Stecker S, Diangelis AJ. Dens evaginatus. A diagnostic and treatment challenge. J Am Dent Assoc. 2009; 133:190-193
Kocsis G, Marcsik A, Kokai E, Kocsis K. Supernumerary occlusal cusps on permanent human teeth. Acta Biol Szeged. 2002; 36:71-82
Jerome CE, Hanlon RJ. Dental anatomical anomalies in Asians and Pacific Islanders. J Calif Dent Assoc. 2007; 35:631-636
Merrill RG. Occlusal anomalous tubercles on premolars of Alaskan Eskimos and Indians. Oral Surg Oral Med Oral Pathol. 1964; 17:484-496
Hill FJ, Bellis WJ. Dens evaginatus and its management. Br Dent J. 1984; 156:400-402
Ngeow WC, Chai WL. Dens evaginatus on a wisdom tooth: a diagnostic dilemma. Case report. Aust Dent J. 1998; 43:328-330
Palmer M. Case reports of evaginated odontomes in Caucasians. Oral Surg Oral Med Oral Pathol. 1973; 35:772-779
Stewart R, Dixon G, Graber R. Dens evaginatus (tuberculated cusps): genetic and treatment considerations. Oral Surg Oral Med Oral Pathol. 1978; 46:831-836
Curzon M, Curzon J, Payton H. Evaginated odontomes in the Keewatin Eskimo. Br Dent J. 1970; 129:324-328
Thesleff I, Keranen S, Jernvall J. Enamel knots as signalling centers linking tooth morphogenesis and odontoblast differentiation. Adv Dent Res. 2001; 15:14-18
Thesleff I. Developmental biology and building a tooth. Quintessence Int. 2003; 34:613-620
Kangas AT, Evans AR, Thesleff I, Jernvall J. Nonindependence of mammalian dental characters. Nature. 2004; 432:211-214
Cobourne MT, Hardcastle Z, Sharpe PT. Sonic hedgehog regulates epithelial proliferation and cell survival in the developing tooth germ. J Dent Res. 2001; 80:1974-1979
Wang X, Aberg T, James MJ Runx2 (Cbfa1) inhibits shh signaling in the lower but not upper molars of mouse embryos and prevents the budding of putative successional teeth. J Dent Res. 2005; 84:138-143
Sedano HO, Ocampo-Acosta F, Naranjo-Corona RI. Multiple dens invaginatus, mulberry molar and conical teeth. Case report and genetic considerations. Med Oral Patol Oral Cir Bucal. 2009; 14:69-72
Echeverri EA, Wang MM, Chavaria C, Taylor DL. Multiple dens evaginatus: diagnosis, management, and complications: case report. Pediatr Dent. 1994; 16:314-317
Oehlers F, Lee K, Lee E. Dens evaginatus (evaginated odontome): its structure and responses to external stimuli. Dent Pract Dent Rec. 1967; 17:239-244
Levitan ME, Himel VT. Dens evaginatus: literature review, pathophysiology, and comprehensive treatment regimen. J Endod. 2006; 32:1-9
Rao Y, Guo L, Hu T. Multiple dens evaginatus of premolars and molars in chinese dentition: a case report and literature review. Int J Oral Sci. 2010; 2:177-180
Lau T. Odontomes of the axial core type. Br Dent J. 1995; 99:219-225
Hillson S, Grigson C, Bond S. Dental defects of congenital syphilis. Am J Phys Anthropol. 1998; 107:25-40
Nissanka-Jayasuriya EH, Odell EW, Phillips C. Dental stigmata of congenital syphilis: a historic review with present day relevance. Head Neck Pathol. 2016; 10:327-331
Summary for Policymakers.Cambridge: Cambridge University Press; 2014
Bolk L. Problems of human dentition. Am J Anat. 1916; 19:91-148
Seehra J, Coutts F. The talon cusp – an uncommon anomaly. Dent Update. 2012; 39:262-264
Cho SY, Ki Y, Chu V, Chan J. Concomitant developmental dental anomalies in Chinese children with dens evaginatus. Int J Paediatr Dent. 2006; 16:247-251
Ohishi K, Ohishi M, Takahashi A Examination of the roots of paramolar tuberoles with computed tomography: report of 3 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol. 1999; 88:479-483
Hattab FN, Yassin OM, Al-Nimri KS. Talon cusp in permanent dentition associated with other dental anomalies: review of literature and reports of seven cases. ASDC J Dent Child. 1996; 63:368-376
Turner JW, Kluemper GT, Chance K, Long LS. Dens evaginatus: the hornet's nest of adolescent orthodontics. Am J Orthod Dentofac Orthop. 2013; 143:570-573
Morinaga K, Aida N, Asai T. Dens evaginatus on occlusal surface of maxillary second molar: a case report. Bull Tokyo Dent Coll. 2010; 51:165-168
Yip W-K. The prevalence of dens evaginatus. Oral Surg Oral Med Oral Pathol. 1974; 38:80-87
Reichart P, Tantiniran D. Dens evaginatus in the Thai. Oral Surg Oral Med Oral Pathol. 1975; 39:615-621
Stecker SS, Peterson VS, Beiraghi S Dens evaginatus: just another cusp?. Northwest Dent. 2015; 94:31-33
Villa VG. Chronic periapical abscess with extraoral sinus associated with the so-called ‘Leong's premolar’. Philippines Med Dent J. 1956; 2:19-20
Allwright W.C. Odontomes of the axial core type as a cause of osteomyelitis of the mandible. Br Dent J. 1958;
Goto T, Kawahara K, Kondo T Clinical and radiographic study of dens evaginatus. Dentomaxillofac Radiol. 1979; 8:78-83
McKaig SJ, Shaw L. Dens evaginatus on the labial surface of a central incisor: a case report. Dent Update. 2001; 28:210-212
Gallacher A, Ali R, Bhakta S. Dens invaginatus: diagnosis and management strategies. Br Dent J. 2016; 221:383-387
Tyndall D, Kohltfarber H. Application of cone beam volumetric tomography in endodontics. Aust Dent J. 2012; 57:72-81
Neelakantan P, Subbarao C, Subbarao CV. Comparative evaluation of modified canal staining and clearing technique, cone-beam computed tomography, spiral computed tomography and plain and contrast medium-enhanced digital radiography in studying root canal morphology. J Endod. 2010; 36:1547-1551
AAE and AAOMR joint position statement: use of cone beam computed tomography in endodontics 2015 update. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015; 120:508-512
Yong SL. Prophylactic treatment of dens evaginatus. ASDC J Dent Child. 1974; 41:289-292
Bazan MT, Dawson LR. Protection of dens evaginatus with pit and fissure sealant. ASDC J Dent Child. 1983; 50:361-363
Sim TPC. Management of dens evaginatus: evaluation of two prophylactic treatment methods. Dent Traumatol. 1996; 12:137-140
Chen R-S. Conservative management of dens evaginatus. J Endod. 1984; 10:253-257
Reynolds K, Johnson JD, Cohenca N. Pulp revascularization of necrotic bilateral bicuspids using a modified novel technique to eliminate potential coronal discolouration: a case report. Int Endod J. 2009; 42:84-92
Leith R, O'Connell AC. Selective reduction of talon cusps-a case series. J Clin Pediatr Dent. 2018; 42:1-5
Pledger DM, Roberts GJ. Talon cusp: report of a case. Br Dent J. 1989; 167:171-173
Kumar V, Chawla A, Logani A, Shah N. Mineral trioxide aggregate pulpotomy: an ideal treatment option for management of talon cusp. Contemp Clin Dent. 2012; 3:491-493
Smail-Faugeron V, Picou Rollin J, Muller Bolla M, Courson F. Management of non-syndromic dens evaginatus affecting permanent maxillary central incisors: a systematic review. BMJ Case Rep. 2016;
Stanley HR, White CL, McCray L. The rate of tertiary (reparative) dentin formation in the human tooth. Oral Surg Oral Med Oral Pathol. 1966; 21:180-189
Keane J, O'Sullivan R, Field D Talon cusps: a review. J Ir Dent Assoc. 1997; 43:86-88
Hattab FN, Hazza'a AM. An unusual case of talon cusp on geminated tooth. J Can Dent Assoc. 2001; 67:263-266
Sakiyama Y. Considerable supplement on the central cusp in the lower second molar. Kaibogaku Zasshi. 2001; 76:407-410
Nagaveni N, Umashankara K. Maxillary molar with dens evaginatus and multiple cusps: report of a rare case and literature review. Int J Oral Health Sci. 2013; 3
Nabeel S, Hegde U, Danish G Dens evaginatus on a maxillary molar: case report and an overview. Dent Follicle. 2017; 10
Thakur NS, Thakur S. Double dens evaginatus on permanent maxillary first molar: a case report of this rare occurrence. Indian J Dent Sci. 2017; 2
Prevalence of dens evaginatus (DE) is very rare in molars, with only nine previous cases described, and all involving patients of Asian heritage. This article presents two unique cases of molar DE in European patients of 10 and 5 years of age, and a review of the current literature. The aim of the article is to review the aetiology, diagnosis, clinical significance and management of teeth affected with DE.
CPD/Clinical Relevance: Dens evaginatus describe teeth with supplemental cusps that may contain pulpal tissue. These are susceptible to wear, fracture and caries. This may lead to pain and pulpal necrosis. Early diagnosis and management are key to prevent symptoms and optimize tooth prognosis
Article
Matthew Chung
Dens evaginatus (DE) is a rare developmental anomaly describing teeth with supplemental cusps or protuberances consisting of enamel surrounding a core of dentine, and typically with pulpal tissue.1 Consequently, they are susceptible to pulpal exposure and introduction of pathology into the root canal system when worn or fractured. 2 This underpins the importance for early detection and dental intervention.
Epidemiology
The prevalence of DE ranges from 0.5% to 4.3%,3 with genetic predisposition favouring 2% of the Asian population,4 in particular those of Mongolian origin with 1.29–3.6% among Chinese and as high as 15% observed in Alaskan Eskimo natives.3,5 Limited cases in African-Americans and Caucasians have also been described.6,7,8
Aetiology
The precise aetiology is unclear, although autosomal dominant and X-linked transmissions have been suggested.9,10 It is believed that DE arises as a result of abnormal evagination of the internal epithelium and ectomesenchymal cells of the dental papilla into the stellate reticulum of the enamel organ in the morphodifferentiation stage of tooth development.3
This is initiated by enamel knots that stimulate proliferation of the adjacent epithelial and underlying mesenchymal cells of the dental papilla, which ultimately determine the size, shape and location of cusps and teeth.11 Signal molecules including bone morphogenic proteins, fibroblast growth factors and transforming growth factors are activated by enamel knots, which in turn regulate enamel knot activity.11,12 Consequently, disruption to the enamel knots or signal molecules potentially results in dental anomalies, with examples of animal studies associating overexpression of the signal molecule, ectodysplasin, with formation of additional cusps.13,14 Disruption to SHH, PAX and MSX genes have also been linked.15,16,17 Cuspal development appears to be primarily polygenetic although environmental influences can not be ruled out.15
Clinical significance
Although any primary or permanent teeth can be affected, incidence is more frequent in the permanent dentition, five times more likely in the mandible, with 50% contralateral involvement, and predilection towards females.5,18 Mandibular second premolars are most commonly affected followed by mandibular first premolars, maxillary premolars and rarely molars.6,19
Evaginations most commonly arise between the buccal and lingual cusp of the premolars and central groove of the occlusal surface or lingual ridge of the buccal cusp on molars.20,21 Classifications associated with their location,3 pulpal content19 and anatomical shape22 have been devised with regard to premolars.
They should not be confused with Mulberry (Fournier's) molars, which are typically, but not exclusively associated with congenital syphilis. The unique distinguishing feature of Mulberry molars is enamel hypoplasia and resulting rudimentary cusps.23,24
The cusp of Carabelli is another supplemental cusp, which is found on the mesio-palatal cusp of maxillary first molars and disassociated from DE by the absence of pulpal tissue.25
Cuspal evaginations have been described as talon cusps on the palatal or lingual surface of anterior teeth, and as Bolk's cusps on the mesiobuccal cusp of molars. These are considered to be synonymous with DE as they share the same theory of physiological development.3,26 Prevalence of the talon cusp has been reported between 0.012% and 7.7%.27
Concomitant anomalies with DE have also been described, with hypodontia most prevalent, followed by supernumeraries, impaction and microdont maxillary lateral incisors to name a few.28 This underlines the importance of careful detection of dental anomalies in the presence of DE, as these can lead to pathological complications.
The presence of DE has significant dental implications because the pits or grooves proximal to evaginations are a source of plaque stagnation and caries development.29 Consisting of enamel surrounding a core of dentine and 70% with pulpal extensions,1,19 these evaginations can extend up to 3.5 mm from the occlusal surface of posterior teeth and 6 mm from the palatal/lingual surface of anterior teeth, introducing occlusal interferences liable to wear and fracture.8,30 This can introduce a range of complications such as sensitivity,31 pain,32 loss of vitality,33,34,35 arrestment of root development,35 abscesses,36,37 osteomyelitis38 and cellulitis.36
Separate articles have reported up to 75% of DE resulting in wear or fracture,33 14.1–40.2% becoming non-vital,39 27% associated with peri-apical abscesses,34 and 18% with radiographic peri-apical areas.40 This emphasizes the importance for early intervention to prevent pulpal involvement.
Case reports
Case 1
A 10-year-old male was referred to the paediatric dental department for root canal treatment of an immature maxillary right central incisor (UR1) with an open apex. The patient had suffered avulsion of UR1 6 months previously. The tooth had been immediately submerged in milk, re-implanted by the dentist several hours later and subsequently extirpated.
The patient presented complaining of intermittent pain from the mandibular right second primary molar (LRE) and had a medical history including asthma, repaired juxtaductal aortic coarctation, patent foramen ovale and a bicuspid aortic valve.
Examination
Intra-oral examination identified a discoloured UR1 with normal physiological mobility, buccal tenderness, draining buccal sinus and negative responsive to electric pulp testing.
Other findings included mandibular left and right second primary molars (LLE and LRE) with occlusal caries, invaginations of maxillary left and right lateral incsiors (UL2 and UR2), and evaginations on all four permanent first molars.
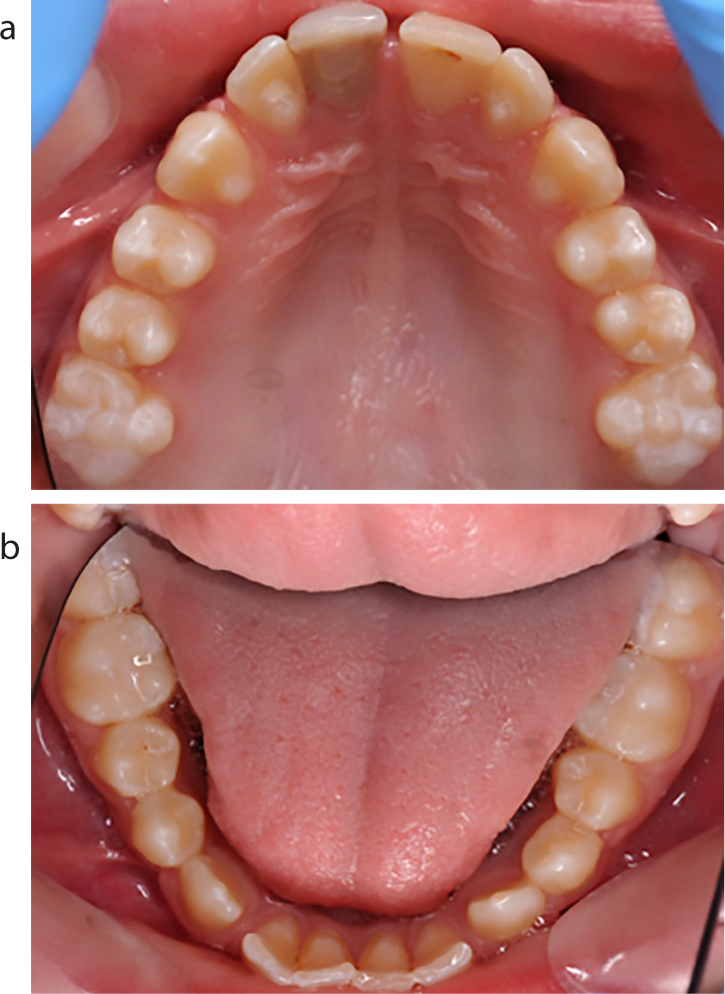
Clinically the maxillary left and right first molars (UL6 and UR6) had two evaginations arising from the occlusal surface; one between the mesio-buccal and mesio-palatal cusp and another between the disto-buccal and mesio-palatal cusp. The mandibular left and right first molars (LL6 and LR6) had abnormally wide central fissures and evaginations on the mesio-buccal cusps. There was no pathology, premature contact, wear or fracture of the evaginations (Figure 1).
Figure 1. Case 1 at 12-month review. Invaginations on maxillary lateral incisors. Evaginations of maxillary canines and first molars, and mandibular first molars.
Radiographs
Peri-apical radiographs identified peri-apical pathology and incomplete root formation with UR1. UL2 and UR2 had type 2 dens in dente with no periapical pathology (Figure 2).41
Figure 2. (a, b) Case 1 pre-operative periapical radiographs. Type 2 dens in dente in maxillary lateral incisors, and periapical pathology with arrested root development associated with maxillary right central incisor.
An orthopantomogram confirmed the presence of all developing teeth except for maxillary wisdom teeth, taurodont UL6 and UR6, supplemental cusps with unerupted maxillary left and right canines (UL3 and UR3) and caries of LLE and LRE with pulpal involvement. Pulpal extensions were not evident in any evaginations (Figure 3).
Figure 3. Case 1 pre-operative orthopantomogram with caries visible in mandibular left and right second primary molars. Note the taurodont maxillary first molars, and evaginations visible on unerupted maxillary canines.
Treatment
Initial treatment comprised extensive preventive advice, dressing of UR1 with non-setting calcium hydroxide, extraction of unrestorable LLE and LRE under local anaesthetic, and fissure sealants for UL2 and UR2.
The case was complicated by the patient's poor oral hygiene and failure to attend for fissure sealants of LL6 and LR6, which contributed to the development of occlusal caries in both teeth 6 months later. This was identified clinically and on bitewing radiographs. Pulpal extensions were not discernible on these. Regression of UR1 periapical area was confirmed at month 9 and restored using MTA with backfill thermo-obturation and composite (Figure 4).
Figure 4. (a–c) Case 1: 12-month review radiographs. Peri-apical of maxillary right central incisor completed root canal treatment with resolving peri-apical area. Palatal evaginations of maxillary canines, and occlusal carries in mandibular first molars visible on bitewing radiographs.
Case 2
A 5-year-old male was referred from the community dental service for extraction of carious teeth.
His medical history was complex and included an unspecified genetic syndrome, global developmental delay, left atrophic kidney, obstructive sleep apnoea, dolichocephaly, recurrent urinary tract infections, gastro-oesophageal reflux with hiatus hernia, osteopenia, elevated BMI and small patent ductus arteriosus.
The patient presented with extensive caries affecting all primary teeth except for the mandibular primary incisors. LR6 and LL6 had hypoplasia with post-eruptive breakdown.
Evaginations were noted on the UL6 and UR6 which appeared to be caries free clinically and radiographically, and without obvious radiographic evidence of pulpal extensions. (Figure 5)
Figure 5. Case 2: pre-operative orthopantomogram with breakdown of lower left first molar, and caries affecting all primary teeth except for the mandibular primary incisors.
The patient subsequently underwent extraction of all carious primary teeth, LL6 and LR6 under general anaesthesia (Figure 6). They were reappointed for fissure sealants of UL6 and UR6.
Figure 6. Case 2: post-extraction, with evaginations on maxillary first molars.
Discussion
DE in both patients were managed conservatively. Peri-apical radiographs were preferred to identify pulpal extensions, but unfortunately, both patients were unable to tolerate these.
The patient in Case 1 had good interdigitation of the maxillary first molars with the mandibular first molars, with no symptoms, occlusal interference, wear, fracture, pathology or pupal extensions detected. The patient was also aged 10, which suggested that the occlusion had been stable, and teeth structurally sound for at least 4 years. Review was undertaken at 12 months with no changes to the cuspal integrity, thus suggesting that the conservative approach was appropriate.
Case 2 was free of symptoms, occlusal interference, pathology, pulpal extensions, wear and fracture.
In consideration of this, a conservative option was also agreed to provide resin fissure sealants for all first molars without occlusal adjustment, and to maintain regular review for caries and tooth wear.
These cases are unique because there have been no reported cases of molar DE in those of European origin, with only nine cases previously described, all involving patients of Asian background (three Indian, two Japanese, one Malaysian, one Thai, one Hmong and one Chinese) between the ages of 9 and 56 years (Table 1).
Two cases in Table 1 described patients with DE presenting with generalized pain. This reinforces the importance for clinicians to be vigilant for DE as a potential cause of odontogenic pain, especially where evaginations may be difficult to identify due to diminutive formation, wear, fracture or caries. As mentioned previously, concomitant dental anomalies may also be present with DE, and clinicians should be vigilant for these.
Pre-operative dental radiographs should also be considered in the presence of DE, with three of the cases in Table 1 demonstrating visible pulpal extension on peri-apical radiographs. DE should also be taken into consideration when reporting radiographs on unerupted teeth because early diagnosis can allow planning for timely intervention post eruption. Superimposition, distortion, magnification and misrepresentation may lead to misdiagnosis on 2D radiographs.42 This may result in pulpal extensions being missed in teeth with DE. Although canal morphology has been demonstrated to be accurately visualized in 99% with cone beam computed tomography (CBCT) compared with 84% with peri-apical radiographs, its use should be limited to cases where diagnostic benefit exceeds risk of increased radiation dose.43,44
The literature has extensively reported various treatments for DE in premolars and maxillary central incisors:
Oehlers et al proposed intermittent grinding of the evagination alone, with the aim of stimulating tertiary dentine formation and providing a barrier to pulpal extension, although results were varied and tertiary dentine formation unreliable.19 Yong successfully treated 39 immature, vital and asymptomatic teeth with prophylactic removal of the tubercle, pulp capping and restoration with amalgam.45 The aim of this was to enable continual root development. Bazan and Dawson suggested the use of fissure sealants, although this still left the evagination liable to wear and fracture, and they subsequently suggested resin-filled restoration coverage for improved strength.46 Hill and Bellis identified that this introduced occlusal interferences, and recommended reducing the tubercle down to dentine, and providing pulp capping with composite resin restoration.6
Sim compared this, and found that development of pulpal signs and symptoms occurred in 0.52% of teeth restored with a preventative resin restoration (Hill and Bellis method) compared to 5.37% using amalgam (Yong method).47
Chen removed enamel from the evagination until the underlying dentine was revealed, and then treated this with 8% stannous fluoride to stimulate reparative dentine formation. However, this was not appropriate for cases where pulpal extensions extended to the dentino-enamel junction.48
Selective reduction of the evagination is now the frequently described management technique. The intention is to allow for stimulation of reparative dentine, pulpal regression and continued root development.
Levitan and Himel categorized DE into five types and devised a treatment summary for teeth with mature and open apices20 (Table 2).
Type INormal pulp with mature apex
Reduce opposing occluding tooth and apply fluoride for desensitizationApply acid-etched flowable light-cured resin to tubercle 6-month review and 1-year radiographic review to assess occlusion, resin and pulpal/peri-radicular statusWhen review demonstrates adequate pulp recession, remove tubercle to occlusal level and apply resin coverage
Type IINormal pulp with immature apex
Same as type I, except review every 3–4 months until development of mature apex
Type IIIInflamed pulp with mature apex
Conventional root canal therapy and restoration
Type IVInflamed pulp with immature apex
Shallow MTA (mineral trioxide aggregate) pulpotomy, glass ionomer layer and acid-etched light-cured resin
Type VNecrotic pulp with mature apex
Conventional root canal therapy and restoration
Type VINecrotic pulp with immature apex
MTA root end barrier, glass ionomer layer and acid-etched light-cured resin
Revascularization of the immature apex of mandibular premolars with DE has also been described, with extraction usually being a last resort where alternative options are not feasible, or have failed.49
Despite reports describing management of evaginations, there is no standardized protocol and present evidence is low with no randomized control trials.
Leith and O'Connell conducted a case series looking at selective reduction and total removal of talon cusps in paediatric patients.50 Talon cusps have been classified into three types, with recommendation for surgical intervention for type 1 cases due to their size and cause for concern over aesthetics and occlusion. Type 1 is defined as cusps spanning at least half the distance from the cemento-enamel junction (CEJ) and the incisal edge. Type 2 is less than half this distance and Type 3 is an enlarged cingulum. Preventive advice and fissure sealing the developmental groove to reduce caries risk is the recommended management for Types 2 and 3. Significantly, all 10 teeth managed by selective reduction maintained pulp vitality. Four teeth were managed with complete reduction, and this was based on clinician experience and preference, size of talon cusp and patient compliance. One tooth had a direct pulp cap and remained vital after 4 years. The other three had partial pulpotomy with two devitalizing. A small sample size was acknowledged and maintenance of vitality with radical reduction of talon cusps with pulpotomies has been reported in literature.51,52
A protocol for selective reduction for talon cusps has been devised by Leith and O'Connell.50 This differs from Levitan and Himmel20 in that selective reduction ceases at the point of acceptable aesthetics and occlusion, rather than eventual total removal of the evagination. The opposing tooth is also not reduced.
A systematic review by Smail-Faugeron et al looking at DE in permanent maxillary central incisors isolated 34 case reports and 39 evaginations.53 Cases free from radiographic pulpal extension, pathology and occlusal interference were not treated (five cases). The remaining cases (14), which showed absence of pulpal extensions radiographically, received either selective (nine cases) or complete reduction with fluoride desensitizer (five cases). Of the nine receiving selective reduction, five received no further treatment, one had pulpal necrosis and four were restored. Five cases underwent completed reduction in a single appointment, with three needing pulp capping with calcium hydroxide or mineral trioxide aggregate, one needing pulpotomy with formocresol and calcium hydroxide and one requiring pulpectomy. For those cases that showed no radiographic pulpal involvement radiographically (20 cases), complete reduction was completed in a single appointment (18 cases) and extraction in two cases. Eleven retained vitality and were subsequently restored. Seven required pulpal treatment for irreversible pulpitis or pulpal necrosis. Only 15 of the 34 cases that had treatment included follow up, ranging from 3 to 24 months. Thus, it is unclear whether pulpal symptoms developed in the remaining 19 cases.
Based on the above two studies, it appears that radical reduction has the advantage of cuspal removal in one appointment, although this tends to result in pulpal exposure that can affect pulpal prognosis. This requires pulp capping or pulpotomy, which can still result in loss of vitality. The procedure may also be more difficult to tolerate because local anaesthesia is required, and overall, there is a greater restorative burden for the patient to endure, especially for young paediatric patients. Perhaps this technique is more appropriately reserved for those with complicating factors, such as complex medical histories or for patients with behavioural management issues who can not tolerate multiple appointments requiring local anaesthetic; however, the risk of subsequent pulpal complications and its management are still present.
Suggestions have been made for selective reduction to be carried out progressively as reparative dentine is deposited at an average of 1.49 μm per day, with the optimum rate over the first 6 weeks and decreasing thereafter.54 Desensitizing agents are recommended over application of bonding agents for this reason as the latter would impede dentine formation.55
Varying amounts of reduction at each visit ranging from 1 mm to 3 mm have been reported.30,56,57 Gauging proximity to pulpal exposure from patient feedback of development of sensitivity with treatment in the absence of local anaesthesia has been suggested.47 It has also been suggested for dentine to be removed from the cusp length rather than the tip to promote optimal reparative dentine formation because this is where more odontoblasts are present.58
An interval of 6–8 weeks between each reduction is recommended, with thicker dentine observed at 8 weeks than at 5 weeks.59,60
Conclusion
A review of the literature has highlighted the importance of timely identification and regular review of DE to prevent development of pain and infection. This is particularly pertinent in inconspicuous cases where there is caries, wear, fracture or undiagnosed odontogenic pain. DE should be monitored clinically and radiographically, especially for those of Asian descent, in mandibular teeth, premolars and contralateral teeth. The two presented cases highlight an unusual presentation of molar DE and that these should not be ruled out in those of European origin.
Further high-level evidence research is required to determine criteria for selecting conservative versus surgical management (selective or radical reduction) of supplemental cusps in teeth with immature and mature apices, and to produce a protocol to describe the optimal method for providing each technique.