Friedlander AH, Marder SR, Sung EC, Child JS. Panic disorder: psychopathology, medical management and dental implications. J Am Dent Assoc. 2004; 135:771-778 https://doi.org/10.14219/jada.archive.2004.0306
Alonso J, Liu Z, Evans-Lacko S, Sadikova E Treatment gap for anxiety disorders is global: results of the World Mental Health Surveys in 21 countries. Depress Anxiety. 2018; 35:195-208 https://doi.org/10.1002/da.22711
Lack CW. Obsessive-compulsive disorder: evidence-based treatments and future directions for research. World J Psychiatry. 2012; 2:86-90 https://doi.org/10.5498/wjp.v2.i6.86
International Classification of Diseases 11th Revision. Mortality and Morbidity Statistics: Mental, Behavioural or Neurodevelopmental Disorders. 2022. https://icd.who.int/browse11/l-m/en (accessed October 2022)
Crerand CE, Phillips KA, Menard W, Fay C. Nonpsychiatric medical treatment of body dysmorphic disorder. Psychosomatics. 2005; 46:549-555 https://doi.org/10.1176/appi.psy.46.6.549
Aggarwal VR, Wu J, Fox F Implementation of biopsychosocial supported self-management for chronic primary oro-facial pain including temporomandibular disorders: a theory, person and evidence-based approach. J Oral Rehabil. 2021; 48:1118-1128 https://doi.org/10.1111/joor.13229
Kessler RC, Amminger GP, Aguilar-Gaxiola S Age of onset of mental disorders: a review of recent literature. Curr Opin Psychiatry. 2007; 20:359-364 https://doi.org/10.1097/YCO.0b013e32816ebc8c
Bolton JM, Gunnell D, Turecki G. Suicide risk assessment and intervention in people with mental illness. BMJ. 2015; 351 https://doi.org/10.1136/bmj.h4978
Why does patient mental health matter? Part 2: orofacial obsessions as a consequence of psychiatric conditions Emma Elliott Emily Sanger David Shiers Vishal R Aggarwal Dental Update 2024 49:10, 707-709.
Honorary Research Consultant, Psychosis Research Unit, Greater Manchester Mental Health NHS Trust, Manchester; Honorary Reader in Early Psychosis, Division of Psychology and Mental Health, University of Manchester; Honorary Senior Research Fellow, School of Medicine, Keele University, Staffordshire
This is the second article in a series looking at psychiatric presentations in dentistry. Recently, the oral health of people with severe mental illness (SMI) has gained significant media attention after the Office of the Chief Dental Officer for England published a statement on the importance of prioritizing oral health for people with SMI. Furthermore, a consensus statement has set out a 5-year plan to improve oral health in people with SMI. In keeping with these developments, this article explores the presentation of dental-specific obsessions and their relationship with psychiatric conditions, identifying how the primary care dental team can play a role in early recognition of psychiatric presentations. A fictionalized case-based discussion is used to explore clinical presentations of orofacial obsessions and their potential relationship to psychiatry.
CPD/Clinical Relevance: The role of the primary care dental team can be important for recognizing psychiatric conditions, such as obsessive compulsive disorder, body dysmorphic disorder and early psychosis.
Article
Recently, the oral health of people with severe mental illness (SMI) gained significant media attention after the Office of the Chief Dental Officer for England published a statement on the importance of prioritizing oral health for people with SMI.1 Two authors (VA and DS) have also been involved in a consensus statement2 that sets out a 5-year plan to improve oral health in people with SMI. In keeping with these developments, this article explores the presentation of dental-specific obsessions and their relationship with psychiatric conditions, identifying how the primary care dental team can play a role in early recognition of psychiatric presentations.
It is common within general dental practice to encounter patients who have presenting complaints that link to perceived defects in appearance, especially as aesthetic dentistry gains awareness. Such presenting complaints may not be linked to any underlying pathology; however, it is important to consider how a patient's psychological wellbeing may influence negative perceptions of their dental health or orofacial appearance. In this article, the fictionalized case of a young female patient presenting with an aesthetic dental complaint is explored and how this may relate to psychiatric disorders is considered.
Case scenario
A 20-year-old female patient attends your practice for a new patient examination. She reports in her medical history that she is fit and well, with no medications or allergies. You ask her if she has any current dental problems and she immediately brings up her front tooth, specifically how the ‘right one’ is grey and discoloured. Her primary concern is how it looks, but she is convinced there must be something wrong with it. She says she has been brushing her teeth with whitening toothpaste four times a day to try and counteract this discolouration. On examination the UR1 is clinically sound and is normal in colour, with no signs of disease and there is no history of trauma.
You explain this to the patient, but she insists that the tooth is discoloured and must be diseased, so you undertake radiographic examination in the form of a peri-apical radiograph to exclude dental pathology. The radiograph confirms absence of pathology. As you were reviewing the radiograph, the patient has brought up pictures on her phone that she says show the tooth changing over time. Visually, there have been no changes in the tooth, but you note she has been taking a picture almost every day for the past few weeks.
What are our initial thoughts?
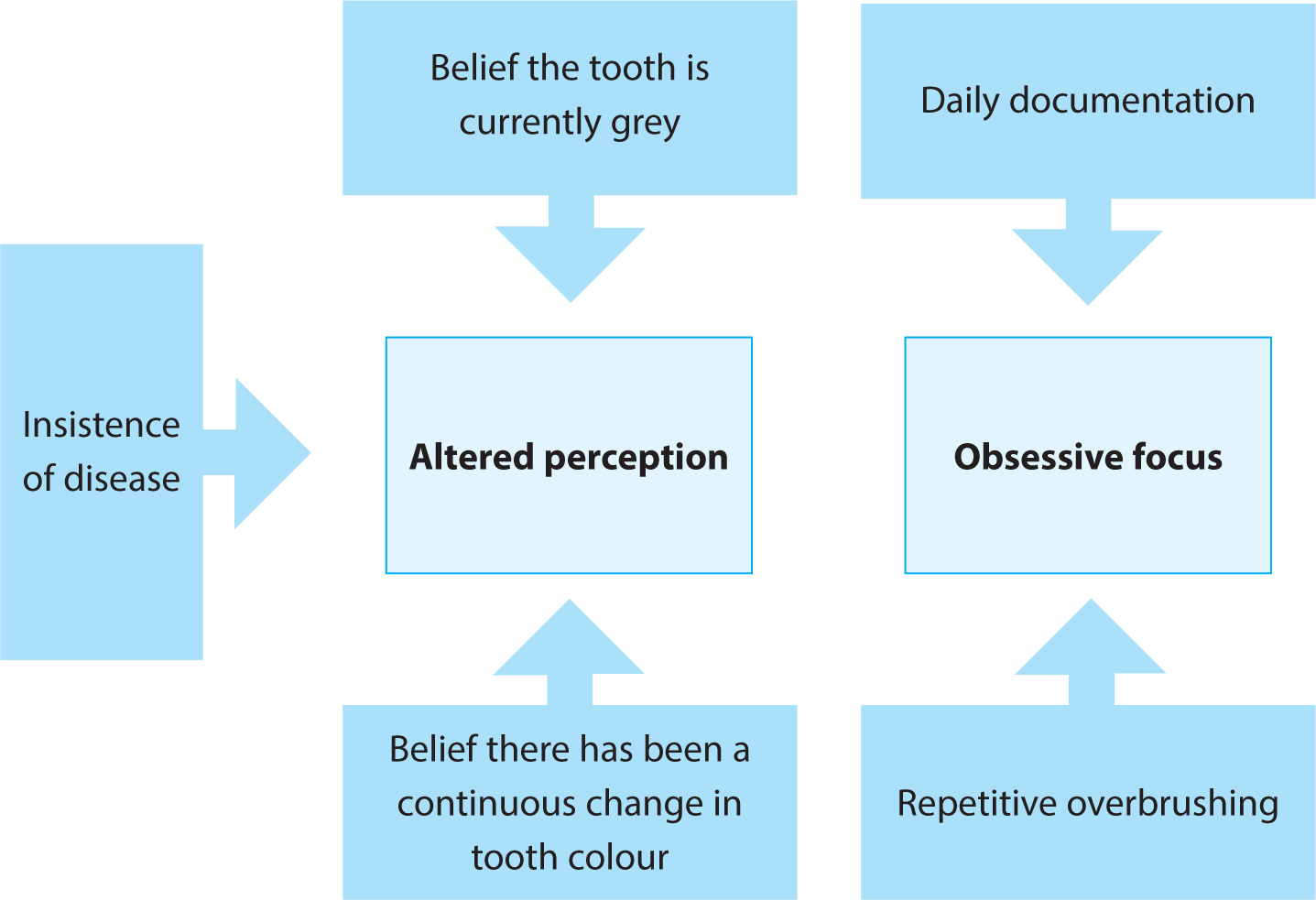
The scenario presents a patient with two potential sources of psychiatric concern, one of altered perception and one of obsessive focus (Figure 1). From a dental perspective, key complexities of the scenario include the patient's insistence on the presence of disease and the difficulty this poses in providing an explanation in the absence of pathology. Ultimately, there is real potential for undertaking unnecessary treatment.
Figure 1. The features of the scenario and how they result in a presentation of altered perception and obsessive focus.
The lack of significant medical history further complicates the presentation with regards to mental health because the dentist may be the only healthcare practitioner she has seen in a while.
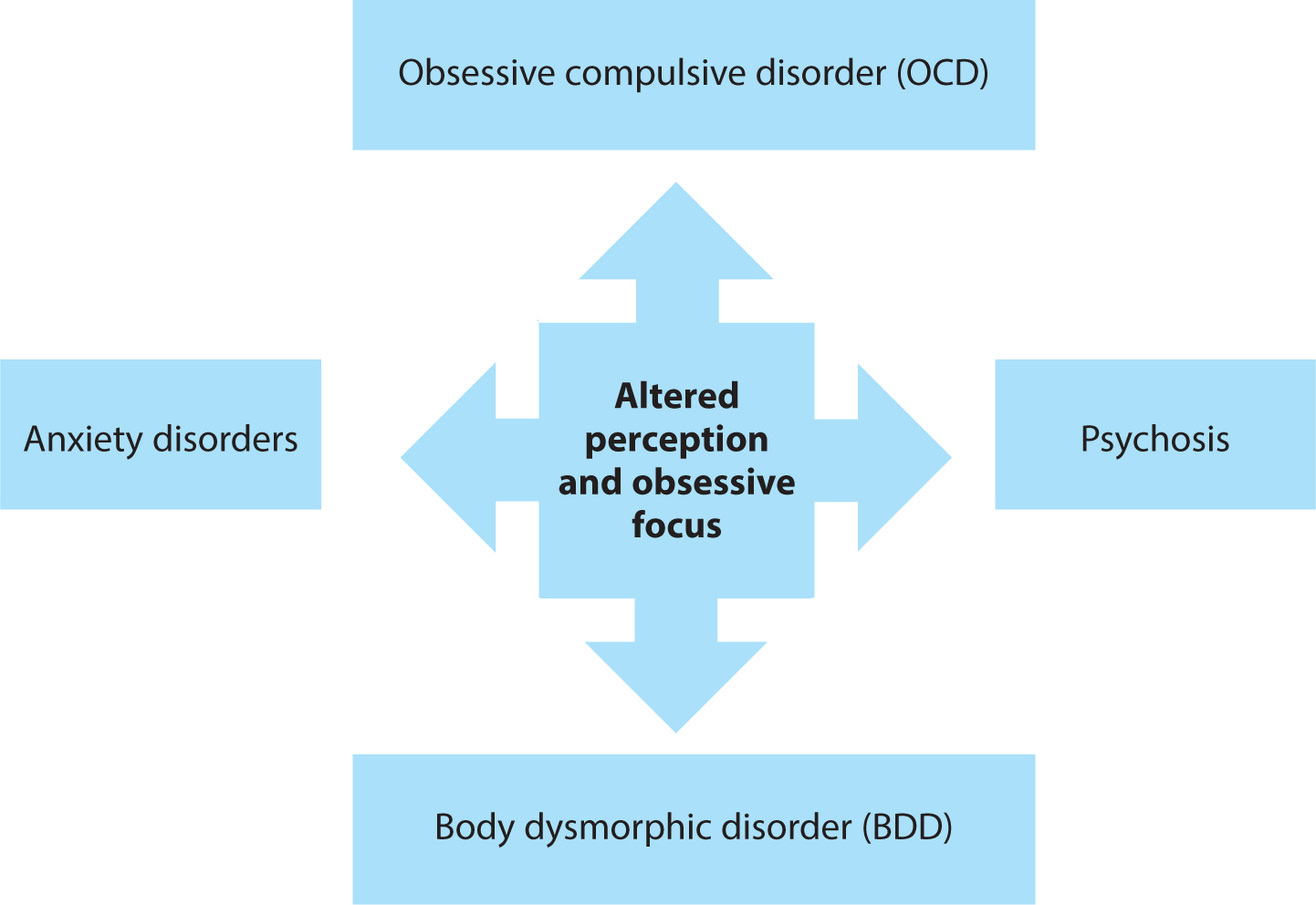
Her altered perception, obsessive focus, age and gender are suggestive of several psychiatric conditions,3,4,5,6,7,8,9,10,11,12,13 which are outlined in Figure 2.
Figure 2. The psychiatric conditions that may relate to the patient's obsessive focus and altered perception.3,4,5,6,7,8,9,10,11,12,13
Body dysmorphic disorder is part of the umbrella of somatization disorders.14 Somatoform disorders produce physical symptoms in response to psychological distress14 and, in this case, a psychiatric condition could be somatizing as a diseased tooth. While we touch upon somatoform disorders in this article, they will be covered more thoroughly later in the series.
Is the presenting complaint related to anxiety?
Anxiety disorders are the most prevalent class of psychiatric disorders that could relate to the patient's presenting complaint. Anxiety disorders often present in adolescence or early adulthood, and encompass a wide range of conditions, including panic disorder, social anxiety and generalized anxiety.1 While the patient is in the right demographic for an anxiety disorder, we can narrow down the presentation to social or generalized anxiety because her behaviour does not indicate panic disorder.3
Panic disorder presents as unpredictable and intense levels of anxiety. Patients affected by panic disorder are likely to develop acute, physical symptoms, such as chest pain, palpitations and shortness of breath. For the general dental practitioner, this may be confused with a cardiac medical emergency, and it is important to be aware of panic attacks and their presentation.4 The lack of such features in the scenario leads us to consider generalized anxiety disorder or social anxiety, focusing on general anxiety first, as the more common of the two.
Generalized anxiety disorder (GAD) affects 5.9% of the UK population and 6.8% of women.15 GAD is marked by an ‘uncontrollable, anxious worry about everyday events or problems,’3 and as part of this excessive generalized worry, we may see concerns about dental health. Anxious, uncontrollable worries can negatively impact functioning – in our scenario, the patient is spending a disproportionate amount of time on her perceived dental problem. This over-brushing and daily documentation may be restricting her daily life and could lead to tooth wear if not appropriately addressed.
It is worth exploring why she is anxious about the perceived discolouration of the front tooth, despite your reassurance of the tooth being healthy. The anxiety may be rooted in fear of ‘scrutiny or negative judgement by other people,’3 which would be more indicative of social anxiety disorder. However, this is less likely because she does not seem to have an avoidance of social interactions or situations, having attended the dental practice and communicated her concerns to you with no apparent difficulty.
A treatment gap exists for anxiety disorders, in which they are generally underdiagnosed and undertreated.5 Among those who have a perceived need for care, only one-third actually receive treatment for their anxiety disorder.5 When interacting with this patient, it is important to recognize that an unmanaged presentation of anxiety is highly likely. However, there is a lack of generalized anxiety in her presentation, and her concerns seem specifically localized to this one tooth, making OCD an alternative consideration.
Might OCD play a role in her presentation?
Extreme worry is an overlapping symptom of both anxiety disorders and obsessive compulsive disorder (OCD), and anxiety can often be comorbid with a presentation of OCD.6 However, in anxiety disorders, patients do not engage in ‘repetitive, ritualistic behaviours’;3 instead, this is a clinical feature of OCD. OCD is especially prevalent among young adults4,7 and the two most commonly reported compulsions are cleaning and checking.7 These two facts make it highly likely that the patient may be experiencing OCD, acting on compulsions, such as daily documentation and over-brushing. Furthermore, 60% of first symptoms of OCD are reported before the age of 25, followed by an average of 8 years before the individual seeks psychiatric treatment.7 At 20, the patient has a likelihood towards an unmanaged presentation of OCD; however, her lack of insight into her obsession complicates the presentation.
In cases of OCD, the individual recognizes that their obsessions are both irrational and self-generated.7 People who experience OCD are unable to suppress their obsessions, often presenting with an associated compulsion. In our case, the patient lacks insight into her own obsession and resultant compulsions, insisting there is an observable defect. We should therefore additionally explore her altered perception of her front tooth in the form of a somatization disorder, such as body dysmorphic disorder.
Could body dysmorphic disorder be driving her expressed need for treatment?
When contemplating altered perception and perceived defects in appearance, we must consider the presentation of Body Dysmorphic Disorder (BDD). BDD is categorized as part of the obsessive-compulsive spectrum of disorders; however, unlike in OCD, few individuals with BDD have good insight into their obsessive focus.8 These preoccupations are often driven by feelings of anxiety and individuals with BDD may focus on a perceived defect for 3–8 hours per day, compulsively checking, picking or camouflaging.9 BDD presents with specific criteria that must be met in order to make a diagnosis. Table 1 outlines these diagnostic criteria and how they relate to our clinical scenario.
Diagnostic criteria for BDD (ICD-11)
How does this relate to the clinical picture?
Preoccupation with an imagined defect in appearance. If a slight anomaly is present, the concern is markedly excessive and there is profound self-consciousness
The patient has an imagined defect, with a clinically healthy tooth that has no apparent discolouration
The preoccupation causes clinically significant distress or impairment in social, occupational, or other important areas of functioning. There can be attempts to camouflage or disguise the defect, avoidance of social situations or repeated excessive checking
The patient is experiencing significant distress. She is convinced of dental disease and is spending time documenting and attempting to counteract the perceived defect
The symptoms are not as a result of another medical condition or the effects of substances or medications
Based on our limited clinical information, we cannot comment on whether the patient fits this criterion
In cases of unfounded or excessive aesthetic dental complaints, it is reasonable for a practitioner to consider the potential for BDD. In one study of 250 individuals experiencing BDD, 76% sought cosmetic treatment in some form, with 66% receiving non-psychiatric medical treatment, for example dermatological or surgical intervention for their aesthetic complaint.11 Despite this, invasive treatment of the aesthetic complaint fails to improve symptoms in over 90% of patients experiencing BDD.11 Thus, any treatment attempted by practitioners is often unnecessary and unhelpful, instead it can be more useful to take a step back and consider some important questions (Table 2).
Probing question
Information gained
Are there any other psychiatric conditions in the medical history?
BDD can only be considered as a potential in the absence of a psychiatric condition that better accounts for the preoccupation. If you are considering any communication with other services it is best to have an awareness of perceived risk, such as self-harm or suicidal thoughts
Has the patient ever seen another clinician about the issue?
Often in cases of BDD, patients will visit multiple practitioners in the hope of receiving treatment. With this question, you may find that the patient has already received treatment, or that they have previously been turned away by another clinician
What does the patient expect from treatment and why have they sought help?
In this case, it is reasonable to explore the patient's treatment expectations as you can gain an insight into how grounded their goals are.12 Asking why they have sought help can further enlighten a practitioner to what extent the defect is affecting the patient's quality of life. Obsessions or rituals can occupy hours of a patient's day and can severely impact social functioning
Could this presentation be an early sign of psychosis?
Early symptoms of psychosis can be difficult to identify, but an emerging psychosis can present as a patient appearing ‘not quite right’. Broadly, this can present as a breakdown in social functioning, withdrawing from social relationships, education or work.13 More specifically there can be signs of early psychotic thinking that include suspicion, distrust, odd beliefs or perceptual changes.13
The patient could be experiencing a visual perceptual disturbance reinforced by delusional thinking and beliefs that are difficult to shake off. This could explain why there is apparent resistance to medical opinion in the scenario. She is also a young patient; 80% of new psychosis patients present between 16 and 30 years of age.14 Overall, psychosis carries a high risk to self, with schizophrenia having a lifetime suicide risk of 5.6%. However, the early stages of psychosis have a ‘1.6 times greater mortality risk compared to later stages of the illness’.15 Early identification and intervention can halve the risk of suicide and potentially prevent the onset of psychosis.13 Insight into the patient's mental state can be sought by asking the questions shown in Figure 3.13
Figure 3. Suggested questions to ask a patient who may be experiencing an emerging psychosis.13
What should I do now?
In this instance, it is best to defer any invasive dental treatment until you can better assess the situation. It would be reasonable to suggest to the patient that you can both monitor the tooth together going forwards, perhaps supported by taking clinical photographs today. The potential for BDD in this case makes the provision of invasive dental treatment risky and unwise; people with BDD often report high levels of dissatisfaction with treatment, with over 90% of procedures producing no change in BDD symptoms.11 While this condition remains a possibility, it is wise to restrict yourself to monitoring and reassurance.
The risk of suicide is generally higher in the early stages of all mental health disorders, and this is especially true of psychosis. There is no widely accepted standard for assessing suicide risk, but there is evidence demonstrating that asking about a patient's suicide risk does not increase their suicidal ideation.18 When considering communicating to another healthcare practitioner about a patient's mental wellbeing, an awareness of their suicide risk can be valuable information. Questions should include whether there has been any previous suicidal behaviour, if the patient has any current thoughts or plans, or if they are experiencing any feelings of hopelessness or significant stressors.18
This appointment would be best spent exploring what we have discussed above and how the patient feels about her need for treatment. Additionally, an onward referral to a mental health professional is indicated. It would be sensible to ask the patient for consent to communicate with her general medical practitioner and explore potential referral to psychiatric services via this pathway. This can be a difficult conversation to navigate and should be approached sensitively.