scratched and the need for extreme detail and accurate visualization is low, such as during intra-oral air abrasive procedures, rear-reflecting or disposable mirrors can be considered.16
Since mouth mirrors are semi-critical items, the reusable mirrors must be cleaned and autoclaved. While autoclaving, failing to separate them physically in the sterilization tray can contributor to mirror scratches, hence care must be taken during decontamination.8,17 When cleaning, disinfecting or storing mouth mirrors, a mirror cover (Mirror Gear Mirror Covers, USA) may also be used to protect them from scratches.18
Image distortion, as well as secondary or ‘ghost’ images of lesser intensity than the principal image might be visible is a problem encountered with a rear reflecting mirror.4 This issue can be tackled using mouth mirrors with a high-quality reflective surface on the front.
Another very rare, but serious, complication reported in the literature is the ingestion/aspiration of the mouth mirror head.19 The integrity of detachable metallic mouth mirrors should therefore always be checked. Detachable mouth mirrors with loose threading that cannot be tightly secured on the handle, and those with defective solder joints at the head–shank junction, need to be replaced.
Dental lasers are used for procedures, such as soft tissue biopsy, gingivoplasty and crown lengthening, among others. Inadvertent refection of a dental laser during such procedures from a mouth mirror can cause ocular damage. Therefore, care should be taken to avoid such incidents. According to the Medicines and Healthcare products Regulatory Agency, dental lasers should be used only in designated controlled areas. All personnel and patients in the controlled area should be advised to wear protective eyewear when using dental lasers.20
Advances in mouth mirror technology
Mouth mirror with varying designs
Microsurgical mouth mirrors are defined as mirrors that have extremely small head sizes (Figure 5a). These microsurgical mirrors are used during peri-radicular microsurgery, such as during root-end surgery and surgical repair of iatrogenic or resorption-associated perforations.21 Microsurgical mirrors are also available with several different shapes.
Figure 5. Advanced mouth mirrors. (a) Microsurgical mirror with a diameter of 3 mm as compared to a regular number 5 mirror that is 24 mm in diameter. (b) Self-cleaning mouth mirror by use of controllable air flow (courtesy of DHM-Dental). (c) Mouth mirror with light (courtesy of Smart Mirror Dental).
Reverse-angle mouth mirrors have a standard mirror surface that makes an outward 45° angle with the stem, in contrast to the standard mirror where the mirror surface and stem form a 45° inward angle. Therefore, along with cheek or tongue retraction, indirect vision or illumination of the operative field can be achieved.22
Self-cleaning mouth mirrors
Self-cleaning mirrors prevent debris or water spray from smearing the surface of the mouth mirror, hence additional procedures such as cleaning the surface glass repeatedly are not required. The benefits of these self-cleaning mouth mirrors include, but are not limited to, improved vision and time efficiency during operative procedures as the need to clean/wipe the reflective surface is eliminated.
Yirro-plus mirror (DHM-dental BV, Arnhem, Netherlands) is a mouth mirror with airflow. It has an ultra-reflective surface and includes a smooth multi-layered coating, which is repellent to grease and contamination (Figure 5b). The adjustable airflow system offers a permanent clear sight. The mirror can be mounted at a comfortable location on the delivery unit using a universal adapter. The mirror heads and handles can be sterilized in an autoclave.23
Three-in-one mouth mirror is a multifunctional prototype of a mouth mirror, combining three dental instruments in one tool. It is also used as a light source. It has air and water valve components, which are placed on the foot pedal, making it convenient for rinsing and cleaning the glass of the mirror preventing debris and water spray from staining the surface of the mirror.15
EverClear (Nuview Ltd, Gloucestershire, UK) is a self-cleaning mouth mirror with a mirror head that spins when the tip of the handle is turned. Thus, centrifugal force helps keep debris and fog at bay, providing speed and convenience for uninterrupted patient care. The mirror is ergonomically balanced and powered by rechargeable batteries, hence completely cordless. However, a disadvantage would be the need to remove the batteries before autoclaving, and the extra cost to replace the batteries as and when required.24 HVE Suction Dental Mirror (GoldenDent, Roseville, MI, USA) is another patented system where the specifically designed mirror handle is connected to a high-volume evacuation (HVE) unit. The mirror has powerful suction with 20 suction holes around the mirror lens and on the back of the mirror for enhanced working visibility and isolation.25 Both these products can be sterilized by autoclaving for easy infection control.
Mouth mirror with light
Mouth mirrors with light-emitting diode (LED) lights can improve visualization in the oral cavity.26
Smart Mirror (Chicago, IL, USA) is a new-generation mouth mirror with an in-built self-adjusting camera, very high-quality LEDs, and an ultra-bright, fog-free sapphire mirror that gives a crystal-clear reflection (Figure 5c). Owing to their 5000 Kelvin (K) colour temperature and 93 colour rendering index (CRI), the LEDs imitate daylight and allow the practitioner to see the true colour of teeth. The self-adjusting camera wirelessly connects to electronic devices, such as a tablet, and provides real-time images and video at a magnification of up to 10x on the connected device. Using this technology, dentists can educate their patients about oral care by showing real-time videos on the screen. For infection control, the Smart Mirror head can be sterilized using common methods, such as autoclaving or cold sterilization.27 However, this hi-tech dental mirror is very expensive.
Intra-oral mirrors for clinical photography
Intra-oral mirrors are important accessories for dental photography and can provide a reflected image for areas with difficult access. To capture distortion-free and clear images, front-reflecting mirrors of various shapes are available. To avoid fogging, the assistant can be instructed to gently blow air across the mirror using a three-way syringe, or the photographic mirror can be emersed in warm water for a few minutes before use.28 More recently, mirror handles with micro fans and LED lights (Trueoptics Fog Free Mirror handle, Adenta Global, Germany) are available to create fast, easy and clear images.29 Intra-oral photographic mirrors have been recommended for viewing large areas, for example, when evaluating tooth preparation for the path of placement parallelism for multiple teeth or implant abutments.30
Conclusion
A distortion-free, clear reflective image provided by an intra-oral mirror will improve clinical efficiency and cause less frustration for the clinician. A thorough understanding of the types of mouth mirrors available can provide the dental clinician with means to tackle the issues associated with their use.