Wright JT, Torain M, Long K Amelogenesis imperfecta: genotype-phenotype studies in 71 families. Cells Tissues Organs. 2011; 194:279-283
Uchida T, Tanabe T, Fukae M, Shimizu M Immunocytochemical and immunochemical detection of a 32 kDa nonamelogenin and related proteins in porcine tooth germs. Arch Histol Cytol. 1991; 54:527-538
Witkop CJ Amelogenesis imperfecta, dentinogenesis imperfecta and dentin dysplasia revisited: problems in classification. J Oral Pathol. 1988; 17:(9–10)547-553
Bäckman B, Holmgren G Amelogenesis imperfecta: a genetic study. Hum Hered. 1988; 38:189-206
Aren G, Ozdemir D, Firatli S, Uygur C, Sepet E, Firatli E Evaluation of oral and systemic manifestations in an amelogenesis imperfecta population. J Dent Res. 2003; 31:585-591
Seow W Dental development in amelogenesis imperfecta: a controlled study. Pediatr Dent. 1995; 17:26-30
Arkutu N, Gadhia K, McDonald S, Malik K, Currie L Amelogenesis imperfecta: the orthodontic perspective. Br Dent J. 2012; 212:485-489
Crawford PJM, Aldred M, Bloch-Zupan A Amelogenesis imperfecta. Orphanet J Rare Dis. 2007; 2
McDonald S, Arkutu N, Malik K, Gadhia K, McKaig S Managing the paediatric patient with amelogenesis imperfecta. Br Dent J. 2012; 212:425-428
Seow WK Clinical diagnosis and management strategies of amelogenesis imperfecta variants. Pediatr Dent. 1993; 15:384-393
Malik K, Gadhia K, Arkutu N, McDonald S, Blair F The interdisciplinary management of patients with amelogenesis imperfecta – restorative dentistry. Br Dent J. 2012; 212:537-542
Watson TF, Bartlett DW Adhesive systems: composites, dentine bonding agents and glass ionomers. Br Dent J. 1994; 176:227-233
Shields ED, Bixler D, El-Katrawy AM A proposed classification for heritable human dentine defects with a description of a new entity. Arch Oral Biol. 1973; 18
Witkop CJ Hereditary defects in enamel and dentin. Acta Genet Stat Med. 1957; 7:236-239
Moundori-Andritsakis H, Kourtis S, Andritsakis D All-ceramic restorations for complete-mouth rehabilitation in dentinogenesis imperfecta: a case report. Quintessence Int. 2002; 33:656-660
Guideline on Dental Management of Heritable Dental Developmental Anomalies. 2013; 35:13-14
Waltimo J, Ranta H, Lukinmaa PL Ultrastructure of dentine matrix in heritable dentine defects. Scanning Microsc. 1995; 9:85-98
O'Connell A, Marini J Evaluation of oral problems in an osteogenesis imperfecta population. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999; 87:189-196
Pettiette MT, Wright JT, Trope M Dentinogenesis imperfecta: endodontic implications. Case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998; 86:733-737
Sapir S, Shapira J Dentinogenesis imperfecta: an early treatment strategy. Am Acad Pediatr Dent. 2001; 23:232-237
Dhaliwal H, McKaig S Dentinogenesis imperfecta – clinical presentation and management. Dent Update. 2010; 37:364-371
Schwartz S, Joseph C, Iera D, Vu DD Bisphosphonates, osteonecrosis, osteogenesis imperfecta and dental extractions: a case series. J Can Dent Assoc. 2008; 74:537-542
Yip HK, Smales RJ Oral rehabilitation of young adults with amelogenesis imperfecta. Int J Prosthodont. 2003; 16:345-349
Cogulu D, Becerik S, Emingil G, Hart PS, Hart TC Oral rehabilitation of a patient with amelogenesis imperfecta. Pediatr Dent. 2009; 31:523-527
Sengun A, Özer F Restoring function and aesthetics in a patient with amelogenesis imperfecta: a case report. Quintessence Int. 2003; 33:199-204
Faria-e-Silva AL, De Moraes RR, Menzes Mde S, Capanema RR, De Moura AS, Martelli H Hardness and microshear bond strength to enamel and dentin of permanent teeth with hypocalcified amelogenesis imperfecta. Int J Paediatr Dent. 2011; 21:314-320
Lindunger A, Smedberg JI A retrospective study of the prosthodontic management of patients with amelogenesis imperfecta. Int J Prosthodont. 2005; 18:189-194
Kostoulas I, Kourtis S, Andritsakis D, Doukoudakis A Functional and esthetic rehabilitation in amelogenesis imperfecta with all-ceramic restorations: a case report. Quintessence Int. 2005; 36:329-338
Turkun LS Conservative restoration with resin composites of a case of amelogenesis imperfecta. Int Dent J. 2005; 55:38-41
Venezie RD, Vadiakas G, Christensen JR, Wright JT Enamel pre-treatment with sodium hypochlorite to enhance bonding in hypocalcified amelogenesis imperfecta: case report and SEM analysis. Pediatr Dent. 1994; 16:433-436
Gallusi G, Libonati A, Campanella V SEM-morphology in dentinogenesis imperfecta type II: microscopic anatomy and efficacy of a dentine bonding system. Eur J Paediatr Dent. 2006; 7:(1)9-17
Harley KE, Ibbetson RJ Dental anomalies – are adhesive castings the solution?. Br Dent J. 1993; 174:15-22
Rios D, Falavinha A, Tenuta L, Machado M Osteogenesis imperfect and dentinogenesis imperfecta: associated disorders. Quintessence Int. 2005; 36:695-701
Sabatini C, Guzmán-Armstrong S A conservative treatment for amelogenesis imperfecta with direct resin composite restorations: a case report. J Esthet Restor Dent. 2009; 21:161-170
Patel M, McDonnell ST, Iram S, Chan MF Amelogenesis imperfecta – lifelong management. Restorative management of the adult patient. Br Dent J. 2013; 215:(9)449-457
Nathwani NS, Kelleher M Minimally destructive management of amelogenesis imperfecta and hypodontia with bleaching and bonding. Dent Update. 2010; 37:170-179
Restorative indications for porcelain veneer restoration.London: Royal College of Surgeons of England; 1997
Nalbandian S, Millar BJ The effect of veneers on cosmetic improvement. Br Dent J. 2009; 207:(2)
Meijering AC, Creugers NH, Roeters FJ, Mulder J Survival of three types of veneer restorations in a clinical trial: a 2.5-year interim evaluation. J Dent. 1998; 26:563-568
Millen C, Bhatia K, Ibbetson R Laboratory aspects of zirconia restorations. Dent Update. 2012; 39:342-354
Siadat H, Alikhasi M, Mirfazaelian A Rehabilitation of a patient with amelogenesis imperfecta using all-ceramic crowns: a clinical report. J Prosthet Dent. 2007; 98:85-88
Walls AW, Nohl FS, Wassell RW Crowns and other extra-coronal restorations: resin-bonded metal restorations. Br Dent J. 2002; 193:135-142
Heij DG, Opdebeeck H, van Steenberghe D, Kokich VG, Belser U, Quirynen M Facial development, continuous tooth eruption, and mesial drift as compromising factors for implant placement. Int J Oral Maxillofac Implants. 2006; 21:867-878
Seymour DW, Chan MF, Nixon PJ Dentinogenesis imperfecta: full-mouth rehabilitation using implants and sinus grafts – a case report. Dent Update. 2012; 39:498-504
Full-mouth rehabilitation for a patient with dentinogenesis imperfecta: a clinical report. 2013.
Zola MB Staged sinus augmentation and implant placement in a patient with osteogenesis imperfecta. J Oral Maxillofac Surg. 2000; 58:443-447
Payne MA, Postlethwaite KR, Smith DG, Nohl FS Implant-supported rehabilitation of an edentate patient with osteogenesis imperfecta: a case report. Int J Oral Maxillofac Implants. 2008; 23:947-952
Jensen L, Brox H, Storhaug K, Ambjørnsen E, Støvne S, Bjørnland T Dental implants in patients with osteogenesis imperfecta: a retrospective and prospective study with review of the literature. Oral Surg. 2011; 4:105-114
Visram S, McKaig S Amelogenesis imperfecta – clinical presentation and management: a case report. Dent Update. 2006; 33:612-616
Takagi Y, Koshiba H, Kimura O, Kuboki Y, Sasaki S Dentinogenesis imperfecta: evidence of qualitative alteration in the organic dentin matrix. J Oral Pathol. 1980; 9:201-209
van Waas MA, Jonkman RE, Kalk W, van't Hof MA, Plooij J, Van Os JH Differences two years after tooth extraction in mandibular bone reduction in patients treated with immediate overdentures or immediate complete dentures. J Dent Res. 1993; 72:1001-1004
Ghodsi S, Rasaeipour S, Vojdani M Oral rehabilitation of a patient with amelogenesis imperfecta using removable overlay denture: a clinical report. J Contemp Dent Pract. 2012; 13:227-231
Lynch CD Successful removable partial dentures. Dent Update. 2012; 39:(2)118-126
Alani A, Bishop K Dens invaginatus. Part 1: classification, prevalence and aetiology. Int Endod J. 2008; 41:1123-1136
Hovland EJ, Block RM Non-recognition and subsequent endodontic treatment of dens invaginatus. J Endodont. 1977; 3:360-362
Hülsmann M Dens invaginatus: aetiology, classification, prevalence, diagnosis, and treatment considerations. Int Endod J. 1997; 30:79-90
Conklin WW Bilateral dens invaginatus in the mandibular incisor region. Oral Surg Oral Med Oral Pathol. 1978; 45:905-908
Grahnen H, Lindahl B, Omnell K Dens invaginatus: a clinical roentgenological and genetical study of permanent lateral incisors. Odontol Revy. 1959; 10:115-137
Oehlers FA Dens invaginatus (dilated composite odontome). I. Variations of the invagination process and associated anterior crown forms. Oral Surg Oral Med Oral Pathol. 1957; 10:(11)1204-1218
Rotstein I, Stabholz A, Heling I, Friedman S Clinical considerations in the treatment of dens invaginatus. Endod Dent Traumatol. 1987; 3:249-254
Seow WK Diagnosis and management of unusual dental abscesses in children. Aust Dent J. 2003; 48:156-168
Bimstein E, Shteyer A Dilated type of dens invaginatus in the permanent dentition. ASDC J Dent Child. 1976; 43:410-413
Duncan WK, Helpin ML Bilateral fusion and gemination: a literature analysis and case report. Oral Surg Oral Med Oral Pathol. 1987; 64:82-87
Aguiló L, Gandia JL, Cibrian R Primary double teeth. A retrospective clinical study of their morphological characteristics and associated anomalies. Int J Paediatr Dent. 1999; 9:175-183
Neville BW, Damm DD, Allen CM, Bouqout JE, 2nd edn. Philadelphia: Saunders; 2002
Alvarez I, Creath CJ Radiographic considerations for supernumerary tooth extraction: report of case. ASDC J Dent Child. 1995; 62:141-144
Uÿs H, Morris D ‘Double’ teeth – a diagnostic conundrum. Dent Update. 2005; 32:237-239
Killian CM, Croll TP Dental twinning anomalies: the nomenclature enigma. Quintessence Int. 1990; 21:571-576
Schuurs AH, van Loveren C Double teeth: review of the literature. ASDC J Dent Child. 2000; 67:313-325
Buenviaje TM, Rapp R Dental anomalies in children: a clinical and radiographic survey. ASDC J Dent Child. 1984; 51:42-46
Crawford NL, North S, Davidson LE Double permanent incisor teeth: management of three cases. Dent Update. 2006; 33:608-610
Li RW Clinical variants in tooth number and crown form: a report of bilateral double teeth associated with a talon cusp. Dent Update. 2002; 29
Taloumis LJ, Nishimura RS Treatment of an unusual instance of fusion with a talon cusp. Gen Dent. 1989; 37:208-210
Velasco LF, de Araujo FB, Ferreira ES, Velasco LE Esthetic and functional treatment of a fused permanent tooth: a case report. Quintessence Int. 1997; 28:677-680
Gautam G, Kumari VS, Jayashankar CM, Hadge P, Garg G Interdisciplinary management of dental anomalies: fusion and supernumerary teeth. Orthodontics. 2011; 12:140-147
Garattini G, Crozzoli P, Brenna F Bilateral dental fusion of the upper central incisors: a multidisciplinary approach. J Esthet Dent. 1999; 11:149-154
Thomas MB, Greenhalgh CM, Addy L ‘Double-veneers’ – a novel approach to treating macrodontia. Dent Update. 2008; 35:479-484
Hülsmann M, Bahr R, Grohmann U Hemisection and vital treatment of a fused tooth – literature review and case report. Endod Dent Traumatol. 1997; 13:253-258
Rada RE Perio-prosthetic rehabilitation of a geminated central incisor. Pract Periodontics Aesthet Dent. 1991; 3:23-26
Türkaslan S, Gökçe HS, Dalkız M Esthetic rehabilitation of bilateral geminated teeth: a case report. Eur J Dent. 2007; 1:188-191
There are a number of anomalies that affect the structure of the dental hard tissues which impact upon the form, function and aesthetics of the dentition. Understanding the challenges these conditions pose will enable dentists to manage the functional and aesthetic problems with restorative techniques better. This article will present cases that demonstrate the different conditions, the restorative challenges experienced and a variety of restorative treatments in the management of these conditions.
CPD/Clinical Relevance: Awareness of different anomalies affecting tooth structure that may present to the dental practitioner is necessary. Clinicians should appreciate the specific restorative challenges that may arise in treating such patients and the possible treatment options that may be available.
Article
There are a number of local and systemic conditions that affect the structure of the dental hard tissues that the GDP may come across in practice. This includes anomalies such as amelogenesis imperfecta and dentinogenesis imperfecta, which are well known to those specialists who work in secondary care environments.
These conditions are developmental abnormalities and can affect the form, function and aesthetics of the whole dentition, which can potentially have a psychological impact on the patient. Other anomalies that affect one or two teeth, such as dens invaginatus or fusion, are no less important simply because they are more localized.
These conditions often appear early in life and require immediate management and treatment where necessary. As patients get older they may be referred for restorative specialist advice and treatment. Treatment can be challenging, complex and prolonged. Even when treatment is complete the patient will require long-term review and maintenance.
Although several conditions can affect tooth structure, the aim of this article is to provide an overview of selected anomalies that affect the dental hard tissues and to present case examples of the range of restorative treatment performed on this patient group. Many of these patients are treated in specialist settings; however, it is likely that general dental practitioners will come into contact with these patients before, during or after treatment phases. This paper will highlight strategies to overcome specific challenges with the restorative aspect of their dental care.
Dental developmental conditions
Table 1 lists a variety of conditions that can affect the quality and quantity of dental hard tissue and the morphology of teeth. The remainder of this article will focus on the features and management of the following conditions:
Amelogenesis imperfecta (AI) is a hereditary genetic disorder which affects enamel formation and is not associated with systemic abnormality or disease.1 The condition affects the formation of the enamel matrix or the enamel mineralization process. The changes to enamel formation are normally due to single gene mutations that affect enamel matrix proteins (amelogenin, enamelin and amelobastin), which are used to produce enamel during amelogenesis.2,3 The inheritance pattern can be autosomal dominant, autosomal recessive or X-linked.4
In general, AI affects both the primary and permanent dentitions. The estimated frequency of AI ranges from 1:700 to 1:14,000, depending on the population studied.5
There has been a number of different classifications of AI that have included genetic pattern, as well as clinical and radiological features. The popular Witkop classification has 15 different variants that have been put together into four groups based on the inheritance pattern (Table 2).4
Type I Hypoplastic
Type IA Hypoplastic, pitted autosomal dominant
Type IB Hypoplastic, local autosomal dominant
Type IC Hypoplastic, local autosomal recessive
Type ID Hypoplastic, smooth autosomal dominant
Type IE Hypoplastic, smooth X-linked dominant
Type IF Hypoplastic, rough autosomal dominant
Type IG Enamel agenesis, autosomal recessive
Type II Hypomaturation
Type IIA Hypomaturation, pigmented autosomal recessive
Type IIB Hypomaturation, X-linked recessive
Type IIC Snow-capped teeth, X-linked
Type IID Snow-capped teeth, autosomal dominant
Type III Hypocalcified
Type IIIA Autosomal dominant
Type IIIB Autosomal recessive
Type IV Hypomaturation-hypoplastic with taurodontism
Type IVA Hypomaturation-hypoplastic with taurodontism, autosomal dominant
Type IVB Hypoplastic-hypomaturation with taurodontism, autosomal dominant
In Type I hypoplastic AI, there is a defect in the enamel matrix formation but mineralization of the enamel matrix is normal. This creates a normal enamel layer, but of a reduced thickness.
In Type II hypomaturation AI and Type III hypocalcified AI, there is a defect in the maturation of the enamel but the enamel is of normal thickness and is of a softer consistency.
In Type IV hypomaturationhypoplastic with taurodontism, this appears similar to Types II and III but there is evidence of taurodontism.
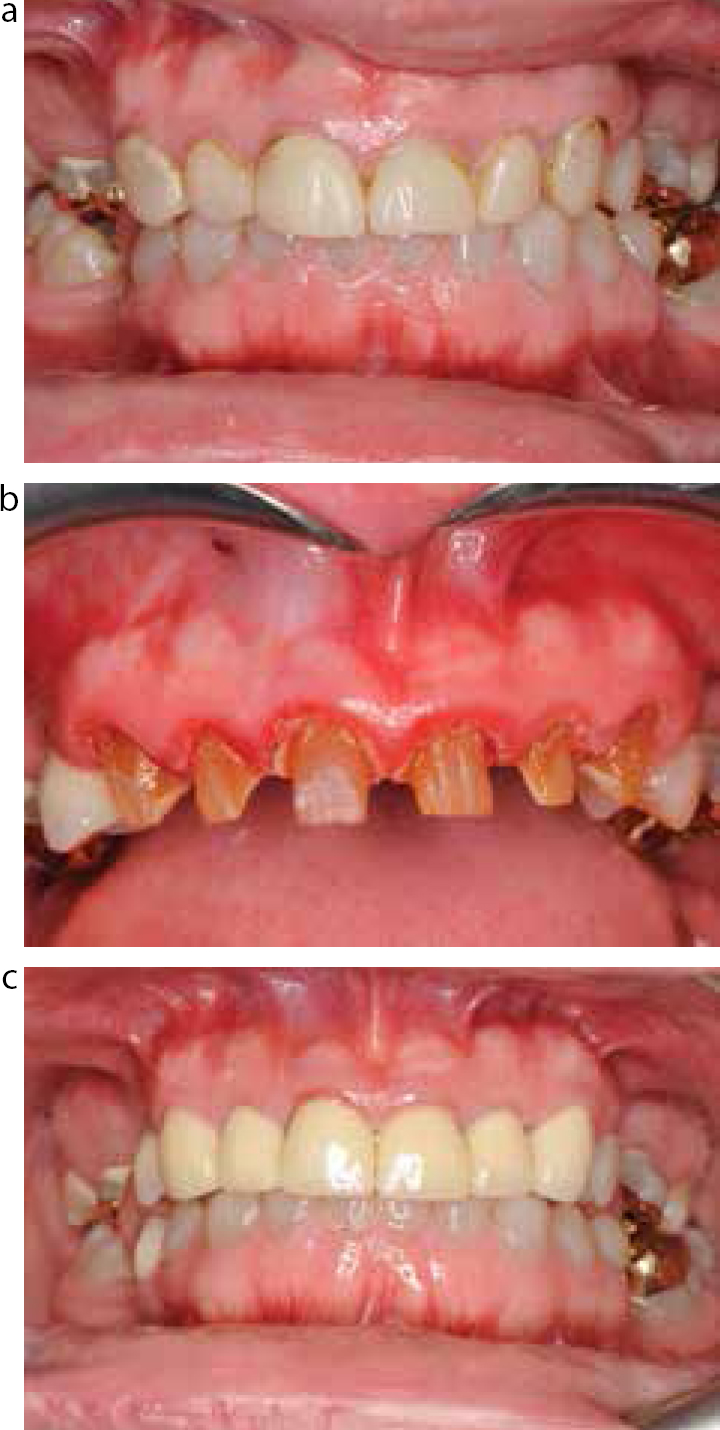
The clinical presentation is variable and can range from minimal pitting, discoloration and minimal breakdown of enamel to severe pitting, discoloration and rapid breakdown of enamel. Figure 1 shows the discoloration and form of a patient's dentition suffering from a severe form of AI. AI has been associated with other dental anomalies, these include:3,4,6,7,8
Taurodontism;
Congenitally missing teeth;
Anterior open bites (reported to occur in 50% of patients with AI);
Pulpal calcification;
Failed tooth eruption and impaction of permanent teeth;
Crown and root resorption.
Figure 1. Patient suffering from severe AI.
This range of features poses a number of specific challenges for the restorative dentist. Table 3 summarizes the restorative challenges associated with AI.
Accelerated toothwear10 - potentially leading to loss of occlusal vertical dimension and/ or loss of interocclusal space11
Unerupted and ectopic teeth
Dentinogenesis imperfecta
Dentinogenesis imperfecta (DI) is a hereditary genetic disorder which affects dentine formation. It can occur in isolation or be associated with osteogenesis imperfecta (OI).
Shields et al classified DI into three types (Table 4).14
Type
Presentation
Type I (DI-I)
The dental manifestation of osteogenesis imperfecta
Type II (DI-II)
Classical hereditary opalescent dentine (essentially the same clinical radiographic and histological features as DI Type 1 but without osteogenesis imperfecta)
Type III (DI-III)
Brandywine isolate opalescent dentine
The incidence of DI is around 1:8,000.15 Type I DI appears in 20–40% of patients with OI.16
In general, it affects all the teeth in both the primary and permanent dentitions.
Type I is caused by mutations in collagen genes (COL1A1 and COL1A2), with OI being an autosomal dominant condition. DI Type II and Type III are caused by mutations in the dentine sialophosphoprotein gene (DSPP) and have an autosomal dominant inheritance pattern.17
Dentine is the first dental hard tissue to form and is produced by the odontoblasts. In patients with DI the dentine is weaker. This is due to the calcospherites being unable to fuse during dentine matrix mineralization and leads to hypomineralized areas of interglobular dentine. Progressive tooth surface loss is also caused by the loss of the scalloping at the enamel dentine junction, the scalloping acting to hold the two tooth structures together mechanically. Without this enamel is readily chipped off the underlying dentine.18
The clinical presentation and severity of DI is variable. The teeth are often discoloured (amber, grey, purple to bluish translucent discoloration) and show structural defects such as bulbous crowns. Radiographically the teeth may appear to have small pulp chambers and there is often progressive calcification of the pulp chamber. The teeth may also undergo spontaneous loss of pulpal vitality without any symptoms, and with progressive calcification of the pulp chamber endodontic treatment can be difficult if not impossible.
Figure 2 shows the classic radiographic features of a patient with Type II DI, reduced pulp chambers and bulbous crowns. The underlying defect of mineralization often results in loss of the overlying enamel, leaving exposed weakened dentine which is prone to wear. This wear is often compensated for through continued alveolar growth that results in an over-closed appearance, lack of tooth display and decreased interocclusal space.
Figure 2. OPG of patient suffering from DI.
DI has been associated with other dental anomalies such as microdontia, malocculsions (including Class III malocclusion), posterior crossbites and open bites in Type I DI.19
Table 5 summarizes the restorative challenges associated with DI.
Endodontic treatment difficulty due to obliteration of the pulp chambers and root canals, short canals, abnormal dentine mineralization20,21
Spontaneous abscesses may occur in the absence of any coronal pathology21
Accelerated toothwear20 - potentially leading to loss of occlusal vertical dimension and/ or loss of interocclusal space
Type I DI will have OI - additional care needs to be undertaken when causing trauma to bone, eg extraction, implant placement due to risk of bone fracture. Some patients may be taking bisphosphonates and therefore at risk of bisphosphonate-induced osteonecrosis of the jaw (BRONJ)24
Shortened root length - therefore crown lengthening procedures may be contra-indicated16
Aims of treatment in patients with AI and DI
The aims of treatment include:
Removing sources of infection or eliminating pain;
Restoring aesthetics;
Protecting teeth from wear and caries;
Maintaining or improving function;
Improving malocclusions where required; and
Preservation of tooth tissue where possible.
Treatment options vary and are dependent on a number of factors but are heavily influenced by the severity of the condition and the patient's presenting complaint. In general terms, the severity of AI and DI will affect the outcome and prognosis of restorative treatment owing to the physical properties of the tooth structure.
Treatment may often be complex, extensive and will require long-term care and maintenance, of which the patient needs to be aware. The general management of these patients is often complicated by behaviour and attitude to dental treatment. Some patients are understandably introverted and lack confidence because of their dental appearance. The treatment of these patients, like any other patient, should be minimally invasive using adhesive techniques where possible,25,26,27 however, treatment of AI and DI using adhesive techniques can be challenging, if not impossible in some cases.
Prosthetic treatment options in patients with AI and DI
Resin bonding and AI and DI
All adhesive techniques are complicated by a patient's poor oral hygiene. This is compounded by lack of motivation to clean what are seen as ‘ugly’ teeth and, in the case of AI, rough surfaces that are plaque retentive. In patients with AI, teeth are often very sensitive, which sometimes means that local analgesia is needed even for very simple additive composite resin techniques.
The difficultly in patients with AI is being able to attain a predictable adhesive bond to the tooth structure and this can be compromised,28 but there is evidence to show that bonding to teeth with AI can be successfully carried out.29,30,31 Predictable bonding is also affected by the microdontia noted in both conditions, which reduces the total surface area.
There is some evidence suggesting that teeth affected by AI have an atypical etch pattern and thus have reduced bond strength from enamel to the composite resin. This study also showed that adequate bonding can be achieved with the pre-treatment of hypocalcified AI teeth with sodium hypochlorite prior to adhesive bonding. This improved the bond strengths attained with resin-based materials.32
There are two concerns with bonding in patients with DI. First, bonding to enamel may not result in a predictable restoration since the enamel may itself detach from underlying dentine, although this varies from case to case. Secondly, the altered structure of dentine itself may affect the formation of a hybrid layer that is required in conventional dentine bonding techniques. A study by Gallusi et al showed that a hybrid layer could not be created in dentine in DI Type II affected teeth with an adhesive system and therefore seemed to be less effective than on normal substrates.33
However, adhesive bonding and adhesive restorations in patients with DI have been proven to be successful.34,35 Some clinicians have recommended the use of resin-modified GIC-based bonding agents rather than conventional resin-based adhesives as they produce true chemical bonds to metal ions rather than the hybrid layer. There is some evidence to show glass ionomer cements are as effective as resin-based cements in cementation of cast restorations in both DI and AI.34
In general, adhesive restorations are commonly used to treat patient with AI and DI and have been shown to be successful.27,31,36 In practical terms, however, in severe forms of AI and DI and where repeated debonding or loss of restorations occur, full coverage restoration may need to be considered. The severity of AI and DI will affect the outcome of restorative treatment and, in particular, the quality of the dentine substrate and ability to form a hybrid layer. Enamel loss due to weakness at the ADJ will affect restoration longevity where restoration margins are within enamel only.
Veneers
Veneers are commonly used on anterior teeth in AI and DI patients. They allow good aesthetics whilst being relatively conservative of tooth tissue in comparison to crowns.37 Even so, preparation is required and can be destructive of reasonably sound tooth tissue.38
Possible indications for the use of veneers in AI and DI patients are to restore areas of wear and to improve aesthetics, particularly if direct composite has been tried and proved unsuccessful.23,37 They are also generally indicated for hypoplastic and discoloured teeth, when other techniques have failed to create a satisfactory clinical result.39
Veneers tend to be more useful in AI than DI patients due to the issues with bonding and the underlying discoloration of the dentine in DI patients.
Veneers can be either composite or porcelain, and both have proved to be aesthetic, with high patient satisfaction.40,41
Obtaining good aesthetics with veneers can be difficult in patients, particularly when the tooth structure is dark. In a minority of cases the veneers are unable to mask the discoloration and lead to compromised aesthetics. Techniques to alleviate this are for the porcelain veneers to have a layer of opaque porcelain incorporated into the restoration, or the use of an opaque resin cement. They can be used separately or together to help disguise this discoloration but lead to a loss of translucency which can detract from the final appearance.37 Another option, which is yet to be validated with long-term clinical data, is to use zirconia for the coping of the veneer, which is overlaid with feldspathic porcelain. Zirconia can be opaque which enables the blocking out of the underlying tooth colour, however, due to zirconia being inert and lacking silica, bonding to zirconia is difficult.42Figure 3 shows the comprehensive restoration of a patient with AI following previous failure of interim composite restorations. Treatment included surgical crown lengthening with osseous recontouring in the maxilla to improve the gingival contour. This was followed by the placement of zirconia-reinforced veneers anteriorly and full coverage restorations posteriorly.
Figure 3.
(a) Pre-operative and (b) postoperative views of a patient with AI following a comprehensive rehabilitation.
The same issue with bonding applies as with direct placement of composite. Direct composite placement can be considered as the treatment is reversible, reasonably quick and allows preservation of tooth tissue. It is useful in young growing patients to allow gingival maturation and avoid the risk of pulpal pathology in patients with larger pulps.
Crowns/onlays in patients with AI and DI
Onlays and crowns can be used to protect the underlying tooth structure. They can be placed conforming to the existing occlusion or placed to compensate for loss of occlusal vertical dimension.
Conventional crowns have been shown to be successful in patients with AI and have also been shown to be predictable and durable, but have the disadvantage of being destructive of tooth tissue.25 There are risks associated with placing crowns in AI patients that include cementation failure, material fracture, caries and endodontic treatment,29,43 all of which are common complications of crowning teeth in the general population.
Where gingival asymmetry, excess gingival display or microdontia is an issue, then crown lengthening surgery may be considered (Figure 3). This is complicated by the close proximity of the roots which are often spindly and the inevitable increased sensitivity following surgery. However, this may be contra-indicated in teeth with short roots, common in DI patients.16
In posterior teeth where protection of the tooth structure is required in AI and DI patients, gold onlays bonded with resin composite or full coverage gold veneer crowns can be provided. They have been proven to be successful in these patients and help minimize toothwear and maintain the occlusal vertical dimension.12,44
Adhesive restorations, such as dentine-bonded crowns and gold onlays cemented with resin composite, rely more on the adhesion than the mechanical retentive features of tooth preparation,45 and with this have reduced tooth preparation.
In anterior and posterior teeth for patients with aesthetic concerns, metal-ceramic crowns may be considered. Metal-ceramic crowns should be designed to restrict porcelain to aesthetic areas and metal in non-aesthetic areas to preserve tooth tissue.37 Other options include all-ceramic dentine-bonded crowns, which can be a more conservative aesthetic treatment option for the anterior region.12,37 High strength all-ceramic crowns with zirconia and alumina have been used in patients with AI,43 but require heavier preparations, which could lead to pulpal pathology.37 Zirconia crowns have the advantage of an opaque substructure which can be useful to block out underlying orange/brown discoloration, more translucent ceramics such as alumina, or lithium disilicate which may be inadequate in regards to this.
Crowns are not recommended in DI-affected teeth with short thin roots and marked cervical constrictions.44 They may also not be recommended in teeth severely affected by the condition. Prior to the placement of crowns it is essential that an assessment of tooth vitality be made, since DI-affected teeth often become necrotic with asymptomatic apical periodontitis. These teeth should not be root treated but planned for extraction as a canal location is often impossible.
It is the recommendation of the authors that, wherever possible, minimal preparation be carried out to preserve as much tooth tissue as possible and, although adhesion to AI- and DI-affected teeth isn't as predictable, it has been shown to be successful and allows tooth preparation to be more conservative. Timing of treatment in relation to the patient's age needs to be considered. Where possible, extra-coronal restorations should only be placed in patients at least 18 years old and, where feasible, as late as possible. This is due to the higher risk of loss of pulpal vitality in AI patients, that the tooth will be put into the restorative cycle, and the high likelihood of requiring multiple replacements in patients of a young age. Also, the gingival tissues do not fully mature until the end of the second decade.
Implants
There is no evidence to suggest the need for any special consideration on implant provision in patients with AI. Provision of implants in patients with AI will usually occur in patients with advanced cases where teeth are deemed unrestorable through caries or severe microdontia. Teeth which remain unerupted and cannot be extruded orthodontically may need removal.
Implant treatment can only be considered in patients who have stopped growing,46 as it can lead to infraocclusion of the implant restoration. It has been suggested by Patel et al that implant treatment may not be the ideal choice in the first instance for young adult patients with AI.37 This is due to the fact that further treatment will be required in later life and the possibility of improved outcomes in implant treatment in the future due to the constant improvements in technology.
Specific challenges in AI may relate to the occlusion and limited interproximal space for implant placement due to narrow spindly roots and narrow clinical crowns. In DI patients with Type II or III DI, the bone quantity and quality is the same as in an unaffected individual,47 but there are a limited number of studies on dental implant provision in DI patients.48
Patients with Type I DI have OI but, despite this, implant placement has been shown to be successful in OI patients49,50 with similar success rates to non-OI patients,51 but there is limited evidence available. Type I DI patients may also be on bisphosphonate (BP) medication due to OI. The use of BP medication comes with the risk of BP-induced osteonecrosis of the jaw (BRONJ).
In DI patients, the bone volume is often reduced, particularly in terms of width. It is the authors' opinion that this is related to short roots and, therefore, a lack of alveolar development. It is often necessary to perform a guided bone regeneration procedure at the time of implant placement.
Overall, careful planning of treatment is required to ensure optimal results are attained. Figure 4 shows the management of a patient with DI following repeated failure of anterior veneers and fracture of premolars on the right side. Initial management included increasing the vertical dimension with direct composite veneers placed on the mandibular incisors and canines. Later two implant-supported crowns were placed and restored in the first premolar regions on the right side followed by the placement of six porcelain-bonded crowns to restore the maxillary anterior teeth. Note the discoloration of the prepared maxillary incisors.
Figure 4. Patient with dentinogenesies imperfecta (a) pre-operatively, (b) following crown preparation and (c) post-operatively.
Removable prosthesis
In the past, treatment of AI and DI patients often involved the extraction of teeth and provision of a partial or complete denture.37 With advances in dental materials and techniques, treatment can be more conservative with benefit to the patient.52
Even in advanced cases, and when teeth are deemed unrestorable, they can be retained with provision of an overdenture or onlay denture.23
Dentures are particularly useful in cases of extensive toothwear,53 as they may be used to protect remaining tooth tissue, and maintain occlusal face height.21,23
They may also be used to help retain teeth and be of particular importance in young patients who are not of a suitable age or are in the planning stages of treatment for more invasive treatment, such as implants. The retention of teeth helps to preserve alveolar bone.54 Until growth is complete, the treatment of choice for the replacement of missing teeth in DI20 and AI may be dentures.
A removable partial denture has been shown to be a good temporary or permanent solution, particularly in patients with low aesthetic concerns or medical limitations.55 This may include Type I DI patients who have OI, where restorative treatment options are restricted to implants or a removable prosthesis for tooth replacement. These patients with OI are at risk of bone fractures and BRONJ (if taking bisphosphonates) if implants are placed. The risk and benefits of providing an implant-retained prosthesis and a removable prosthesis need to be weighed up. The disadvantages of dentures include: increased plaque retention with the potential consequences, including gingivitis; periodontal disease or caries; trauma from denture components and decreased patient tolerance.56
However, dentures are not usually the first choice of treatment in AI and DI patients, but do serve a role, and can provide temporary or definitive treatment in some patients.
Developmental conditions affecting size or shape of the teeth
Dens invaginatus
Dens invaginatus is a development abnormality resulting in malformation of teeth due to invagination of the enamel organ into the dental papilla during tooth development. It has also been called dens-in-dente and an invaginated odontome. The exact aetiology of dens invaginatus is unknown but it has been proposed that there is likely to be a genetic cause.57
The prevalence of dens invaginatus ranges from 0.04–10%.58 The permanent maxillary lateral incisor is the most frequently affected tooth,59 with posterior teeth less likely to be affected.60 Bilateral occurrences are common, accounting for 43% of cases,61 so contralateral teeth should be routinely assessed.
Teeth affected can present with an infolding of enamel and dentine with variable degrees of severity. This ranges from the invagination affecting the amelo-cemental junction only, to extension into the pulp cavity and extending into the root, which can sometimes form a second apical foramen.
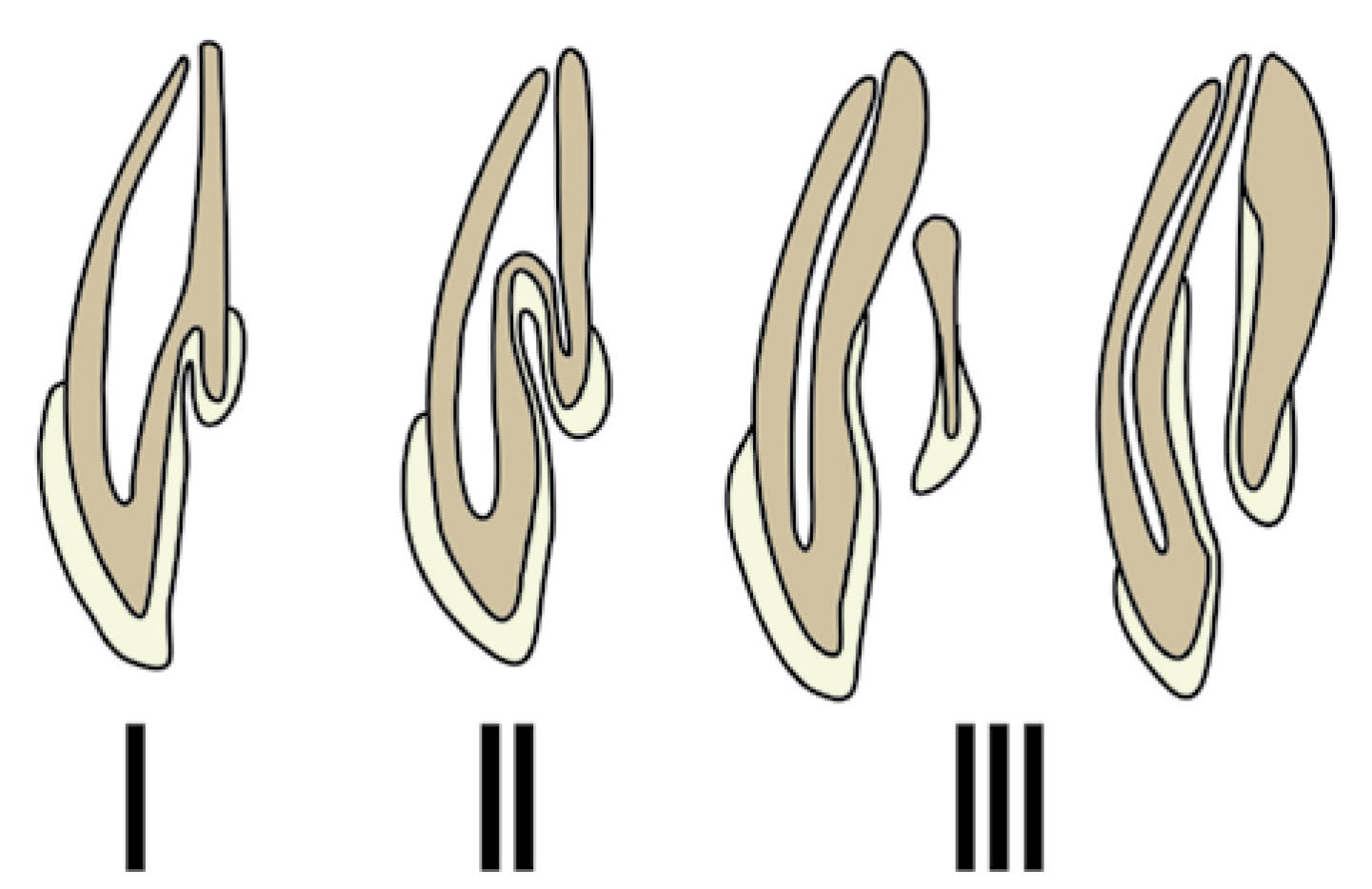
The most commonly used classification is proposed by Oehlers62 and is categorized into three types (Table 6 and Figure 5).
Type
Presentation
Type I
An enamel-lined minor form occurring within the confines of the crown not extending beyond the amelocemental junction.
Type II
An enamel-lined form which invades the root but remains confined as a blind sac. It may or may not communicate with the dental pulp.
Type III
A form which penetrates through the root perforating at the apical area showing a ‘second foramen’ in the apical or in the periodontal area. There is no immediate communication with the pulp. The invagination may be completely lined by enamel, but frequently cementum will be found lining the invagination.
Figure 5. Oehlers classification of invaginated teeth (1957).62
Teeth affected with dens invaginatus are associated with an increased risk of developing pulpal pathology,63 and this may occur without evidence of any obvious caries or history of trauma.64 It is assumed that the infection results from increased plaque accumulation within narrow grooves that are impossible to clean. Dens invaginatus has been associated with other dental anomalies and disturbances of dental development59 including:
Microdontia;
Macrodontia;
Hypodontia;
Oligodontia;
Taurodontism;
Gemination and fusion;
Supernumerary teeth;
Amelogenesis imperfecta;
Invagination in an odontome;
Multiple odontomes;
Coronal agenesis;
Williams syndrome.
Table 7 summarizes the restorative challenges associated with dens invaginatus.
Restorative Challenges Associated with Dens Invaginatus
Endodontic treatment difficulty - due abnormal pulp chamber, and root canal anatomy, there may also be a separate apical or lateral foramen59
'Double teeth'
During tooth development, there can be developmental abnormality whereby a ‘double tooth’ is formed. These ‘double teeth’ can be classified as: gemination, fusion or concrescence.66,67,68
Gemination is caused by an attempt of a tooth germ to divide unsuccessfully during development.69,70 It may result in the formation of a large tooth with a bifid crown or two crowns and have a single root and one root canal.71,72 It may also result in varying depths of coronal notches or grooves. In these cases, the normal number of teeth is observed if the affected tooth is counted as one.66
Fusion is caused by the combination of two tooth germs during development.70 It may result in the formation of either a large tooth with a bifid crown or roots and may involve the entire length of the tooth or the roots only.68 In these cases, there are usually a reduced number of teeth observed if the affected tooth is counted as one, unless there is a supernumerary tooth.73
Concrescence is the union of two adjacent teeth by the cementum.74
The prevalence of gemination or fusion for the primary dentition is between 0.4–0.9%, and for the permanent dentition averages 0.2%.75,76
The aetiology of gemination/fusion is unknown, but there is a potential genetic cause.70
Gemination is more common in the anterior maxillary dentition and fusion in the anterior mandibular dentition.66Table 8 shows the restorative challenges associated with 'double teeth'.
Malocclusions - spacing in the dental arch may result from the union78 and crowding may result if a supernumerary is involved79
Prosthetic treatment options for patients with dens invaginatus and ‘double teeth’
Resin bonding and veneers
Bonding is the same as for a normal tooth as the enamel and dentine are structurally normal. The major challenge is correction of the unusual aesthetic appearance. It is easier to make a microdont appear of normal dimensions than to camouflage a tooth with macrodontia. Therefore, creative techniques are required that include reduction of bulbosities and modification of buccal grooves that create the desired illusion. These cases are best planned using laboratory diagnostic wax-ups and careful technician–dentist interaction to plan the result. Showing the patient the planned aesthetic changes as part of a wax-up is part of the consent process.
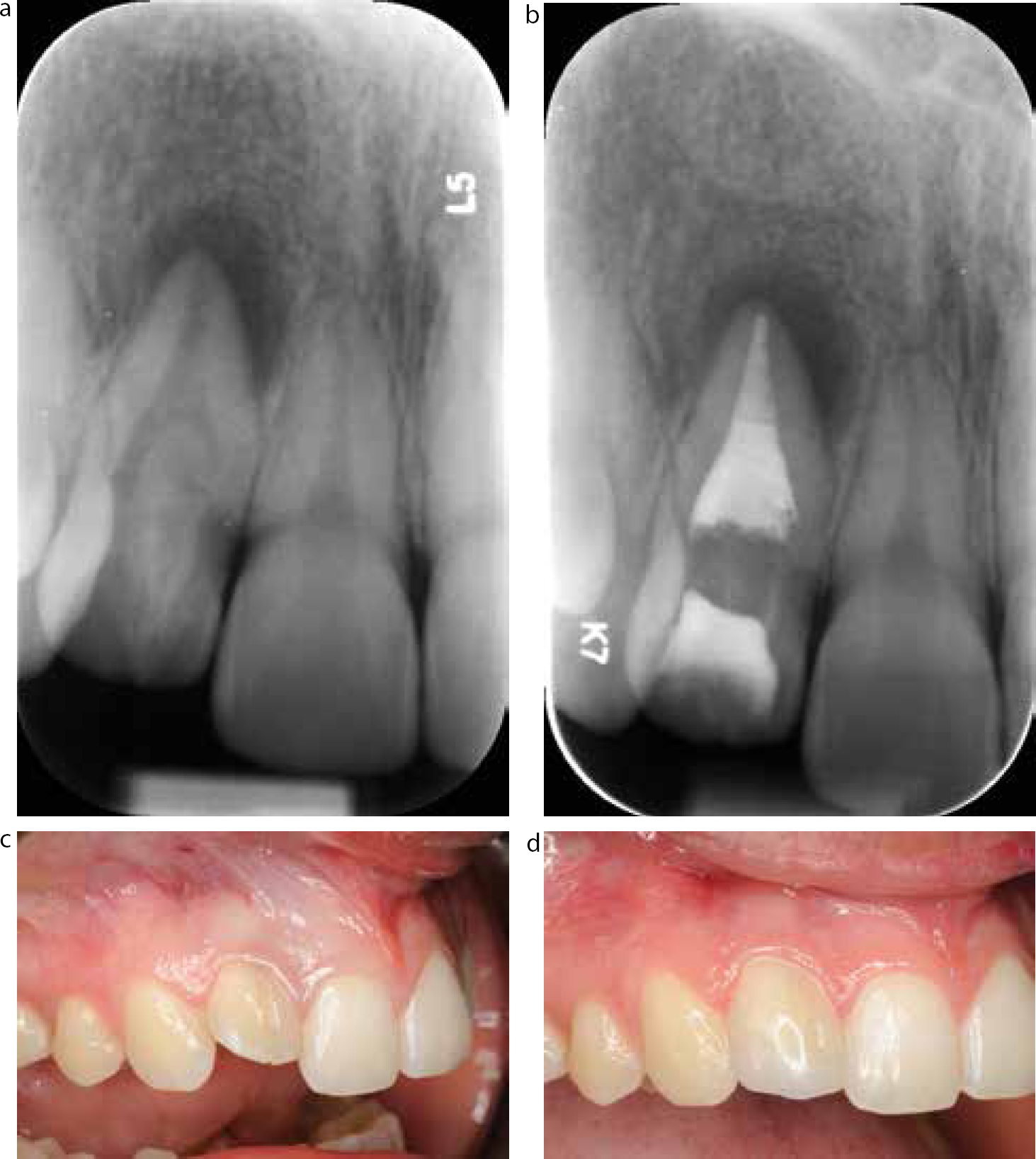
Figure 6 shows the management of a patient with dens invaginatus of the maxillary right lateral incisor. The patient presented with pain and swelling due to apical periodontitis secondary to pulpal necrosis. Clinically, the tooth had a deep labial grove, was proclined and was macrodont. Treatment involved disinfection of the root canal by eliminating the invagination to create a single pulp chamber. The root canal was filled with an apical plug of MTA and guttapercha. Following non-vital bleaching, the tooth was camouflaged with a combination of enameloplasty and direct composite placement.
Figure 6. (a–d) Radiographs and clinical views of dens invaginatus following root canal treatment and restorative camouflage.
Veneers are generally less invasive and require less preparation than crowns, but teeth affected with dens invaginatus are associated with an increased risk of developing pulpal pathology. They often have enlarged pulp chambers that can be easily exposed during conventional veneer preparation, particularly if the tooth is rotated. Veneers should only really be considered when there is minimal or no preparation required or the tooth has had successful endodontic treatment carried out. Veneers are particularly useful in teeth that have abnormal tooth shape and size. Composite and porcelain veneers have been used to camouflage 'double teeth'.80 They have also been used to restore/close the space of 'double teeth' that have been sectioned.81,82
Novel techniques using double veneers have been described to make a double tooth appear as two separate units.83Figure 7 shows a case report previously published in Dental Update that shows the use of ‘double veneers’ to camouflage ‘double teeth’.83
Figure 7.
(a, b) Indirect composite veneers used to disguise two macrodont central incisors.
Crowns
The teeth affected by dens invaginatus that are not endodontically treated are at a high risk of developing pulpal pathology.63 Preparation of vital teeth therefore carry a high risk of pulp death. Crowns should only be considered when there is minimal or no preparation required or the tooth has had successful endodontic treatment carried out.
Crowns are particularly useful in teeth that have abnormal tooth shape and size.
In 'double teeth', it has been suggested post-endodontic and sectioning of the tooth, that a crown may be a consideration in restoring teeth that have been fused.84
Metal-ceramic85 and all-ceramic crowns86 have been used to restore affected anterior teeth.
Removable prosthesis
Dentures can be used to replace dens-in dente teeth that have been extracted or used as overdenture abutments, if applicable. Dentures that are used around dens invaginated teeth, which are vital, should be designed, where possible, to provide clearance around them so that there is a reduced risk of harbouring bacteria that can contaminate or cause dental caries and potential sequelae of pulpal pathology. The changes within the invagination increase the risk of bacterial contamination and therefore increase the risk of developing pulpal pathosis.57
Implants
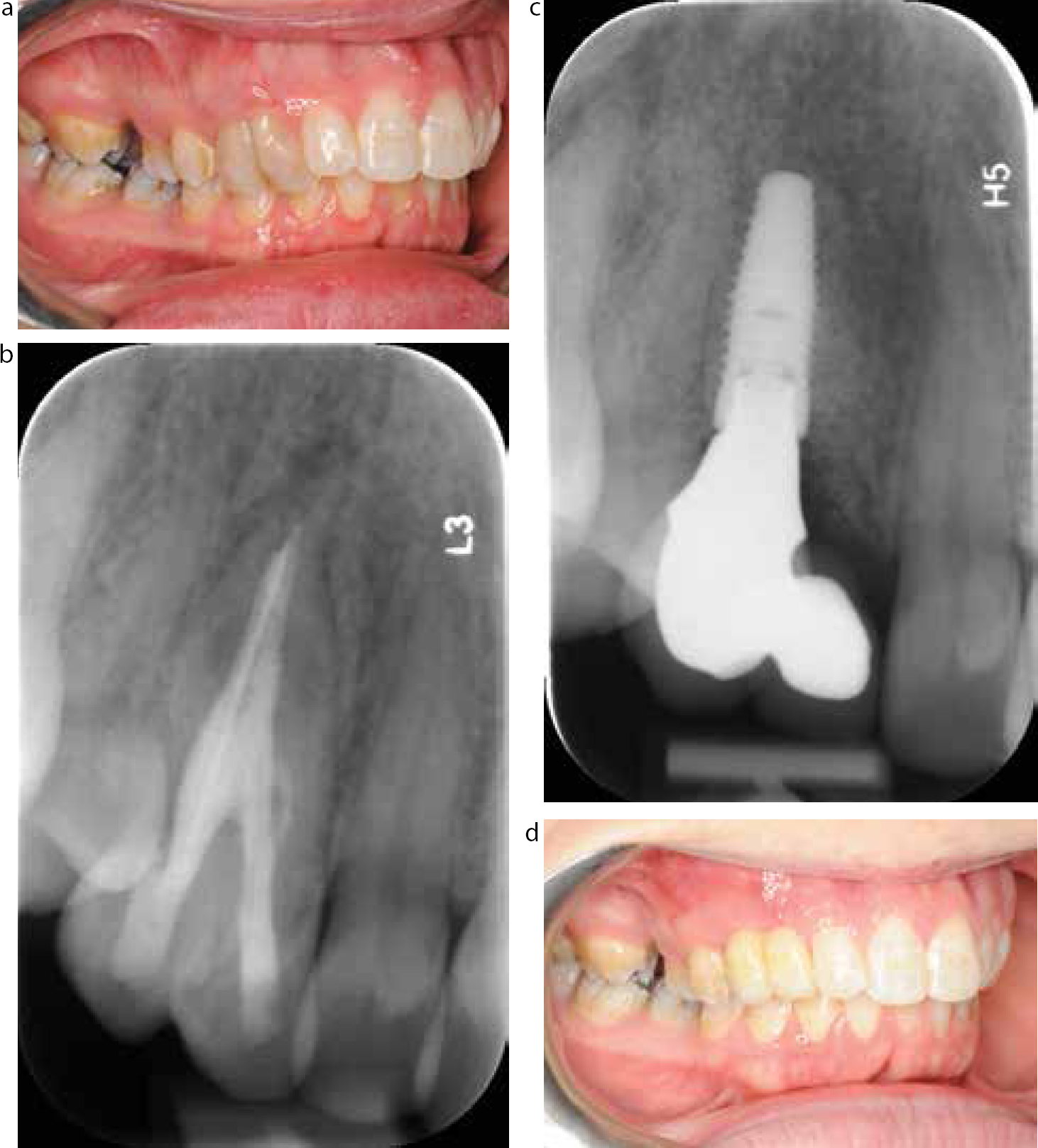
There appears to be no contra-indication in using implants to replace teeth that have had dens invaginatus or 'double teeth' or in patients with teeth affected by these conditions. The main issue arises from the mesio-distal space left behind following extraction of a wide double tooth. It may be that orthodontic treatment is required to optimize spacing as part of a comprehensive treatment strategy prior to dental implants. Therefore, careful planning is required in these malocclusion cases.78,79 With careful surgical, restorative and technical work it is often possible to improve the appearance of such cases. Figure 8 shows a patient with a double tooth in the position of the canine that had been inadequately root treated. Revision of the root treatment failed to control the infection and therefore the tooth was extracted and the spaces restored with an implant-supported cantilever bridge.
Figure 8.
(a–d) Radiographs and clinical views showing the replacement of a double tooth with an implant-supported prosthesis.
Conclusion
This article has briefly summarized the clinical presentation and restorative challenges associated with conditions affecting tooth structure, shape and size. Some conditions affect all the teeth, such as DI and AI, and others may affect one or two teeth, such as dens invaginatus and 'double teeth'. A knowledge of the challenges these conditions pose will enable all dentists to manage the functional and aesthetic problems better, with a combination of simple and more advanced restorative techniques.