Kumar S, Gupta A, Dixit A, Balasubramanyam G, Prabu D, Kulkarni S. Factors that affect dental caries status of medical students in Udaipur city, India. Int J Dent Hyg. 2010; 82:110-115
Rashad JM. Dental knowledge and behavior among technical medical institute students in Baghdad governorate. J Bagh College Dentistry. 2012; 24:115-119
Al-Omari WM, Al-Omiri MK. Dental anxiety among university students and its correlation with their field of study. J Appl Oral Sci. 2009; 17:199-203
Hakim H, Razak IA. Dental fear among medical and dental undergraduates. Scientific World J. 2014; 747508:1-5
Locker D, Shapiro D, Liddell A. Negative dental experiences and their relationship to dental anxiety. Community Dent Health. 1996; 13:86-92
, 3rd edn. : Public Health England; 2014
Baysan A, Lynch E. Management of primary root caries with a high fluoride dentifrice.London: Quintessence; 2001
Ekstrand KR. High fluoride dentifrices for elderly and vulnerable adults: does it work and if so, then why?. Caries Res. 2016; 50:15-21
Näsman P, Ekstrand J, Granath F, Ekbom A, Fored CM. Estimated drinking water fluoride exposure and risk of hip fracture: a cohort study. J Dent Res. 2013; 92:1029-1034
Usman S, Bhat SS, Sargod SS. Oral health knowledge and behaviour of clinical medical, dental and paramedical students in Mangalore. J Oral Health Com Dent (JOHCD). 2007; 13:46-48
Sharda AJ, Shetty S. A comparative study of oral health knowledge, attitude and behaviour of non-medical, para-medical and medical students in Udaipur city, Rajasthan, India. Int J Dent Hyg. 2010; 8:101-109
McCann PJ, Sweeney MP, Gibson J, Bagg J. Training in oral disease, diagnosis and treatment for medical students and doctors in the United Kingdom. Br J Oral Maxillofac Surg. 2005; 43:61-64
Mouradian WE, Reeves A, Kim S, Evans R, Schaad D, Marshall SG, Slayton R. An oral health curriculum for medical students at the University of Washington. Acad Med. 2005; 80:434-442
’Educating the educated’: a report of an undergraduate medical student with multiple carious lesions and poor dietary habits Amardeep Singh Dhadwal Aylin Baysa Dental Update 2024 44:6, 707-709.
Authors
Amardeep SinghDhadwal
Final Year BDS Undergraduate Student, The Institute of Dentistry, Barts and the London School of Medicine and Dentistry, Queen Mary University, London, E1 2AT, UK
Senior Clinical Lecturer, Department of Adult Oral Health, The Institute of Dentistry, Barts and the London School of Medicine and Dentistry, Queen Mary University, London, E1 2AT, UK
It is evident in the undergraduate dental curriculum that competent dental students are expected to have a broad knowledge of the intricacies of the human body and its relationship with the oral cavity, but the same cannot be guaranteed for medical students. This case report of a medical undergraduate student who presented with multiple carious lesions and a poor knowledge of the impact of her habits on her oral heath illustrates the importance of using a well-formulated and holistic treatment plan with a focus on oral health promotion and education. The review appointment proved promising with an improved plaque score and dietary analysis. This article provides a brief introduction to the topics and discusses potential future developments that aim to reduce the subjectivity in the analysis process and simplify presentation of evidence to non-dental parties.
CPD/Clinical Relevance: This case re-iterates the need to encompass education and prevention to stabilize and prevent dental caries and teach other future healthcare professionals so that they can utilize and consider this knowledge in the management of their own patients. Moreover, it demonstrates that there may be scope for raising dental awareness and education within the medical profession.
Article
Although dental practitioners possess a detailed knowledge of the management and multifactorial aetiology of dental caries, treatment remains predominantly operative, failing to address the long-term consequences and the likelihood of new carious lesions, further progression of existing early carious lesions and caries adjacent to restorations. It may be suggested that this is due to the time constraints dental professionals may face in trying to stabilize and restore carious lesions, whilst also providing the thorough education and preventive advice needed to aid patients with the necessary knowledge of how their behaviour can impact their oral health.
Due to their intellectual ability and general understanding of the human body, it may be incorrectly assumed that medical students are aware of the importance of good dietary habits and oral health education in reducing the risk of dental diseases in themselves and their patients. Consequently, this may also lead to a reduction in the time and effort invested in educating them about their habits. Recent literature suggests that this may not be the case. For example, in a cohort of undergraduate medical students in India, dental caries status was significantly affected by factors such as high dental anxiety and poor plaque control.1 Kumar et al identified that 75.7% of these students brushed their teeth once daily.1 A similar study identified that only 35.5% of medical students who participated were aware that they can reduce their susceptibility to dental caries through regular brushing and dental attendance, reduced sugar consumption and using fluoride.2 The patient in this report stated that the aetiology and management of dental diseases have not yet been implemented into the undergraduate curriculum.
The aim of this clinical case report of a medical undergraduate student, who presented with multiple carious lesions, is to demonstrate the importance of using a personalized and detailed history and examination to construct a well-formulated holistic treatment plan. It also re-iterates the need to encompass education and prevention to stabilize and prevent dental caries and to teach other future healthcare professionals so that they can also utilize and consider this knowledge in the management of their own patients. Moreover, it demonstrates that there is still scope for raising dental awareness and education within the medical profession.
Case report
A 22-year-old female attended the undergraduate restorative clinic for a general check-up at Barts and the London School of Medicine and Dentistry. Having last visited a dentist two years previously, the patient was an irregular dental attender. She admitted being anxious regarding the dental appointment.
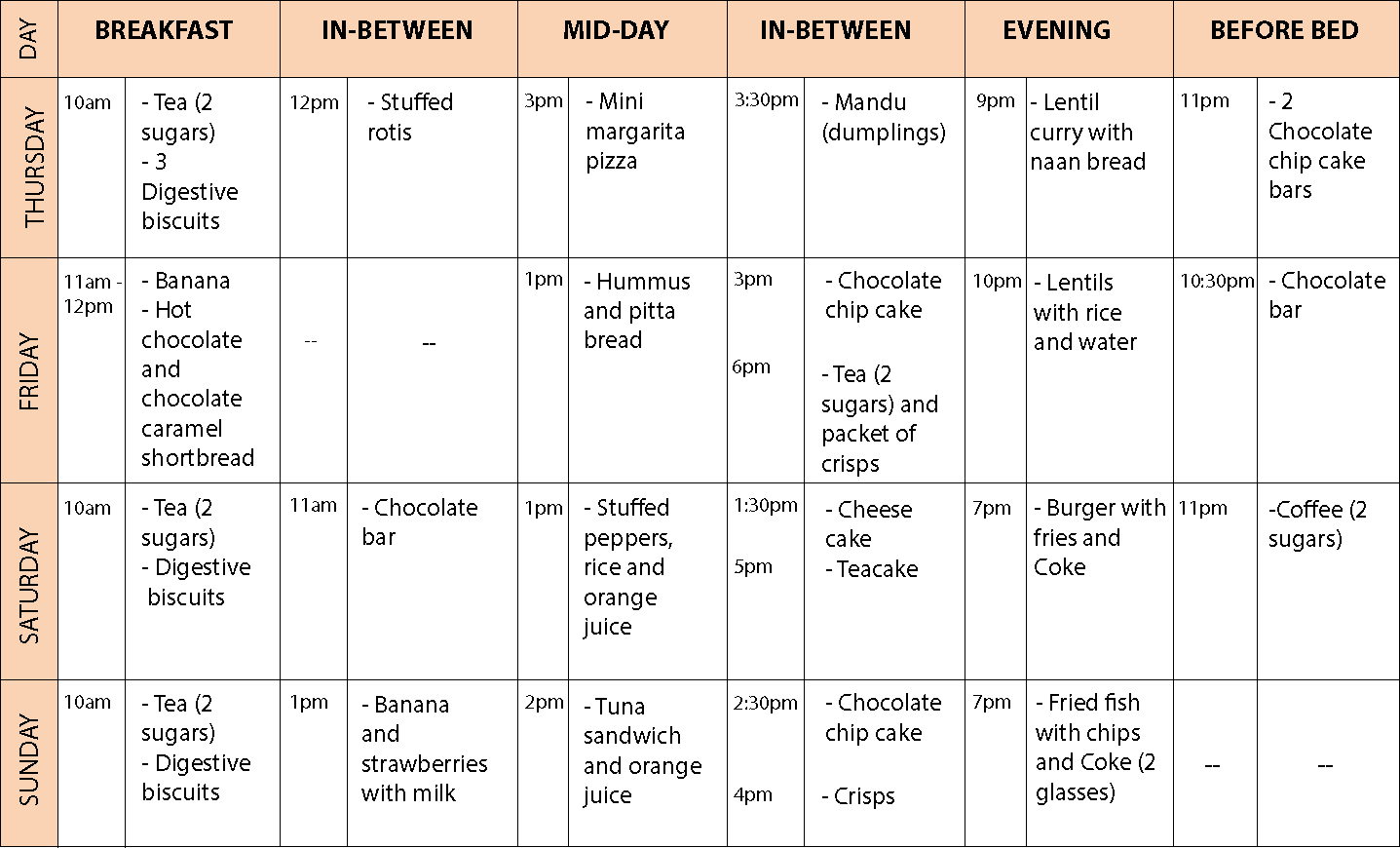
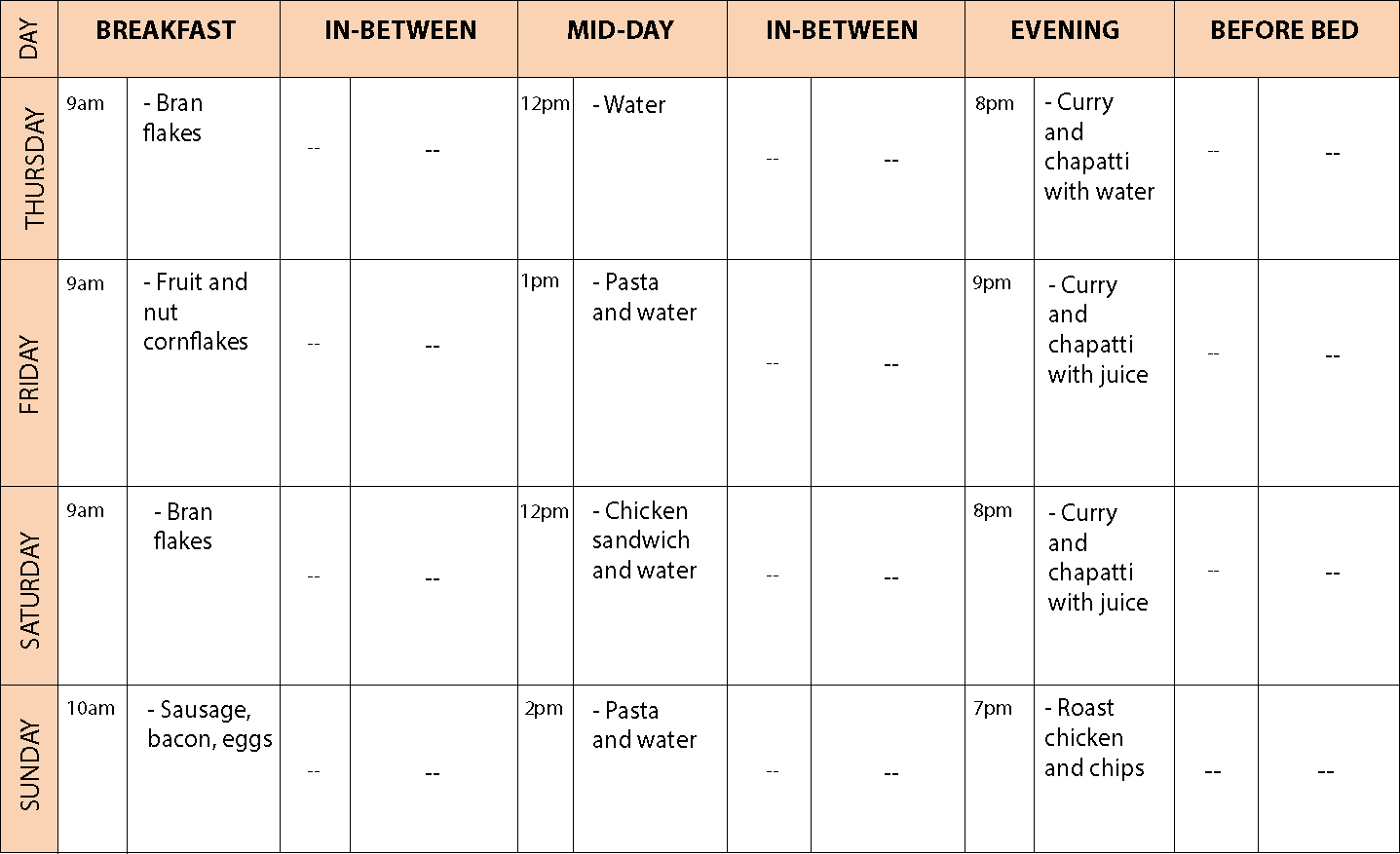
Her medical history revealed well-controlled Irritable Bowel Syndrome with no medications. There were no known allergies reported. Careful questioning concluded that her lifestyle is stressful and hectic as a medical student and she had a highly cariogenic diet with frequent sugar consumption on weekends whilst studying (Figure 1). The patient reported brushing her teeth twice daily using a standard fluoridated dentifrice with an electric toothbrush but failed to use interdental cleaning aids regularly and was unaware of the significance of fluoride usage. Before bed, whilst studying, the patient would continue to snack after brushing her teeth (Figure 1).
Figure 1. Diet analysis sheet at the beginning of treatment.
Clinical examination revealed a minimally restored dentition. Generalized marginal and interproximal plaque deposits were visible with mildly inflamed gingivae with immediate bleeding on probing in all sextants. The Basic Periodontal Examination scores were all marked as ‘2’ except a score of ‘1’ in the maxillary anterior sextant.
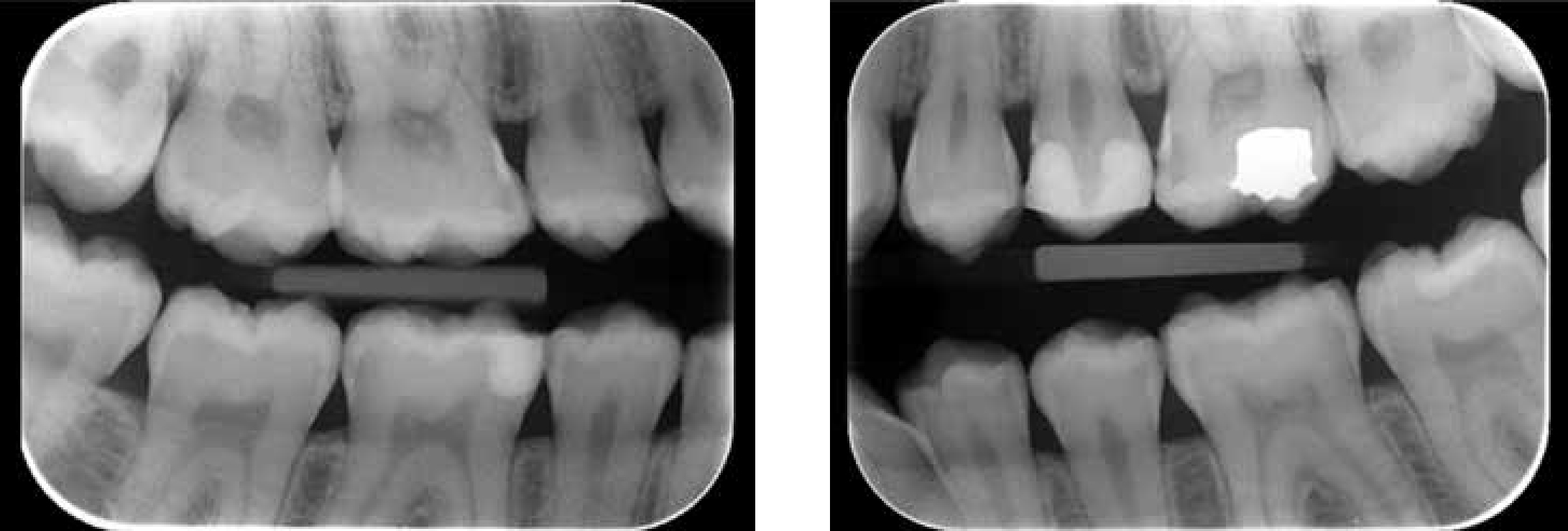
Clinically, suspected carious lesions were visible at the LL6 (distal), LL7 (mesial), LL8 (occlusal) and LR6 (distal) (Figure 2). These teeth were symptom free and the patient was surprised at the findings. Additionally, bitewing radiographs (Figure 3) revealed further radiolucencies consistent with caries:
Figure 2. Clinical examination revealed generalized stained fissures posteriorly, enamel caries at the LL67 and dental caries at the LL8 and LR6.Figure 3. Left and right bitewings taken at initial screening appointment.
The treatment plan for this patient was divided into three main stages to ensure that a holistic approach to treatment planning was adopted and to help to reduce the patient's high caries risk and dental anxiety.
Investigation, stabilization and prevention phase:
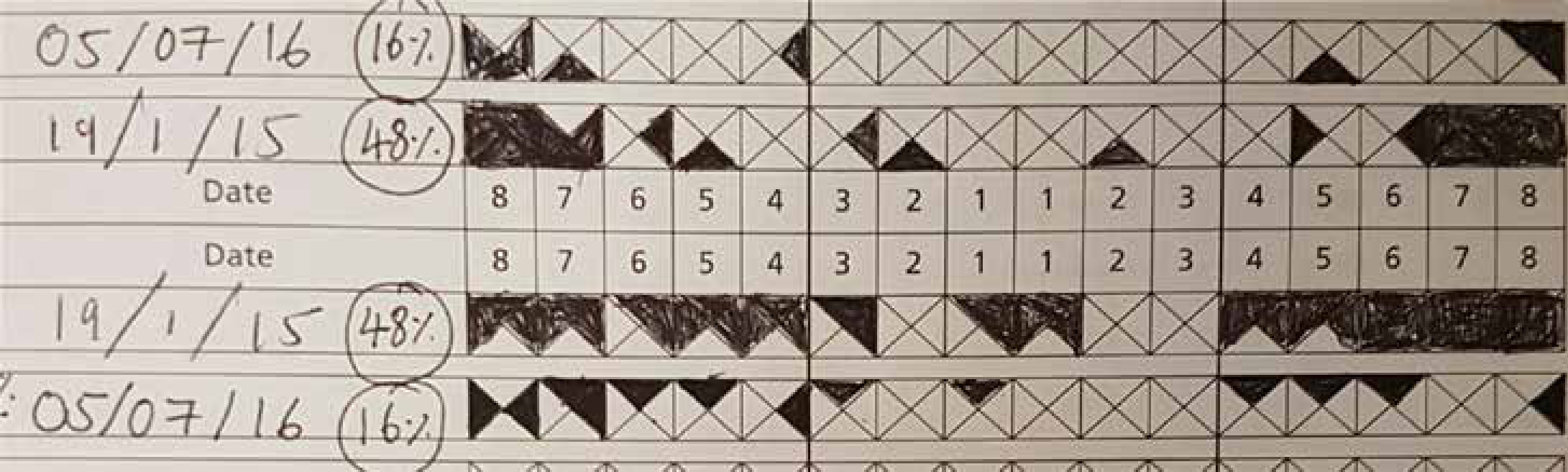
Baseline assessments: plaque distribution chart (47.7%) (Figure 4) and bleeding points index (11%) – also used to aid education and provide sufficient oral hygiene instructions to the patient;
Diet analysis and education: using a diet sheet to explain the link between her dietary habits and dental caries and to identify contributing factors and assess the frequency of sugar intake;
Oral hygiene instructions using interdental cleaning aids and a demonstration of the appropriate brushing technique;
Full mouth supragingival debridement and polish.
Restorative and rehabilitation phase:
Direct restoration of teeth with dental caries into dentine.
Maintenance and monitoring phase:
Monitor dentition and teeth with early carious lesions: apply fluoride varnish (2.2% sodium fluoride), repeat at least twice yearly and consider prescribing a high fluoride toothpaste;
Regular maintenance through review appointments to ensure that plaque control and diet are improving and no new carious lesions develop and monitor progression of lesions confined to enamel.
Figure 4. Plaque index at initial screening appointment and at post-treatment review appointment.
Subsequent appointments demonstrated that this systematic and methodical approach to treatment planning equipped the patient with the necessary knowledge and motivation to help stabilize and improve her oral health. As the patient was considered to be high caries risk, a reduced recall interval of 3 months, following the initial phase of treatment, was most appropriate. The review appointment identified that no new carious lesions developed and the patient had retained information and education provided previously, adopted a more adequate oral hygiene regimen and was more positive about the power she has to maintain and improve heroral health. Her reduction in plaque and reduced frequency of sugar consumption and snacking after brushing in the evenings proved promising (Figures 4 and 5).
Figure 5. Diet analysis sheet at review appointment.
Discussion
With such a case, detailed history-taking to identify a cariogenic diet and stressful lifestyle is the centre of the consultation. This can be used to formulate a personalized treatment plan that places an emphasis on prevention and education. Interestingly, this patient was aware of the benefits of a healthy and balanced diet and the effect of dietary carbohydrates on the human body, however, her awareness of their impact on her oral health was poor. Many students go through a transition period when they are at university. During this period, their routine lifestyle with their parents may discontinue and they may acquire a different perspective in eating habits.
It is also crucial that the dental anxiety of the patient is considered when treating and managing her oral health. Al-Omari and Al-Omiri assessed the anxiety scores for dental treatment amongst university students. The results revealed the highest dental anxiety scores for medical students and female students in all subjects when compared to the engineering and dental students.3 Kumar et al also identified that female medical students exhibited greater dental anxiety than male medical students.1 It has been suggested that, ultimately, dental anxiety may lead to irregular dental attendance within female medical students4 and that it is related to personality traits and psychological status.5 These could be the main factors for the presence of higher levels of dental anxiety amongst female medical students but may also encourage poor dietary habits.
During the university years, the harsh reality of a competitive environment, continuous assessments, and psychological challenges may lead to inadequacy and self-doubt. All these factors may then contribute to conscious or unconscious eating habits that can adversely affect oral health. Additional adverse factors could be related to working stressful hours, staying up late to study, and long days on placements.
To aid management, prior to commencing restorative treatment, oral health promotion could begin with an explanation of the well-established link between dietary sugars and dental caries. A diet diary, containing work days and leisure days, is a useful tool for doing this. It enables the identification of the frequency of sugar intake as well as quantity. Whilst evoking behaviour change is more complex than this, it is useful in building a strong therapeutic relationship with patients, as well as preventing the patient from having such frequent sugar consumption within a day. This may help to reduce dental anxiety slightly at the first visit and also the fear and anxiety related to subsequent dental treatments.
Additionally, with patients of high caries risk and active dental caries, the prescription of a high fluoride toothpaste could be considered. Current Public Health England guidelines suggest that toothpaste with a high fluoride concentration may be prescribed in patients with active disease.6 According to these guidelines, for patients aged 10 or over, toothpaste containing 2,800 ppm fluoride may be prescribed whilst, for patients aged 16 or over, either 2,800 ppm or 5,000 ppm fluoride toothpaste can be prescribed.6 Clinicians may prefer to prescribe the lower concentration of 2,800 ppm in young patients since there is currently insufficient evidence to support that toothpaste containing 5000 ppm fluoride has a superior effect to the 2,800 ppm dentifrice for the management of dental caries.7 In this respect, the adverse systemic effects of long-term exposure to a higher concentration of fluoride also remain uncertain.8,9
The lack of oral health knowledge demonstrated by the medical student was concerning. Taking time to identify patient risk factors and provide the basic knowledge in oral health could raise patient awareness. It is important that medical students and practitioners have a reasonable knowledge regarding dental caries and assessing the risk factors to improve the general health of their patients.
By joining dental practitioners at the forefront of the healthcare profession, medical practitioners are also influential and suitable for helping to reduce the global burden of dental caries by educating their patients on the impact of habits such as poor diet, and fluoride use, on their oral health. Further literature suggests that there is an unacknowledged need to identify and assimilate information regarding medical students' perceptions and knowledge of oral health.10,11 It has been suggested that one way of achieving this is through embedding oral health teaching into the undergraduate medical school curriculum.11,12,13 However, there is currently insufficient available evidence identifying the effectiveness of this approach.
Conclusion
This is an interesting case suggesting a potential lack of dental awareness within the medical profession and undergraduate medical curriculum. This emphasizes that there is a greater need to investigate the teaching and oral health perceptions of medical professionals. This case also highlights the importance of adopting a holistic approach to the history-taking process by asking questions about anxiety, stress and daily routines. There is a need to ensure that patients of all educational backgrounds are provided with adequate preventive dietary and oral hygiene advice to alleviate the demand for multiple restorative treatments at a young age and to help ensure that solidarity remains amongst healthcare professionals to maximize the chances of reducing the global burden of oral diseases.