Odonwodo A, Badri T, Hariz A. Scleroderma.Treasure Island, FL, USA: StatPearls Publishing; 2020
Herrick AL, Ennis H, Bhushan M Incidence of childhood linear scleroderma and systemic sclerosis in the UK and Ireland. Arthritis Care Res (Hoboken). 2010; 62:213-218
Albilia JB, Lam DK, Blanas N Small mouths … Big problems? A review of scleroderma and its oral health implications. J Can Dent Assoc. 2007; 73:831-836
Salliot C, Mouthon L, Ardizzone M Sjogren's syndrome is associated with and not secondary to systemic sclerosis. Rheumatology (Oxford). 2007; 46:321-326
Alantar A, Cabane J, Hachulla E Recommendations for the care of oral involvement in patients with systemic sclerosis. Arthritis Care Res (Hoboken). 2011; 63:1126-1133 https://doi.org/10.1002/acr.20480
Laforgia A, Corsalini M, Stefanachi G Non-surgical periodontal management in scleroderma disease patients. J Biol Regul Homeost Agents. 2016; 30:847-851
Yuen HK, Weng Y, Bandyopadhyay D Effect of a multi-faceted intervention on gingival health among adults with systemic sclerosis. Clin Exp Rheumatol. 2011; 29:(2)S26-32
Yuen HK, Weng Y, Reed SG Factors associated with gingival inflammation among adults with systemic sclerosis. Int J Dent Hyg. 2014; 12:55-61 https://doi.org/10.1111/idh.12024
Hadj Said M, Foletti JM, Graillon N Orofacial manifestations of scleroderma. A literature review. Rev Stomatol Chir Maxillofac Chir Orale. 2016; 117:322-326 https://doi.org/10.1016/j.revsto.2016.06.003
Singh K, Gupta N, Gupta R, Abrahm D. Prosthetic rehabilitation with collapsible hybrid acrylic resin and permanent silicone soft liner complete denture of a patient with scleroderma-induced microstomia. J Prosthodont. 2014; 23:412-416
McKenna G, Hayes M, Burke FM. Provision of resin bonded bridgework for a patient with microstomia secondary to scleroderma. Eur J Prosthodont Restor Dent. 2012; 20:56-60
Gözde Türk A, Ulusoy M. A collapsible partial denture for a patient with limited mouth opening induced by scleroderma: a clinical report. J Prosthodont. 2015; 24:334-338 https://doi.org/10.1111/jopr.12220
Consultant in Special Care Dentistry UCLH/Honorary Senior Lecturer UCL, Royal National ENT and Eastman Dental Hospitals, University College London Hospital, London
Scleroderma is an autoimmune condition of the connective tissue. It encompasses a range of disorders that can affect the face, skin, limbs and internal organs. Common dental manifestations include xerostomia, dysphagia, microstomia, thickened and tight facial skin and tongue rigidity. This article describes how scleroderma can severely impact and compromise oral health. This can occur due to the restricting nature of sclerodactyly and microstomia seen in severe forms of the disease. Dental professionals must be mindful of this condition and its common oral manifestations. Techniques of how to recognize and manage these patients are discussed.
CPD/Clinical Relevance: The dental and oral health implications of scleroderma are relevant to clinical practice.
Article
Scleroderma originates from the Greek words sclero meaning hard tissue and derma, which means skin. It is an umbrella term for different autoimmune conditions caused by excess collagen and scarring in the tissues.
The cause of scleroderma is still uncertain; however, an autoimmune response is evident where fibroblasts produce too much collagen. Triggers for this abnormal immune response have been linked with previous viral infections, such as measles, previous radiotherapy treatment, family history of scleroderma and exposure to certain chemicals or drugs.1
Clinical presentation
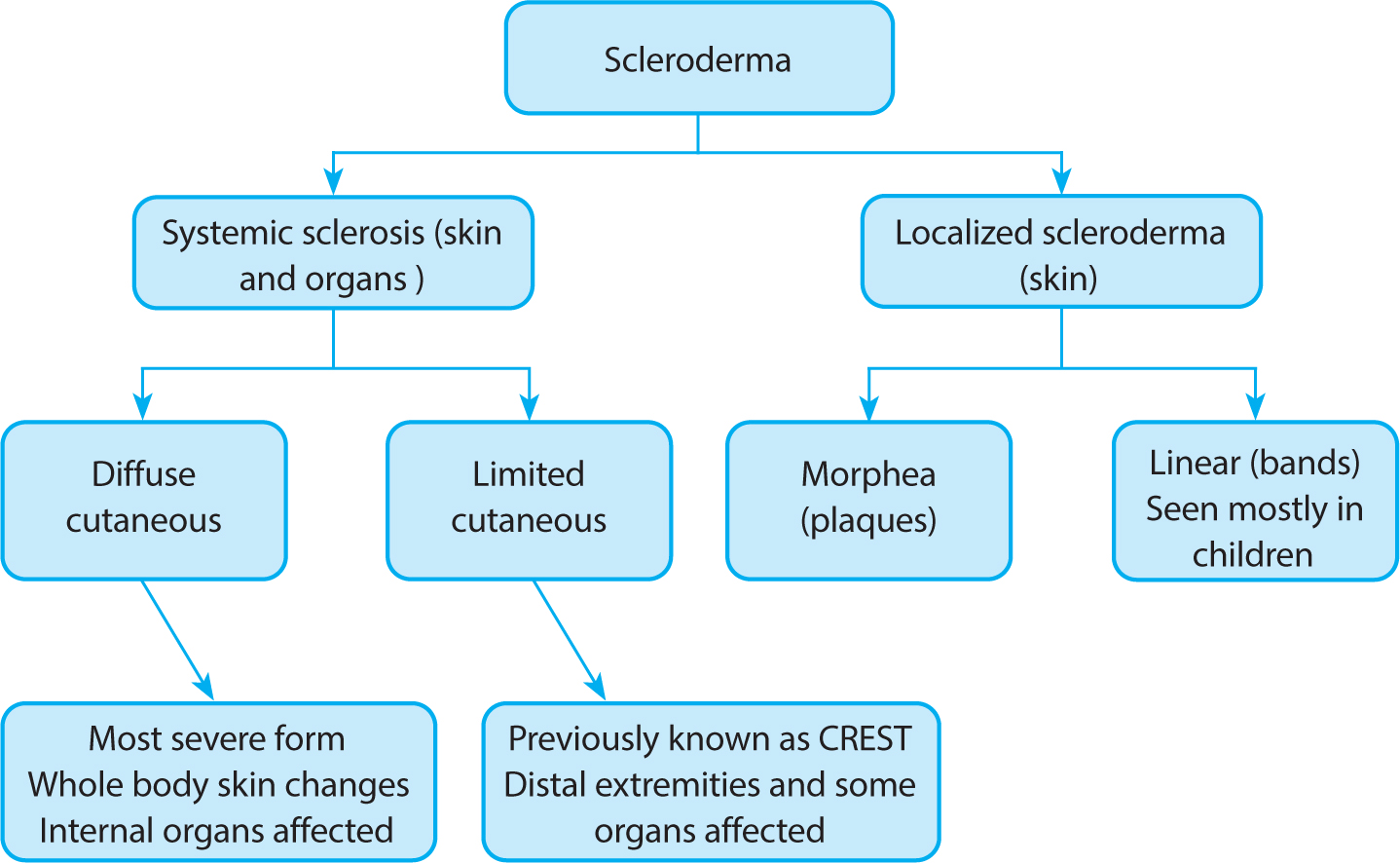
Scleroderma can be divided in to two main forms: localized and systemic. These can then be further subdivided according to severity and which parts of the body are affected (Figure 1). In localized scleroderma, the collagen deposition is restricted to the dermis and subcutaneous tissues.1 Fat, fascia, bone and muscle may be affected in this form, but internal organs are usually spared. Approximately 1300 people per year are diagnosed with the condition in the UK, with 70% of cases affecting children between the ages of 5 and 10 years. In adults, it is usually seen in the fifth decade, and affects twice as many woman as men.2 In the localized form, thickened white plaques are seen on the skin known as plaque morphea. Long-standing plaques present as brown patches on the skin. The area is often smooth, shiny, hairless and tight.3 This condition is rarely life threatening, but can greatly reduce quality of life as the patches may appear on any skin surface and patients can feel disfigured.
Figure 1. The different forms of scleroderma and which areas of the body are affected. Localized scleroderma is a milder form of the disease affecting skin alone, whereas in diffuse cutaneous systemic sclerosis, internal organs can also be affected.
Limited cutaneous systemic sclerosis was previously referred to as CREST syndrome, which encompasses the pathological signs and symptoms seen. This condition is rare and affects 3–9/100,000 people in the UK, and is seen after the fourth decade.4 It affects four times as many women as men.5 In both forms of systemic sclerosis, the skin and organs can be affected with more severe complications seen in the diffuse form (Table 1).
CREST features
Clinical features
Calcinosis
Abnormal inflammatory response causing calcium deposits within the dermis along the bones in distal extremities. Swellings appear under the skin
Raynaud's disease
Vascular changes due to blood vessel damage. Distal blood vessels vasoconstrict producing pale fingers and toes. Cyanotic appearance then appears due to hypoxia in the area followed by reperfusion and a return to normal colour
Oesophageal dysmotility
Damage to muscle layers cause abnormal contractions and acid reflux
Sclerodactyly
Fibrosis of the skin in the fingers or toes cause skin to appear hard and tight. Hands take on a ‘claw’ like appearance. Difficult to move and hold objects
Telangiectasia
Dilated or damaged blood vessels present in distal extremities due to blood vessel damage. Appear as fine red/purple lines under the skin
Tightening and scarring of tissues of the face causes limited mouth opening, and a characteristic and recognizable facial appearance seen in patients with systemic sclerosis (Figure 2). Calcinosis is often a common finding in patients and appears as hard swellings under the skin, along the bones in the hands and feet. This greatly affects movement and can be debilitating and painful (Figure 3).
Figure 2. Clinical photographs of a patient with limited cutaneous systemic sclerosis. Common orofacial findings include (a) mask-like features with widened palpebral fissures. (b) A slanting facial profile is seen with microstomia, oral cavity tissues appearing stretched and sunken lip musculature.Figure 3. Clinical photographs of hands of a patient with limited cutaneous systemic sclerosis showing severe sclerodactyly. Calcinosis is evident under the skin (top left). Movement of the hand is extremely restricted. Skin appears stretched with a characteristic ‘shiny’ appearance.
Early signs of systemic sclerosis are swellings in the distal extremities. Fingers and toes may appear ulcerated, swollen and be painful during movement (Figure 3). Raynaud's phenomenon is an early symptom of scleroderma, seen in 70% of localized scleroderma cases and 95% of systemic sclerosis patients.3 In Raynaud's, the blood vessels narrow in the distal extremities (fingers, nose and feet) and display a change in colour from white, when the vessels initially vasoconstrict, to blue, owing to localized hypoxia in the area, to red once the vessels vasodilate.5 This symptom can be triggered by cold and stress and can be painful with a sensation of tingling and numbness in distal extremities.
In diffuse cutaneous systemic sclerosis, the condition is more severe and affects internal organs and systems, including the stomach, oesophagus and lungs.6 These, in turn, can lead to further complications affecting the bowels, kidneys, bones and heart (Table 2). Renal disease can be seen in 10–15% of patients with scleroderma, and is seen in more severe forms of the disease.7 Abnormal levels of connective tissue deposition and thickening of the arterioles in the kidneys causes impaired renal function and can cause scleroderma renal crisis. This can be life-threatening owing to an imbalance of electrolytes and fluids in the body. There is currently no cure for this condition; however, it can be managed by relieving symptoms and preventing progression by taking immunosuppressant medications. Patients are routinely monitored by the medical team to ensure complications are treated early.
Internal systems involved
Complications
Gastrointestinal
Oesophageal dysmotility, acid reflux, gastroparesis, bloating, constipation or diarrhoea
Respiratory
Interstitial fibrosis of lung tissue can affect ventilation and perfusion. Damage to pulmonary vessel wall can cause pulmonary arterial hypertension. This is a serious and potentially life-threatening complication
Musculoskeletal
Pains and aches in joints and muscles affecting movement in the body. Difficulty using hands for everyday function and holding objects. Can be extremely debilitating for the patient
Cardiovascular
Pulmonary arterial hypertension due to damage to vessel wall. This can lead to cardiac abnormalities and is a life-threatening complication
Renal
Inefficient kidney function and damage causing scleroderma renal crisis and accelerated hypertension. Decreased urine output occurs, and patients may suffer from nervous system affects including fainting, dizziness, blurred vision and breathlessness. A life-threatening complication
A good understanding and a patient-specific approach can help minimize a patient's disability and improve their quality of life (Table 2).
Dental implications and management
With many significant oral symptoms, early signs of scleroderma may initially be seen by the general dental practitioner. It is important to carry out extra- and intra-oral examinations of the patient's features at every visit and record any abnormalities. Dental radiographs may show widening of the periodontal ligament without any other attributable cause in a healthy patient, which is a sign commonly seen.6
Both limited and diffuse forms of systemic sclerosis can affect oesophogeal motility. This can cause gastroesophageal reflux disease (GORD). Acid reflex due to GORD can cause palatal and lingual tooth surface loss and can be an early clinical sign discovered. Appropriate medical referral is advised to allow this symptom to be investigated as GORD can be a risk factor for other complications including pneumonia and oesophogeal cancer3.
Pulmonary disease is seen due to scarring of the alveolar tissue in the lungs, predisposing the patient to interstitial lung disease. Patients can exhibit breathlessness, dry coughs, fatigue on exertion and may require supplemental oxygen. Regular monitoring and testing is required to assess lung function for patients with severe forms of the disease. These patients may need to be seen in a hospital setting to ensure emergency equipment is available.
Systemic sclerosis has many features that make it an uncomfortable and debilitating, as well as disfiguring condition for the patient. It is important that dental professionals are mindful of the condition and how to ensure that patients feel comfortable and safe. A good understanding of the condition will improve communication and better holistic patient management. It is important to update the medical history regarding symptoms related to the condition, document any changes and seek medical advice as appropriate (Table 3).
Systemic sclerosis complications
Dental implications
Management
Raynaud's phenomenon
Patients can experience pain from digits in cold and stressful environments
Ensure clinical and non-clinical areas are not too cold, and see patient on time3,4,5,6,7,8,9Speak to patient regarding any dental anxieties
Microstomia
Difficult to access mouth for examination and treatmentTissues can be dry and be damaged during exam
Apply neutral balm to patients lips and corners of the mouthCareful tissue manipulation, do not overstretch tissues3,4,5,6,7,8Measure maximal mouth opening comfortable for patientOffer breaks during treatmentEnsure good aspiration to prevent inhalation/ingestion3,4,5,6,7,8,9
Calcinosis, sclerodactyly and tightening of skin on hands and limited joint movements
Unable to hold toothbrushUnable to brush effectively at home
Assess patients' hands and discuss options of electric toothbrush or larger sized handles to aid cleaningPatients' toothbrush can be put into putty and molded to patients grasp
Osteoporosis
Patient may take bisphosphonates
Assess patients medication-related osteonecrosis risk (MRONJ) and manage according to MRONJ guidelines20
Xerostomia
Reduced saliva predisposes patient to; dental caries, increase failure of restorations, sores in the mouth, plaque and food build up, halitosis, dysphagia and dysarthria
Fluoride therapy with emphasis on prevention3-–11Prescribe high fluoride toothpasteFluoride application 2–3 times a yearOffer water as required during consultation and treatmentMoist gauze on inner buccal mucosa when examining and lubrication on lips and corners of the mouthSaliva substitutes can be prescribed
Oesophagus dysmotility causing acid reflux
Acid reflux in the mouth causing tooth surface loss
Assessment of tooth wear and monitor at every visit11Fluoride therapyDiet adviceRestorations if appropriate
Other complications involving internal organs
Patient may have high blood pressure due to pulmonary arterial hypertension or interstitial fibrosis causing faint, dizzy or breathless symptomsUnderactive thyroidHeart complicationsBowel obstructionGastrointestinal abnormalitiesKidney dysfunction
Liaise with medical team regarding the severity of the patient's condition.Referral to secondary care if hospital setting required to allow for any complications to be managed
Most patients with systemic sclerosis have a moderate or mild form of the disease. Severe forms of the condition may require referral to secondary care. The condition can be stable and unstable at different times, thus regular monitoring and updating the medical history is important.
Symptoms of skin tightening can be managed with a balm applied to the skin and lips and corners of the mouth before and after dental exam and treatment. Patients with Raynaud's are often seen wearing gloves and multiple layers in non-clinical areas to ensure the pain in the digits is minimized. It is important dentists ensure that non-clinical and clinical areas are not too cold, and stress is minimized by seeing patients on time and establishing good open communication to alleviate any dental anxiety.3,4,5,6,7,8,9,10,11
Long-term steroid use can increase the risk of an Addisonian crisis due to suppressed cortisol production. The dentist must be aware of the complications of long-term steroid use and liaise with the medical team about appropriate steroid dose supplementation before and after dental treatment, specific to the patient's risk assessment. A variety of drugs, including antibiotics to treat ulcers and infections in the skin and body, as well as medication for high blood pressure may be taken by the patient.
Patients with scleroderma can present with low mood and/or depression because of the disabling affect that this has on their daily lives. Dental professionals must be aware of this condition so that they are confident to speak with the patient and signpost to further support services, if required.
Physiotherapists are sometimes involved to aid with exercises to improve movements in the face and body. Patients will need regular dental and hygienist appointments owing to the adverse effects of xerostomia and factors predisposing to gingival inflammation.9,10,11,12,13 Xerostomia is a common dental finding due to salivary gland fibrosis seen in systemic sclerosis. Sjögren's syndrome is seen in 60% of patients with systemic sclerosis10 and research shows that it is associated with, and not secondary to, the disease10. Xerostomia and xerophthalmia are both common findings evident as part of the autoimmune disorder. Both can be highly debilitating and uncomfortable. Xerostomia also increases the risk of tooth decay as well as disturbing speech, taste, mastication and carrying out dental treatment. Preventive advice and targeted fluoride therapy must be given.
Oral access is difficult due to microstomia and tightening of intra-oral tissues. Careful clinical examination of tissues must be carried out at every visit to ensure any potentially malignant conditions are caught early.11
The restricting nature of sclerodactyly can affect patient's ability to carry out effective oral hygiene care. A putty mould can be made in the clinic of the patients grasp, which can then be attached to their toothbrush to improve toothbrushing. Larger-sized toothbrushes and electric toothbrush options may also be more effective and provide easier access to posterior teeth (Figure 4).
Figure 4. Clinical photographs showing restricted maximal mouth opening. Tight banding of the oral musculature can be seen with skin appearing thin and stretched.
Discussion
Patients with systemic sclerosis can vary from having a mild, moderate or, in rare cases, a severe form of the disease. The condition affects connective tissue in the entire body with the limited cutaneous form affecting the distal extremities of the skin and joints, and diffuse cutaneous form also affecting upper arms, thighs and trunks. Both forms can affect the internal organs to varying degrees.
Most patients can be treated in the practice setting, ensuring an accurate medical history is taken regularly and communication with the patients' medical team is carried out prior to treatment to allow risk assessment. Regular hygiene visits are advised to care for the adverse periodontal effects seen.9,11,12,13
Patients need to be cared for holistically, from ensuring they are not kept waiting in a cold dental lounge, reducing stress for the patient by having open communication to discuss any anxieties, to gentle manipulation of oral tissues and careful examination and treatment. Complex treatment may require specialist referrals if access is more challenging to allow appropriate time and management. Difficulty in carrying out prosthetic dental work, including dentures and bridgework for this patient group, has described the importance of time and tailored specialist patient care. Sectional tray impression technique and advantages of bridgework over dentures have been discussed to aid in patient compliance and prosthetic success.15,16,17
Figure 3 shows how this condition can severely affect the movement of the hands and fingers, which greatly hinders all aspects of effective oral healthcare. A larger-size toothbrush or electric toothbrush is advised to aid with palmar grasp and toothbrushing. Regular dental appointments with an emphasis on prevention is important and high fluoride prescription toothpaste is advised to reduce the risk of dental caries secondary to xerostomia and any inability to carry out good oral hygiene.
Further guidance is needed regarding the dental management of patients on certain medications, such as monoclonal antibody therapy that targets the immune system.18 These medications can have different effects on the immune system and may require adjustment if dental surgery is required. Liaising with the medical team prior to invasive dental treatments is important to provide guidance on how patients on these medications are best treated.
Scleroderma can affect many different parts of the body and has significant implications for how dentistry is delivered. Understanding the disease and its oro-facial presentation will allow safe, effective clinical treatment and improve patients own oral health practices.