van Noort R The future of dental devices is digital. Dent Mater. 2012; 28:3-12
Hull C Apparatus for Production of Three-Dimensional Object by Stereolithography. 1986;
Wohlers Associates. What is 3D printing? Wohler's Report 2013.
NASA to launch 3D printer into space to help supply astronauts. 2013.
Schubert C, van Langeveld MC, Donoso LA Innovations in 3D printing: a 3D overview from optics to organs. Br J Ophthalmol. 2014; 98:159-161
Gao B, Wu J, Zhao X, Tan H Fabricating titanium denture base plate by laser rapid forming. Rapid Prototyp J. 2009; 15:133-136
Banks J Adding value in additive manufacturing: researchers in the United Kingdom and Europe look to 3D printing for customization. IEEE Pulse. 2013; 4:22-26
Ventola LC Medical applications for 3D printing: current and projected uses. P T. 2014; 39:(10)704-711
Miller JS, Stevens KR, Yang MT Rapid casting of patterned vascular networks for perfusable engineered three-dimensional tissues. Nat Mater. 2012; 11:768-774
Jeong JE, Chan V, Cha C “Living” microvascular stamp for patterning of functional neovessels; orchestrated control of matrix property and geometry. Adv Mater. 2012; 24:58-63
Leukers B, Gulkan H, Irsen SH Hydroxyapatite scaffold for bone tissue engineering made by 3D printing. J Mater Sci Makter Med. 2005; 16:1121-1124
Mannoor MS, Jiang A, James T 3D Printed bionic ears. Nano Lett. 2013; 13:2634-2639
Haumont T, Rahman T, Sample W Wilmington robotic exoskeleton: a novel device to maintain arm improvement in muscular disease. J Pediatr Orthop. 2011; 31:e44-49
Zopf DA, Hollister SJ, Nelson ME Bioresorbable airway splint created with a three-dimensional printer. N Engl J Med. 2013; 368:2043-2045
Gross BC, Erkal JL, Lockwood SY, Chen C, Spence DM Evaluation of 3D printing and its potential impact on biotechnology and the chemical sciences. Anal Chem. 2014; 86:3240-3253
Mueller AA, Paysan P, Schumacher R Missing facial parts computed by a morphable model and transferred directly to a polyamide laser-sintered prosthesis: an innovation study. Br J Oral Maxillofac Surg. 2011; 49:67-71
Traini T, Mangano C, Sammons RL Direct laser metal sintering as a new approach to fabrication of an isoelastic functionally graded material for manufacture of porous titanium dental implants. Dent Mater. 2008; 24:1525-1533
Akova T, Ucar Y, Tukay A, Balkaya MC, Brantley WA Comparison of the bond strength of laser-sintered and cast base metal dental alloys to porcelain. Dent Mater. 2008; 24:1400-1404
Fukuda A, Takemoto M, Saito T Osteoinduction of porous Ti implants with a channel structure fabricated by selective laser melting. Acta Biomater. 2011; 7:2327-2336
Tara MA, Eschbach S, Bohlsen F, Kern M Clinical outcome of metal-ceramic crowns fabricated with laser-sintering technology. Int J Prosthodont. 2011; 24:46-48
Williams RJ, Bibb R, Eggbeer D, Collis J Use of CAD/CAM technology to fabricate a removable partial denture framework. J Prosthet Dent. 2006; 96:96-99
Ucar Y, Akova T, Akyil M, Brantley W Internal fit evaluation of crowns prepared using a new dental crown fabrication technique: laser-sintered Co-Cr crowns. J Prosthet Dent. 2009; 102:253-259
Kanazawa M, Iwaki M, Minakuchi S, Nomura N Fabrication of titanium alloy frameworks for complete dentures by selective laser melting. J Prosthet Dent. 2014; 112:1441-1447
Chen J, Zhang Z, Chen X Design and manufacture of customized dental implants by using reverse engineering and selective laser melting technology. J Prosthet Dent. 2014; 112:1088-1095
Serra-Prat J, Cano-Batalla J, CabratosaTermes J, Figueras-Àlvarez O Adhesion of dental porcelain to cast, milled, and laser-sintered cobalt-chromium alloys: shear bond strength and sensitivity to thermocycling. J Prosthet Dent. 2014; 112:249-256
Wu L, Zhu H, Gai X, Wang Y Evaluation of the mechanical properties and porcelain bond strength of cobalt-chromium dental alloy fabricated by selective laser melting. J Prosthet Dent. 2014; 111:51-55
: The NHS Information Centre for Health and Social Care; 2011
Santos EC, Shiomi M, Osakada K, Laoui T Rapid manufacturing of metal components by laser forming. Int J Mach Tools Manuf. 2006; 46:(12-13)1459-1468
Shellabear M, Nyrhilä O DMLS – development history and state of the art.Erlangen, Germany: Bamberg-Meisenbach; 2004
Gebhardt A, Schmidt FM, Hötter JS, Sokalla W, Sokalla P Additive manufacturing by selective laser melting the realizer desktop machine and its application for the dental industry. Phys Proc. 2010; 5:543-549
Deckard C, Beaman J Process and control issues in selective laser sintering. ASME Prod Eng Div (Publication) PED. 1988; 33:191-197
Wang XC, Laoui T, Bonse J Direct selective laser sintering of hard metal powders: experimental study and simulation. Int J Adv Manuf Technol. 2002; 5:351-357
Venkatesh K, Nandini V Direct metal laser sintering: a digitised metal casting technology. J Indian Prosthodont Soc. 2013; 13:389-392
Hems E, Knott NJ 3D Printing in Prosthodontics. Faculty Dent J. 2014; 5:152-157
Quante K, Ludwig K, Kern M Marginal and internal fit of metal-ceramic crowns fabricated with a new laser melting technology. Dent Mater. 2008; 24:1311-1315
Gaytan SM, Murr LE, Martinez E Comparison of microstructures and mechanical properties for solid and mesh cobalt-base alloy prototypes fabricated by electron beam melting. Metall Mater Trans A. 2010; 41:3216-3227
Ayyıldız S, Soylu EH, Ide S, Kılıç S, Sipahi C, Pişkin B, Gökçe HS Annealing of Co-Cr dental alloy: effects on nanostructure and Rockwell hardness. J Adv Prosthodont. 2013; 5:471-478
Chen CL, Tatlock GJ, Jones AR Effect of annealing temperatures on the secondary re-crystallization of extruded PM2000 steel bar. J Microsc. 2009; 233:474-481
Guo WH, Brantley WA, Li D Annealing study of palladium-silver dental alloys: Vickers hardness measurements and SEM microstructural observations. J Mater Sci Mater Med. 2007; 18:111-118
Figliuzzi M, Mangano F, Mangano C A novel root analogue dental implant using CT scan and CAD/CAM: selective laser melting technology. Int J Oral Maxillofac Surg. 2012; 41:858-862
Örtorp A, Jönsson D, Mouhsen A, von Steyern PV The fit of cobalt-chromium three-unit fixed dental prostheses fabricated with four different techniques: a comparative in vitro study. Dent Mater. 2011; 27:356-363
Kim KB, Kim JH, Kim WC, Kim JH Three-dimensional evaluation of gaps associated with fixed dental prostheses fabricated with new technologies. J Prosthet Dent. 2014; 112:1432-1436
Killiçarsian MA, Özkan P, Uludag B, Mumcu E Comparison of internal fit between implant abutments and cast metal crowns vs laser-sintered crowns. J Contemp Dent Pract. 2014; 15:428-432
Xin XZ, Chen J, Xiang N, Wei B Surface properties and corrosion behavior of Co-Cr alloy fabricated with selective laser melting technique. Cell Biochem Biophys. 2013; 67:983-990
Al Jabbari YS Physico-mechanical properties and prosthodontic applications of Co-Cr dental alloys: a review of the literature. J Adv Prosthodont. 2014; 6:138-145
Choi Y, Koak J, Heo S Comparison of the mechanical properties and microstructures of fractured surface for Co-Cr alloy fabricated by conventional cast, 3-D printing laser-sintered and CAD/CAM milled techniques. J Korean Acad Prosthodont. 2014; 52:67-73
Geneva, Switzerland
Puskar T, Jevremovic D, Williams RJ A comparative analysis of the corrosive effect of artificial saliva of variable pH on DMLS and cast Co-Cr-Mo dental alloy. Materials. 2014; 7:6486-6501
Ting-Shu S, Jian S Intraoral digital impression technique: a review. J Prosthodont. 2015; 24:313-321
Mehl A, Gloger W, Kunzelmann KH, Hickel R A new optical 3-D device for the detection of wear. J Dent Res. 1997; 76:1799-1807
Bhaskaran E, Azhagarasan NS, Miglani S Comparative evaluation of marginal and internal gap of Co-Cr copings fabricated from conventional wax pattern, 3D printed resin pattern and DMLS tech: an in vitro study. J Indian Prosthodont Soc. 2013; 13:189-195
The use of 3D metal printing (direct metal laser sintering) in removable prosthodontics Dominic P Laverty Matthew BM Thomas Paul Clark Liam D Addy Dental Update 2024 43:9, 707-709.
Authors
Dominic PLaverty
ACF/StR in Restorative Dentistry, Birmingham Dental Hospital
The use of 3D printing is expanding and it is envisaged that it will have an increasing presence within dentistry. Having an appreciation and understanding of such technology is therefore paramount. It is currently used to produce a variety of dental objects/ prostheses. This paper briefly looks at 3D printing in dentistry and specifically describes the use of the direct metal laser sintering 3D printing technique in the production of cobalt chromium removable prosthesis frameworks.
CPD/Clinical Relevance: Understanding the different technologies that can and are being used within the dental field is important, particularly as it is a rapidly changing field. Having an understanding of such technologies will allow practitioners to utilize such technologies appropriately in the management of their patients.
Article
Three-Dimensional (3D) printing is a process of making a 3D object from a digital file. The 3D object is created using an additive process whereby successive layers of material are placed until the object is created. These layers are thin horizontal 2D cross-sections of the eventual 3D object.1
It was Charles Hull in the early 1980s who invented 3D printing. He described the process of stereolithography or the ‘printing’ of successive layers of material on top of each other to create a 3D object.2
The use of 3D printing is expanding, with the entire 3D printing industry currently worth around $700 million, and is expected to grow to an estimated $8.9 billion industry in the next 10 years.3 Even NASA have used 3D printing to produce a fuel injector and plan to have a 3D printer on board their next space flight.4
This expansion in 3D printing is also being experienced within the medical field.5 The current 3D printing industry is worth $11 million for medical applications but is projected to have exponential growth over the next 10 years to $1.9 billion.6
One of the advantages that 3D printing offers in its medical application is the ability to allow customization and personalization of medical products and equipment, at relatively low costs (as the cost of the first item is the same as the last)5 and produced relatively quickly.7 Hence, 3D printing is ideal for making one of a kind items at cost-effective prices.5
3D printing has been applied in medicine and dentistry since the early 2000s with dentistry quick to embrace the use of this technology, particularly with regards to dental implant reconstructions.8
A number of published articles have described the use of 3D printing in medicine to produce cell cultures, blood vessels and vascular networks,9 bandages,10 bones,11 ears,12 exoskeletons,13 windpipes14 and corneas.15 The use of 3D printing is also being investigated in repairing or replacing defective organs, such as kidneys, the heart and skin.5
In dentistry, 3D printing can produce metallic, polymer16 and ceramic-based objects.1 It has been used to produce a variety of dental objects including stereolithographic models, implant fixtures and components, removable prosthesis frameworks, fixed prosthesis and maxillofacial structures (hard and soft tissue).17,18,19,20,21,22,23,24,25,26
Denture frameworks have traditionally been produced using the lost wax technique and metal casting; however, 3D printing methods are now available. These offer quicker and more cost-efficient production with reduced recasting. Removable partial dentures are still a well-recognized treatment, and around 19% of adults in the UK are wearing some form of removable prosthesis, as shown in the UK Adult Dental Health survey in 2009.27
This article aims to demonstrate the use of 3D printing in the production of removable prosthesis metal cobalt chromium (CoCr) frameworks.
Overview of 3D printing
3D printing is an additive process whereby successive layers of material are placed until the 3D object is created.1
This is markedly different from subtractive manufacturing, such as CAM (computer aided manufacture) Milling, where a block of material is cut away until the final object is created.
3D printing is a digital manufacturing process based on digital data with the 3D object being produced using computer-aided design (CAD) and manufacture (CAM).
This digital data/CAD file of the 3D object is divided into thin 2D sections using software programs. This sectioned data is sent to the printer layer-by-layer using CAM so that each layer is accurately formed and successively built on to produce the 3D object.
This CAD file data can be created in one of two ways; the first by optically scanning a 3D object via a process called reverse engineering24 or by designing the 3D object using CAD software.18
The benefits and challenges of 3D printing in dentistry is shown in Table 1.
Benefits
Challenges
Cost-saving materials (in comparison to traditional subtractive milling process of metal or ceramic or the conventional lost wax casting technique)31,34
Need appropriate training in the use of machinery and the software programs
Unlimited design and manufacturing capability34 (unlike milling machines which are limited by their milling axis) allowing customization, flexibility and geometric freedom24
If using conventional techniques in impression taking and casting of impressions this could be a source of error
If the CAD data is saved, the prosthesis can be re-made exactly or the design modified where required
If using digital scanners and software to transform the scanning data into a 3D model this to could be a source of error
High reproducibility of design (CAD) into the actual prosthesis, with reduced inclusions, defects or distortions (commonly occurring in manual casting processes)35
Faults include - defects: rough surface, pores, cracks, and distortion - but often can be rectified with finishing and polishing procedures24 and can be reduced by using small layer thickness and a small laser beam diameter36
Able to produce highly detailed complex surfaces34
A range of 3D printing technologies (additive process) are being used in dental industry, which include; stereolithography, fused deposition modelling, selective electron beam melting, laser powder forming methods and inkjet printing.1
This article will discuss the use of laser powder forming methods.
Laser powder forming methods
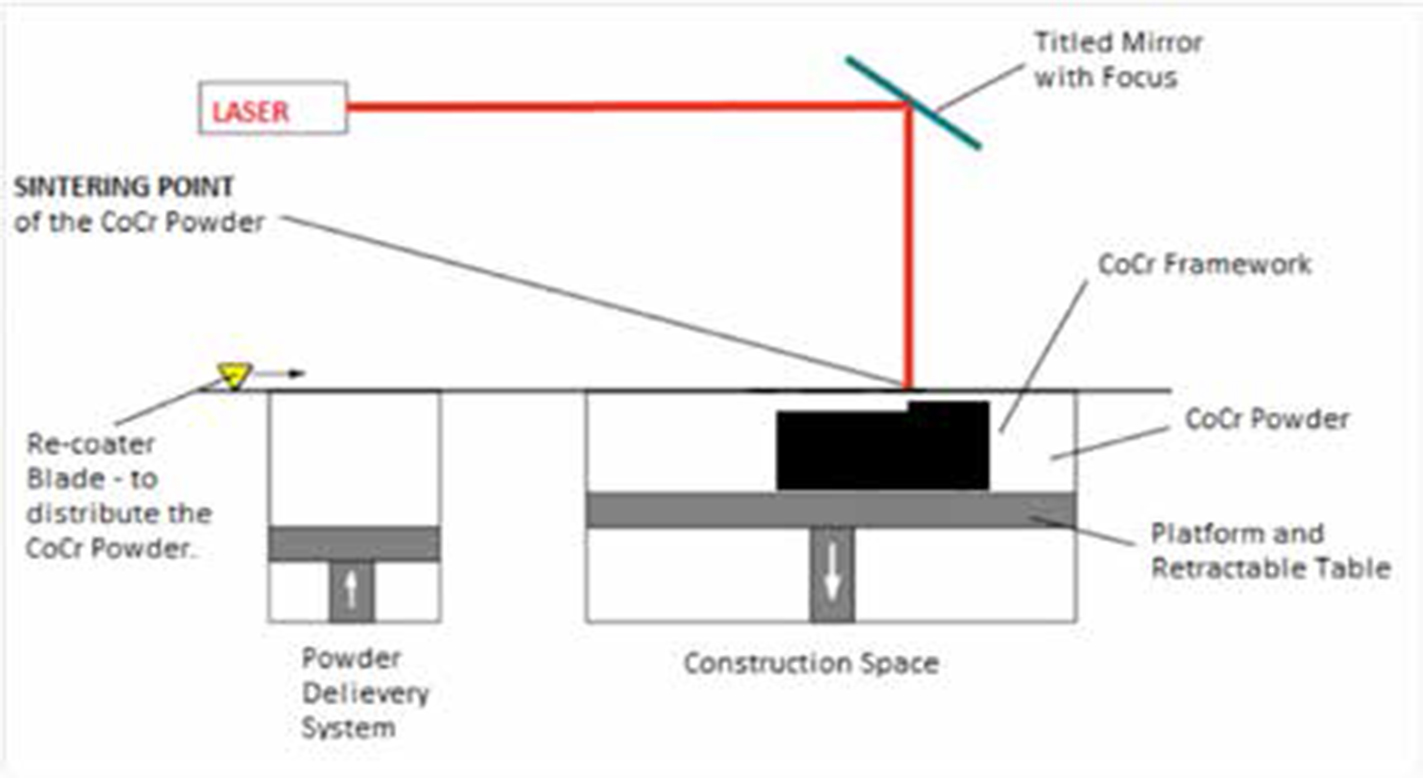
Laser powder forming methods are carried out by directing a laser via mirrors at a layer of fine powder substrate. The laser causes the powder either to melt, via a process called selective laser melting (SLM), or sinter via a process called selective laser sintering (SLS).28,29 The powder particles fuse together,28,29 and layer-by-layer build up by distributing an even layer of powder to produce the 3D object.1
SLM is very similar to SLS in terms of equipment but uses a much higher energy density. This enables full melting of the powders, whereas SLS sinters the powders.28
When using metal powders the process can either be known as SLM, if melting the powder, or DMLS (direct metal laser sintering) when sintering.1
To control this complex set of parameters, the process runs under shielding gas; fine grained powders are applied and sophisticated scan programs are used to govern the exposure by the laser beam. To achieve fine detail and reduce faults, a small layer thickness and a small laser beam diameter are necessary.30
A range of metal powders can be used including steel, titanium, titanium alloys, and Co/Cr alloy.1 Optimization has to be carried out for each material and the geometry of the part being produced and its supporting structure need to be considered. The resulting data is termed the material dataset,30 which is often produced by the manufacturers.
DMLS and dental use
The laser sintering process was first described by Deckard and Beaman, who created the DTM (desk top manufacturing) machine at the University of Texas.28,31 The process is referred to as 3D printing as it builds up an object in a series of successively thin layers.17
The physical process involved with the laser sintering can be full melting, partial melting, or liquid-phase sintering.32
This DMLS process is carried out by forming a thin layer of metal powder (ranging from 20 μm to 100 μm) and sintered by a laser (high powered ytterbium fibre laser) to form a 2D cross-section. This is then built up layer-by-layer by distributing an even layer of metallic powder to produce the 3D object.17 This process is carried out within a controlled inert atmosphere35 (Figure 1).
Figure 1. Schematic diagram of the DMLS process.
The 3D object being created has to be adequately supported during the DMLS process and thus have supporting structures designed into the 3D object. These are produced during 3D printing. The supporting structure ensures that the object is fixed in position to the underlying baseplate and ensures geometric accuracy, which is a vital part of the DMLS process. These supporting structures will then need removing after the production process.
The DMLS process is performed by one of two methods, powder deposition or the powder bed method:33
In the powder deposition method, the metal powder is sintered in a hopper then deposited in a thin layer onto the build platform;
In the powder bed method, a re-coater arm distributes a thin layer of powder onto the powder bed and is then sintered.
In both methods, layers are built on top of one another with the build platform being lowered each time to allow the application of the next layer of powder (Figure 2).
Figure 2. The DMLS process. (By kind permission of 3D Systems Leuven.)
Once complete, the excess powder is removed and the metal framework is carefully separated from the underlying baseplate. They then undergo a heat treatment process called annealing which advances the material to its equilibrium state.37,38 This involves heating the framework above the critical temperate and then cooling.38,39,40 This annealing process produces a more homogeneous metallic structure,38,41 and affects the microstructure and hardness of the alloy.39,40
The framework is then finished which includes removal of the supporting structures, sand blasting, polishing and ultrasonic cleaning.34,35
The printing time varies and is dependent on the 3D printer used, the number of jobs and the height of the jobs.
DMLS can be used to create crowns and bridges,18,20,22 crown copings for metal ceramic crowns,18,25,26 bridge frameworks, denture frameworks,21,23 implant abutments and implant fixtures.17,19,24 (Figures 3 and 4).
Figure 3. Variety of DMLS dental products produced by 3D Systems Leuven. (By kind permission from 3D Systems Leuven).Figure 4. Completed CoCr Framework using DMLS produced by Dentwise. (By kind permission from 3D Systems Leuven.)
There are a number of papers that have demonstrated the use of laser sintering in the production of denture frameworks.6,21,23
In comparing the use of DMLS to conventional lost wax technique and CAD/CAM milling in their use in producing metal dental prosthesis, it has been demonstrated that the marginal fit of prosthesis produced by DMLS is equal to, if not better than, these other methods.36,42,43,44 It has also been shown that restorations fabricated using this method produced good surface properties, such as proper hardness, homogeneous microstructure, and also showed sufficient corrosion resistance, and is appropriate for dental use.45
Production of the prosthesis using 3D printing/DMLS
There are a number of companies that offer 3D printing in dentistry for removable partial dentures (RPDs) metal frameworks. Renishaw plc, based in Gloucestershire, UK, offer a variety of 3D printed products for the dental market, and are close to commercially offering 3D printed CoCr Framework. 3D Systems Leuven, On Demand Parts Manufacturing site for healthcare, formerly known as DentWise, also offer a variety of 3D printed products for the dental market. They offer either CoCr or Titanium (Ti) RPD metal frameworks. They require an stl file (stereolithography file) with a designed RPD metal framework to be sent electronically, which is used to print the framework. The RPD frameworks are then trimmed and either delivered as a sandblasted or mirrored finished framework.
Individual 3D printed frameworks have the same cost range as conventional cast frameworks. However, it is envisaged that the cost of 3D production will reduce as this technology becomes more readily available and there is increased uptake and usage by practitioners.
The framework parameters and design software need to be discussed with the manufacturer to ensure compatibility.
There is a variety of DMLS 3D printers available on the market that are capable of producing an RPD metal framework which include; the AM250 laser melting additive manufacturing machine (Renishaw plc) and the EOS INT M 270 (Electro-optical systems GmBH), 3D Systems Leuven use their own 3D printer.
Cobalt chromium composition
Table 2 shows different dental CoCr alloys used for a variety of manufacturing techniques which include; conventional casting, CAD/CAM milling (S&S Schefner, Starbond CoS) and DMLS techniques (EOS, Cobalt Chrome RPD and Renishaw, Co-Cr-DG1). The alloys all have similar composition, despite having different manufacturing processes and all alloys are compliant with the standards of the International Organization for Standardization (ISO), as stated by the manufacturer.49
Element
Bego-Wironium Plus
Jelenco-Supra chrome
Dentsply prosthetics-Vitallium
Bredent-Brealloy F400
EOS - Cobalt Chrome RPD
S&S Schefner-Starbond CoS
Renishaw-Co-Cr-DG1
Co
62.5
63.6
63.4
64.7
63.8
59
63.9
Cr
29.5
28.5
29.0
29.0
24.7
25
24.7
Mo
5.0
6.0
5.2
5.0
5.1
3.5
5
Si
<1.0
<1.0
<1.0
0.5
1.0
1
<1.0
Fe
<1.0
0.5
<0.5
Mn
<1.0
<1.0
<1.0
0.4
0.1
<0.1
W
5.4
9.5
5.4
The CoCr dental alloys used for DMLS, however, have little scientific evidence reporting on their characteristics.50 The evidence currently available would suggest that the manufacturing technique, whether that be conventional casting, laser sintering or milling using CoCr dental alloys, has adequate mechanical properties satisfying the ISO standards of dental alloys.47
Digital impressions
Intra-oral digital impression scanners can be used to digitalize the process fully. The main intra-oral digital impression systems currently available on the market include CEREC, Lava COS system, iTero, E4D and TRIOS. All these systems vary in their key features, such as their working principle, light source, the need for powder coating, the clinical operative process, and the output file format.51
The digital scanner uses a ‘triangulation’ process to collect the 3D structures being scanned. To create this, a source of light and the receptor unit are in a specific angle to one another; this angulation allows the computer to produce a three-dimensional data set from the image on the receptor unit.52
In general, there are two types of intra-oral scanners on the market. The first uses blue LED (light-emitting diode); these systems depend upon a reflective surface and require a contrasting medium or powder to be placed on the structures being scanned. The other systems use laser technology to scan and measure distances from the tooth surface to acquire the image; they do not require powder.
It is advised to check the compatibility of the intra-oral scanner and RPD design software to ensure compatibly.
CAD software
There is a variety of RPD design software packages which include, 3Shape, Dental Wings, Exocad and Freeform plus™. These software packages vary in complexity. The simpler software packages can be used on a standard computer without the need for any additional equipment. However, more complex software packages may require the use of specialist equipment such as the use of a haptic arm which often requires further training and experience. These software packages create an stl file which is then used to produce the framework. The majority of 3D printers are capable of producing a framework from an stl file, but it's best to check with the manufacturer to ensure compatibility of the software and the printer.
Clinical and manufacturing technique
The following is an example of a design and manufacturing technique that has been utilized at University Dental Hospital in Cardiff.
Impression taking and conventional casting of impressions
Conventional master impressions are taken in an appropriately prescribed special tray with addition cure silicone-based material. This is then conventionally cast up (using Crystacal® R Plaster) creating the master model.
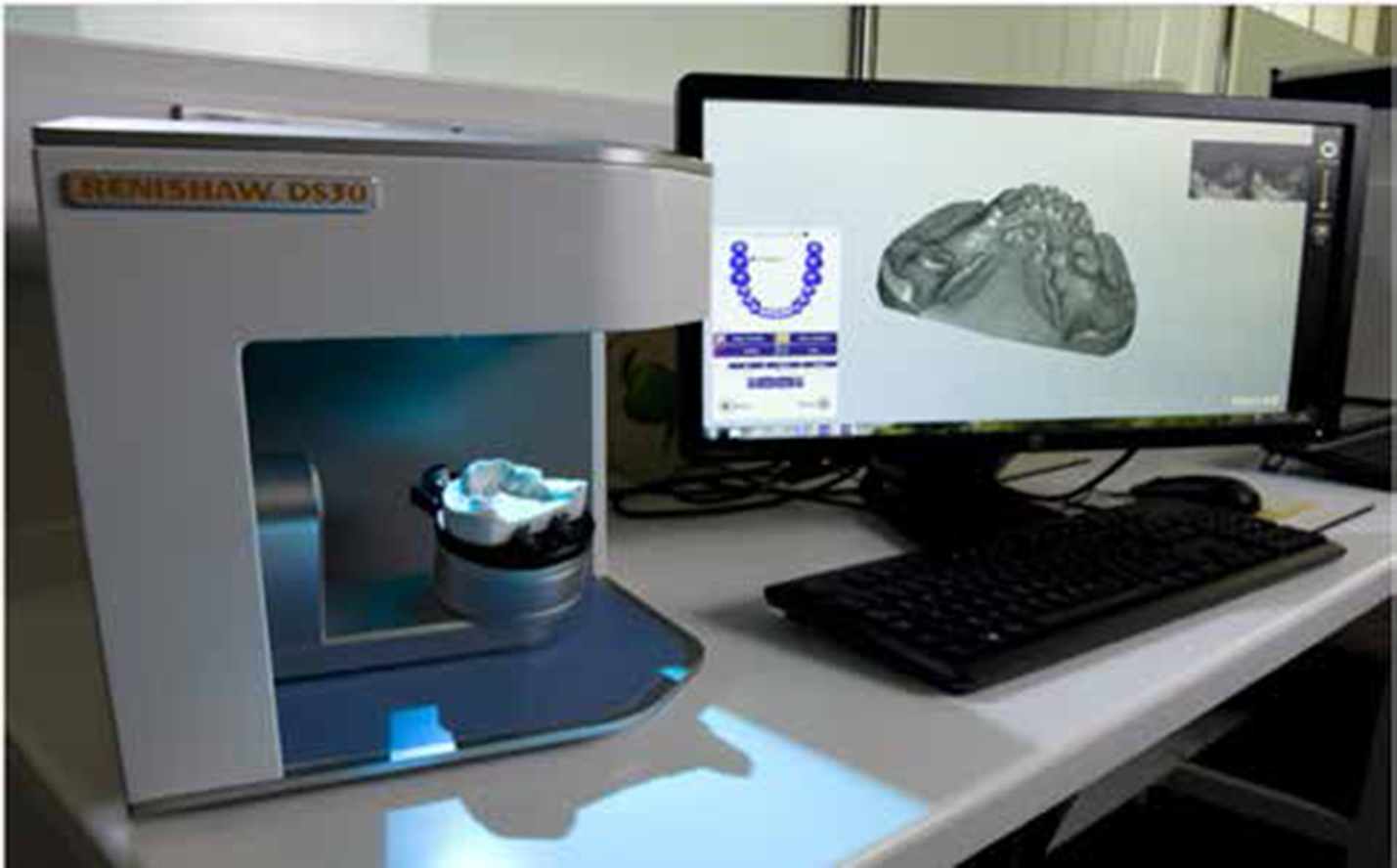
Digital scanning of models
The master model is then scanned using the DS30 Optical Scanner (Renishaw plc). The light optical scanner scans the model, registration and triangulation algorithms are then used to reconstruct the scanned data into an stl file which is a virtual model consisting of a mesh of triangles.53
An stl file format is used to interpret the data in a CAD file, allowing these instructions to be communicated electronically to the 3D printer.15 The data is then imported directly into the Freeform plusTM software (Geomagic®) (Figure 5).
Figure 5. DS30 Optical Scanner and Freeform plusTM software.
Denture design
The TouchTM X (Geomagic®) Haptic arm and Freeform plusTM software (Geomagic®) are used by the operator to design the prosthesis.54
The software can be used to survey the models, block out undercuts, identify insertion paths and guide planes and to design the prosthesis, offering the same capabilities as for a traditional prosthesis.54
The haptic arm is used to design the prosthesis and can accurately measure the 3D spatial position and the orientation of the handheld stylus. The device uses motors to create forces that push back on the user's hand to simulate touch and interaction with virtual objects54 (Figure 6).
Figure 6. Use of The TouchTM X (Geomagic®) Haptic arm and Freeform plusTM software.
Once the design is complete, the stl file data is then ‘sliced’ into sections by MagicsAutoFab (Materialise NV) software. The stl file is then sent directly to the manufacturing machine to construct the CoCr framework.35
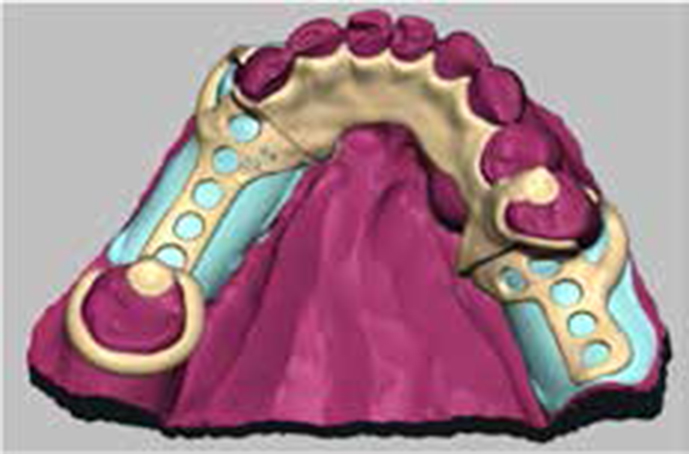
With a digital design it can be electronically sent to the practitioner and/or patient for approval prior to production; the data can also be saved and re-used/modified at a later date if required as well (Figure 7).
Figure 7. Denture design using Freeform plus™ software.
Manufacture
The CoCr framework is produced using the AM250 laser melting additive manufacturing machine (Renishaw plc). It uses a high-powered ytterbium fibre laser to fuse the fine metallic powders together, in a vacuum environment.35
The process is carried out by forming a thin layer of CoCr metal powder, 40 microns thick and sintered using the ytterbium fibre laser with the denture framework being built up layer-by-layer. This process is carried out within a controlled inert atmosphere35 (Figure 8).
Figure 8. CoCr Framework once 3D printing complete.
The metal supporting structures are removed from the metal framework. These supporting structures ensure that the framework is fixed in position to the underlying baseplate and ensure geometric accuracy, which is a vital part of the DMLS process. This is then removed after production, which is similar to the removal of the sprues used in conventional casting techniques of metal frameworks.
Once the framework is complete it can be trimmed, smoothed and polished in the conventional way.
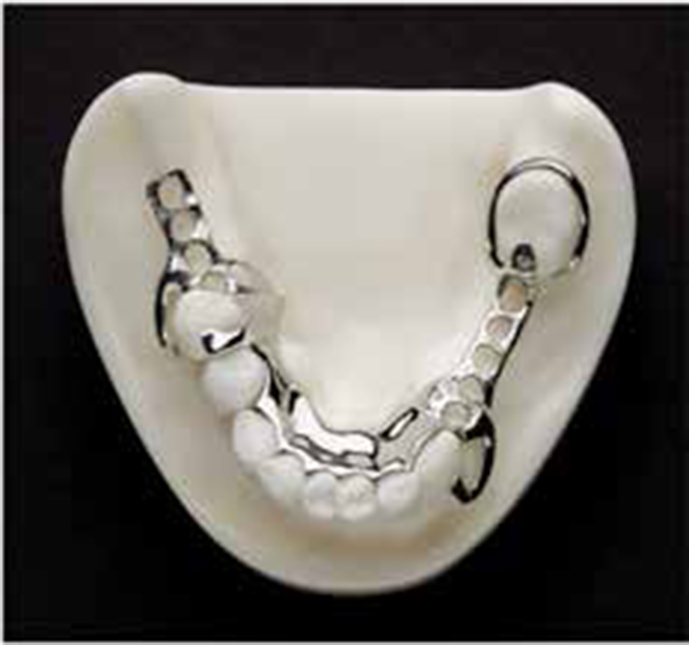
The rest of the laboratory process in the production of the prosthesis is via conventional methods (Figure 9).
Figure 9. CoCr Framework after polishing and trimming.
Conclusion
The use of 3D printing is expanding and it is envisaged that it will have an increasing presence within dentistry. Dental practitioners therefore need to be aware of what this technology can offer them and their patients and how this technology is developing.
The DMLS method has been shown to be successful in the production of removable prosthesis metal frameworks and has a number of advantages over conventional methods of production. It is a relatively new technique for producing metal RPD frameworks and is being introduced in clinical practice; however, research on its clinical utility compared to traditional methods is limited, and the process involves expensive equipment and processes to which dental practitioners may not be accustomed. It is recommended that long-term clinical trials be carried out to provide evidence to support this technique further.