Siddique I, Mahmood H, Mohammed-Ali R. Paracetamol overdose secondary to dental pain: a case series. Br Dent J. 2015; 219:E6-E6
Vogel J, Heard KJ, Carlson C, Lange C, Mitchell G. Dental pain as a risk factor for accidental acetaminophen overdose: case-control study. Am J Emerg Med. 2011; 29:1125-1129
Gilbertson RJ, Harris E, Pandey SK, Kelly P, Myers W. Paracetamol use, availability, and knowledge of toxicity among British and American adolescents. Arch Dis Child. 1996; 75:194-198
O'Sullivan LM, Ahmed N, Sidebottom AJ. Dental pain management – a cause of significant morbidity due to paracetamol overdose. Br Dent J. 2018; 224:623-626
Levy B, Paulozzi L, Mack KA, Jones CM. Trends in opioid analgesic–prescribing rates by specialty, U.S., 2007–2012. Am J Prev Med. 2015; 49:409-413
Leader R, Hackett J, Al-Naher A. Supra-therapeutic oral paracetamol overdose in adults: an update for the dental team. Dent Update. 2017; 44:409-414
Nayyer NV, Byers J, Marney C. Identify adults at risk of paracetamol toxicity in the acute dental setting: development of a clinical algorithim. Br Dent J. 2014; 216:229-235
Oscier CD, Milner QJW. Peri-operative use of Paracetamol. Anaesthesia. 2009; 64:65-72
Craig DGN, Bates CM, Davidson JS, Martin KG, Hayes PC, Simpson KJ. Overdose pattern and outcome in paracetammol-induced acute severe hepatotoxicity. Br J Clin Pharmacol. 2011; 71:273-282
Chiew AL, Isbister GK, Duffell SB, Buckley NA. Evidence for the changing regimens of acetylcysteine. Br J Clin Pharmacol. 2016; 81:471-481
Becker DE. Pain management. Part 1: Managing acute and postoperative dental pain. Anesth Prog. 2010; 57:67-79
Moore PA, Ziegler KM, Lipman RD, Aminoshariae A, Carrasco-Labra A, Mariotti A. Benefits and harms associated with analgesic medications used in the management of acute dental pain: an overview of systematic reviews. J Am Dent. 2018; 149:256-265
Denisco RC, Kenna GA, O'Neil MG, Kulich RJ, Moore PA, Kane WT Prevention of prescription opioid abuse: the role of the dentist. J Am Dent Assoc. 2011; 142:800-810
Boyer EW. Management of opioid analgesic overdose. N Engl J Med. 2012; 367:146-155
Malamed SF., 6th edn. St Louis: The CV Mosby Co; 2012
Tobias JD, Leder M. Procedural sedation: a review of sedative agents, monitoring, and management of complications. Saudi J Anaesth. 2011; 5:395-410
Jann M, Kennedy WK, Lopez G. Benzodiazepines: a major component in unintentional prescription drug overdoses with opioid analgesics. J Pharm Pract. 2014; 27:5-16
Kumar PJ, Clark ML., 8th edn. Edinburgh: Saunders; 2012
The Recognition and Management of Patients who Overdose on Analgesics Secondary to Dental Pain Joshua Lopez Mark Greenwood Dental Update 2024 47:5, 707-709.
Authors
JoshuaLopez
BDS, MFDS
DCT Oral and Maxillofacial Surgery, Royal Hallamshire Hospital, Glossop Road, Sheffield, S10 2JF
Paracetamol, Ibuprofen and Codeine are all analgesics that patients in dental pain often use in an attempt to manage their symptoms. Consequently, cases of analgesic overdose may present to dental practitioners. It is vital that clinicians are able to identify these cases and assess if transfer to an emergency department is required for assessment, investigations and any necessary treatment. Failing to do so could lead to potentially fatal consequences, and the transfer of patients to the emergency department when not warranted results in a delay in dental treatment for patients, with an added strain on emergency department resources.
CPD/Clinical Relevance: It has been reported that patients are more likely to overdose unintentionally on analgesics secondary to dental pain more than for any other reason, highlighting the importance of recognizing such cases.
Article
Joshua Lopez
Pain of dental origin is one of the leading risk factors for unintentional analgesic overdose requiring hospital admission. One study showed that, over a 2-year period, 41% of admissions for unintentional paracetamol overdose at one hospital were secondary to dental pain.1 Furthermore, a case-control study showed that accidental overdoses of paracetamol are more likely due to dental pain than for any other reason.2 There have been several hypotheses suggesting reasons why dental pain elicits analgesic overdose, such as patients having a poor understanding of analgesic regimens and maximum doses.3 The provision of dental services and the difficulty some patients have accessing dental care cannot be overlooked as a potential factor.1 One study showed that 55% of patients presenting to an emergency department with accidental paracetamol overdose due to dental pain had contacted their dentist prior to presentation, and 14% had contacted the NHS emergency and urgent care services telephone number or the local emergency dental service.4
Cases of analgesic overdose in response to dental pain are not restricted to presentation at an emergency department. A study at a dental clinic showed that 16% of patients taking analgesics prior to their visit to manage symptoms had taken supra-therapeutic doses, highlighting how clinicians must remain vigilant to ensure that they recognize cases of analgesic overdose.5 Dentists are responsible for many prescriptions of analgesia, with over 80,000 prescriptions of analgesia issued in the UK in primary care dentistry between April 2017 and April 2018.6 In the USA in 2012, dentistry accounted for 6.4% of all opioid analgesic prescriptions; which was more than that of ‘pain’ medicine and ‘emergency’ medicine.7 The role clinicians have in preventing analgesia overdose by ensuring appropriate prescriptions and advice cannot be overestimated. This article provides a summary on the recognition, treatment and dental implications of analgesic overdose in patients for three analgesics commonly used to manage dental pain: Paracetamol, Ibuprofen and Codeine.
Identification of analgesic overdose
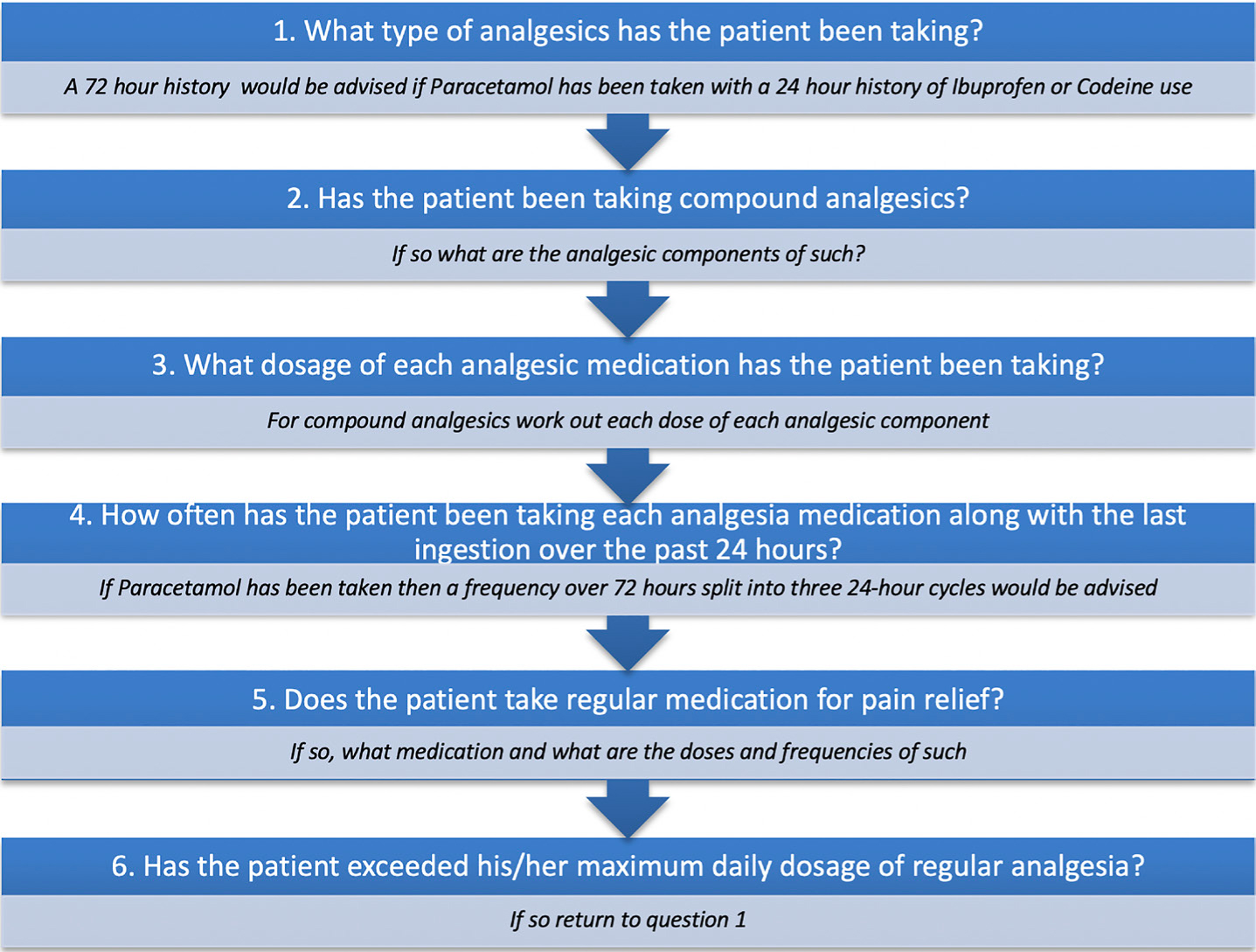
Eliciting a detailed analgesic history is the first step in recognizing an overdose. Figure 1 gives a checklist of information for clinicians to gain from patients to aid when taking a history of analgesic use. Heightened suspicion of overdose should be considered in those patients taking compound analgesics with other analgesics, as patients often do not realize that they may be exceeding maximum doses when doing so. Table 1 lists examples of various compound analgesics that are available over the counter. For some analgesics, risk factor considerations are no longer a requisite in the need for treatment, however, the authors would advise that clinicians are aware of factors that may predispose patients to more severe cases of overdose.
Figure 1. Information checklist to when taking an analgesic history.
Brand Name
Analgesic Constituent and Dosage
Analgesic Constituent and Dosage
Alka Seltzer® XS Pain Relief
Paracetamol 133 mg/tablet
Aspirin 267 mg/tablet
Anadin® Extra
Paracetamol 200 mg/tablet
Aspirin 300 mg/tablet
Co-Drydamol®
Paracetamol 500 mg/tablet
Dihydrocodeine 10 mg/tablet
Lloyds Pharmacy® Co-Codamol
Paracetamol 500 mg/tablet
Codeine Phosphate 8 mg/tablet
Nurofen® Plus
Ibuprofen 200 mg/tablet
Codeine Phosphate 12.8 mg/tablet
Nuromol®
Paracetamol 500 mg/tablet
Ibuprofen 200 mg/tablet
Paramol®
Paracetamol 500 mg/tablet
Dihydrocodeine 7.46 mg/tablet
Solpadeine® Max
Paracetamol 500 mg/tablet
Codeine Phosphate 12.8 mg/tablet
Solpadeine® Plus
Paracetamol 500 mg/tablet
Codeine Phosphate 8 mg/tablet
Syndol®
Paracetamol 450 mg/tablet
Codeine Phosphate 10 mg/tablet
Syndol® Headache Relief
Paracetamol 500 mg/tablet
Codeine Phosphate 8 mg/tablet
This list is not exhaustive and gives examples of common compound analgesics available over the counter. Please consult the British National Formulary for information in cases of uncertainty with regards to compound analgesics content.
Paracetamol
Paracetamol is indicated for use in treating dental pain and its effects are synergized when used along with Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) and opiates.8,9 The mode of analgesia of Paracetamol is through acting upon the peripheral and central nervous system, with the majority of the analgesic effect occurring on the latter.10 The exact specifics of Paracetamol's mechanism of action still remains unknown. It is stipulated that the analgesic effect is due to it acting upon the inhibitory serotonergic descending neuronal pathway, cannabinoid receptors, spinal nitric oxide production, central opioid receptors and by providing central cyclo-oxygenase (COX) inhibition to both isoforms.8,10,11 Paracetamol does not have anti-inflammatory properties like NSAIDs, even though a similar interaction inhibiting prostaglandin production has been noted which is thought to produce mild antipyretic effects.8,10
The recommended maximum therapeutic dose for a standard adult is 4g of Paracetamol a day.9 The Royal College of Emergency Medicine (RCEM) and British National Formulary (BNF) state that a potentially hepatotoxic dose of Paracetamol, the management of which requires the input of a medical colleague, is when equal to or more than 75 mg of Paracetamol per kg of body weight (75 mg/kg) has been ingested in a 24-hour period.9,12 If more than 150 mg/kg of Paracetamol is ingested, then treatment of the overdose will be required. If the patient weighs more than 110 kg, then 110 kg should be inputted for the patient's weight. Pregnant patients should have their weight pre-pregnancy used in calculations.9,12
At therapeutic doses, Paracetamol is mainly metabolized in the liver by conjugation with glucuronic acid and by sulphonation to inactive metabolites, which are then excreted in the kidneys. A small fraction of Paracetamol is metabolized by oxidation via the enzyme cytochrome P450 pathway, producing a reactive metabolite N-acetyl-p-benzoquinoneimine (NAPQI).8,10 This reactive metabolite at therapeutic doses binds to sulphydryl groups, which can be provided by glutathione and does not cause harm. Hepatotoxicity occurs when NAPQI production outweighs the availability of glutathione. The excess NAPQI binds to liver cellular proteins, causing cell injury and precipitating an inflammatory response, followed by hepatocellular necrosis and giving rise to liver damage.11
Risk factors for hepatotoxicity due to Paracetamol overdose are any factors that deplete glutathione levels or contribute to hepatic enzyme induction, and these are outlined in Table 2.11 Hepatotoxicity is the main result of Paracetamol overdose, but Nephrotoxicity may also occur. Unintentional Paracetamol overdoses have been documented to show a higher rate of mortality, and it is these cases that will be predominantly presenting in the dental setting.13 Within the first 24 hours of an ingestion of a hepatotoxic dose, patients are often asymptomatic and any symptoms are often non-specific, such as nausea, abdominal pain and vomiting. Pain in the upper right quadrant of the abdomen is indicative of established liver damage. A reduction in the apparent level of consciousness could indicate a massive ingestion potentially coupled with another medication overdose. Signs of liver damage may then be seen from 24 hours after a hepatotoxic dose, such as: hepatic tenderness, jaundice and impaired consciousness.11 The clinician should be aware that symptoms may not arise until 2–3 days post-hepatotoxic ingestion.
▪ Malnourishment
▪ Eating disorders (anorexia/bulimia)
▪ Alcoholism
▪ Liver disease, eg Hepatitis C, Liver cirrhosis
▪ Cystic fibrosis
▪ Cachexia
▪ HIV
▪ Long-term treatment with enzyme-inducing drugs, eg Carbamazepine, Phenobarbital, Phenytoin, Primidone, Rifampicin, Rifabutin, Efavirenz, Nevirapine and St John's wort
Management of suspected Paracetamol overdose by the emergency department
If indicated, treatment is via an intravenous infusion of acetylcysteine.11 Acetylcysteine is hydrolysed intracellularly to cysteine which replenishes gluthathione stores that bind to NAPQI and prevent this active metabolite from causing hepatocellular necrosis. Acetylcysteine can also aid thiol groups to bind directly to NAPQI in hepatocytes to prevent cellular damage.14 Delayed treatment of Paracetamol overdose can result in liver failure, with the patient possibly requiring a liver transplant as the only way to prevent death.11
Ibuprofen
Ibuprofen is a NSAID used to treat dental pain due to its anti-inflammatory, antipyretic and analgesic properties.15 Ibuprofen's mechanism of action is through its reversible inhibition of Cyclo-oxygenase enzymes (COX-1 and COX-2), resulting in reduced synthesis of arachidonic acid and therefore that of prostaglandin and thromboxane A2 (TXA2). Ibuprofen's analgesic properties are due to the reduction in prostaglandin that acts on the hypothalamus to produce fever and regulates inflammatory mediators involved in the sensitization of pain fibres. It is a weak acid that is metabolized mainly in the liver via oxidation and conjugation.16
Ibuprofen toxicity occurs predominantly due to a decrease in prostaglandin synthesis (via COX-1 inhibition) and the resulting effects this has on the gastrointestinal, renal and central nervous system (CNS). Toxicity may also occur due to the accumulation of acidic metabolites, resulting in biochemical imbalances.16 Nephrotoxicity is a rare complication and neurological toxicity symptoms range from drowsiness to convulsions and coma in catastrophic overdoses.16 There is a small risk of cardiovascular collapse in patients with pre-existing cardiovascular disease such as; ischaemic heart disease, peripheral arterial disease, cerebrovascular disease, congestive heart failure and uncontrolled hypertension when supra-therapeutic doses of Ibuprofen are ingested due to COX-2 inhibition.9 Exacerbation of asthma can occur with severe Ibuprofen overdoses.17
Ibuprofen toxicity is rare due to its large therapeutic window and, even with clinically significant overdoses, patients often only develop self-limiting symptoms such as nausea, vomiting, epigastric pain or, more rarely, diarrhoea. In cases of severe overdose, symptoms such as GI bleeding, tinnitus, headache, convulsions and coma occur. In standard preparations, symptoms will be seen within four hours and, in sustained release preparations, this can be doubled.16 The BNF states that 2.4 g of Ibuprofen a day is the maximum therapeutic dose.9 In the literature it is stated how patients predominantly remain asymptomatic when ingestion of Ibuprofen is less than 100 mg/kg (within 24 hours), with doses of more than 400 mg/kg associated with significant toxicity.16,17 The National Poisoning Information Service (NPIS) gives guidance on how any patient presenting having ingested more than 100 mg/kg (within 24 hours), or less than this, but are symptomatic, should be referred for medical assessment.17
Management of suspected Ibuprofen overdose by the emergency department
Activated charcoal can be administered to reduce Ibuprofen absorption if it is within one hour of last ingestion. Asymptomatic patients are assessed for four hours after last ingestion when taking standard preparations, and for eight hours with sustained release preparations. When patients are symptomatic, they are treated upon the signs of toxicity that they show, as some patients may have symptoms that require no treatment if they have only mild epigastric pain and those with convulsions or metabolic acidosis will be treated accordingly.18
Codeine
Codeine is an opioid analgesic used for the management of mild to moderate pain.12 Codeine is available without prescription in the UK in compound analgesics, with single preparations in the form of codeine phosphate only available with a prescription. Opioid analgesics are not indicated in the treatment of acute dental pain or peri-surgical pain.19 The combination of Paracetamol and a NSAID (if not contra-indicated) should be the first line analgesics used to manage dental pain.12,19 Opioid analgesics have greater adverse side-effects and their use can lead to addiction and subsequent misuse. This is shown in the current American opioid epidemic where it has been reported that approximately 130 people in the USA die daily due to opioid overdose and, in 2017, it was estimated that 1.7 million people in the USA suffered from opioid substance misuse disorders.20 Dentists are the second largest prescriber of immediate release opioids in the USA, accounting for 12% of all prescriptions, and it is these opioids that are frequently abused.21 This shows the role dentists play in this epidemic and inversely the role dentists can play to protect patients from opioid misuse and overdose through appropriate prescribing.
The mechanism of action of opioid analgesics is via acting as agonists to opioid receptors in the CNS. Codeine has minimal affinity for opioid receptors and its analgesic properties are primarily gained through its metabolism in the liver by the cytochrome P450 CYP2D6, where 10% transforms to morphine. It is the active metabolite morphine that acts as an agonist on predominantly mu-opioid receptors, producing its analgesic and potentially adverse affects.15,18 The ability of an individual to metabolize Codeine to morphine directly relates to its analgesic and adverse potential. Excretion of Codeine and its metabolites are via the kidneys and any kidney function impairment greatly increases the risk of toxicity due to reduction of elimination of morphine.17,18 Opioid receptor stimulation results in depression of the respiratory and central nervous systems. Toxicity occurs when this effect is so great that it results in deep coma, convulsions, respiratory depression and can ultimately prove fatal. These effects of overdose are potentiated with the ingestion of alcohol or other centrally acting drugs.17
The BNF states how the maximum dose of codeine is 240 mg a day. Guidance is given by Toxbase® that states if a patient has ingested an estimated toxic dose of 2.5 mg per kg of body weight or more in 24 hours he/she should be referred for medical assessment.9,17 All patients who have intentionally overdosed on this analgesic and those that are symptomatic, regardless of dose ingested, should be transferred to an emergency department.17
Management of suspected Codeine overdose by the emergency department
Diagnosis of opioid overdose is made predominantly by clinical signs and symptoms, such as a reduced respiratory rate, nausea, vomiting, hallucinations and constriction of the pupils. A decrease in oxygen saturation to levels of less than 90% can result in pulmonary oedema and further complications. If the patients present within an hour of ingestion, then activated charcoal can decrease absorption. Treatment of opioid overdose is via the administration of Naloxone that has the ability to reverse all signs of opioid toxicity due to its action as a competitive mu-opioid receptor antagonist.22
Dental implications of analgesic overdose
Dental treatment should be delayed until the patient has had the analgesic overdose treated. Primary metabolism of amide local anaesthetics, such as Lidocaine, Mepivacaine, Prilocaine and Bupivacaine occurs in the liver. Articaine has both ester and amide links and is therefore partially metabolized in the liver and blood plasma and Prilocaine is also partly metabolized in the lungs.23 A reduction in the rate of metabolism of these local anaesthetics will be seen in impaired liver function, which occurs with Paracetamol, Ibuprofen and Codeine toxicity. Therefore, there is an increased risk of local anaesthetic toxicity in cases of analgesic overdose.
Analgesic overdoses impact upon the provision of conscious sedation and general anaesthesia. Sedative agents, such as Benzodiazepines, used in conscious intravenous sedation and Propofol, used for general anaesthesia, work through depression of the respiratory and CNS to different extents.24 This inhibition of the respiratory system and CNS is accentuated in cases of analgesic overdose, for example the combination of Midazolam and Codeine results in significant respiratory depression.25 Many sedative agents, such as Midazolam and Propofol, are metabolized in the liver and, in cases of analgesic overdoses that result in hepatotoxicity, this would result in a reduction of the metabolism of these sedative agents, increasing both their therapeutic and potentially toxic effects.24
There is an increased bleeding risk in surgical procedures, such as exodontia in patients who have taken analgesics at a toxic dose. Ibuprofen's anti-platelet effect via Cox-1 inhibition results in a reduction of TXA2, increasing a patient's bleeding potential.16 Analgesic overdose can lead to hepatic function impairment, which reduces the liver's ability to produce the clotting factors necessary in the coagulation cascade for haemostasis.26 Consideration must be given for the necessity of local haemostatic measures, such as packing, suturing and the use of tranexamic acid, where patients have taken maximum doses of analgesia. When prescribing, clinicians need to consider the hepatotoxic effects that may occur, with the liver often being the primary site of drug metabolism for drugs prescribed in the dental formulary. Advice needs to be given to patients on future analgesic dose regimens and alternative analgesics, where necessary.
Conclusion
Analgesic overdose presentation in a dental setting needs to be recognized due to its potentially fatal consequences and the impact that it can have on providing dental treatment and prescribing. It should be noted that not every clinical situation has been covered in this paper and that, for complex cases such as pregnant or paediatric patients, clinicians should contact the appropriate on call medical colleague for advice or seek advice from the resources mentioned. The authors would advise that contact (or direct transfer in impending emergency situations) should be made to the local emergency department when urgent transfer for assessment is required or advice required in cases of analgesic overdose. All cases of deliberate analgesic overdose must be transferred immediately to the local emergency department.