Irish Oral Health Services Guideline Initiative. Pit and Fissure Sealants: Evidence-based guidance on the use of sealants for the prevention and management of pit and fissure caries. 2010. https://www.lenus.ie/handle/10147/113084
Liu BY, Xiao Y, Chu CH, Lo EC Glass ionomer ART sealant and fluoridereleasing resin sealant in fissure caries prevention – results from a randomized clinical trial. BMC Oral Health. 2014; 14 https://doi.org/10.1186/1472-6831-14-54
Bagherian A, Sarraf Shirazi A, Sadeghi R Adhesive systems under fissure sealants: yes or no? A systematic review and meta-analysis. J Am Dent Assoc. 2016; 147:446-456 https://doi.org/10.1016/j.adaj.2016.01.014
Cagetti MG, Carta G, Cocco F Effect of fluoridated sealants on adjacent tooth surfaces: a 30-mo randomized clinical trial. J Dent Res. 2014; 93:(7 Suppl)59S-65S https://doi.org/10.1177/0022034514535808
Beauchamp J, Caufield PW, Crall JJ Evidence-based clinical recommendations for the use of pit-andfissure sealants: a report of the American Dental Association Council on Scientific Affairs. Dent Clin North Am. 2009; 53:131-147 https://doi.org/10.1016/j.cden.2008.09.003
Cabral RN, Faber J, Otero SAM Retention rates and caries-preventive effects of two different sealant materials: a randomised clinical trial. Clin Oral Investig. 2018; 22:3171-3177 https://doi.org/10.1007/s00784-018-2416-z
Mickenautsch S, Yengopal V Caries-Preventive effect of high-viscosity glass ionomer and resin-based fissure sealants on permanent teeth: a systematic review of clinical trials. PLoS One. 2016; 11 https://doi.org/10.1371/journal.pone.0146512
Zhang W, Chen X, Fan MW Do light cured ART conventional highviscosity glass-ionomer sealants perform better than resin-composite sealants: a 4-year randomized clinical trial. Dent Mater. 2014; 30:487-492 https://doi.org/10.1016/j.dental.2014.01.016
Finucane D Restorative treatment of primary teeth: an evidence-based narrative review. Aust Dent J. 2019; 64:(Suppl 1)S22-S36 https://doi.org/10.1111/adj.12682
Avila WM, Hesse D, Bonifacio CC Surface conditioning prior to the application of glass-ionomer cement: a systematic review and meta-analysis. J Adhes Dent. 2019; 21:391-399 https://doi.org/10.3290/j.jad.a43183
McCabe JF, Walls A, 9th edn. Oxford: Blackwell; 2008
Cury JA, Tenuta LM How to maintain a cariostatic fluoride concentration in the oral environment. Adv Dent Res. 2008; 20:13-16 https://doi.org/10.1177/154407370802000104
Cole BO, Welbury RR The atraumatic restorative treatment (ART) technique: does it have a place in everyday practice?. Dent Update. 2000; 27:118-123 https://doi.org/10.12968/denu.2000.27.3.118
Ebnesajjad S, Ebnesajjad C: Elsevier; 2013
Antonson SA, Antonson DE, Brener S Twenty-four month clinical evaluation of fissure sealants on partially erupted permanent first molars: glass ionomer versus resin-based sealant. J Am Dent Assoc. 2012; 143:115-122 https://doi.org/10.14219/jada.archive.2012.0121
Arrow P, Riordan PJ Retention and caries preventive effects of a GIC and a resinbased fissure sealant. Community Dent Oral Epidemiol. 1995; 23:282-285 https://doi.org/10.1111/j.1600-0528.1995.tb00249.x
Williams B, Laxton L, Holt RD, Winter GB Fissure sealants: a 4-year clinical trial comparing an experimental glass polyalkenoate cement with a bis glycidyl methacrylate resin used as fissure sealants. Br Dent J. 1996; 180:104-108 https://doi.org/10.1038/sj.bdj.4808989
Lovadino JR, Martins LRM, Sartini R Evaluation, after one year, of two sealant materials: glass ionomer cement and composite sealant. Rev APCD. 1994; 48:1243-1246
Oba AA, Dülgergil T, Sönmez IS, Doðan S Comparison of caries prevention with glass ionomer and composite resin fissure sealants. J Formos Med Assoc. 2009; 108:844-848 https://doi.org/10.1016/S0929-6646(09)60415-0
Beiruti N, Frencken JE, van 't Hof MA, van Palenstein Helderman WH Cariespreventive effect of resin-based and glass ionomer sealants over time: a systematic review. Community Dent Oral Epidemiol. 2006; 34:403-409 https://doi.org/10.1111/j.1600-0528.2006.00321.x
Yengopal V, Mickenautsch S, Bezerra AC, Leal SC Caries-preventive effect of glass ionomer and resin-based fissure sealants on permanent teeth: a meta analysis. J Oral Sci. 2009; 51:373-382 https://doi.org/10.2334/josnusd.51.373
Mickenautsch S, Yengopal V Retention loss of resin based fissure sealants – a valid predictor for clinical outcome?. Open Dent J. 2013; 7:102-108 https://doi.org/10.2174/18742106201305130001
Torppa-Saarinen E, Seppä L Shortterm retention of glass-ionomer fissure sealants. Proc Finn Dent Soc. 1990; 86:83-88
de Amorim RG, Leal SC, Frencken JE Survival of atraumatic restorative treatment (ART) sealants and restorations: a meta-analysis. Clin Oral Investig. 2012; 16:429-441 https://doi.org/10.1007/s00784-011-0513-3
Birkenfeld LH, Schulman A Enhanced retention of glass-ionomer sealant by enamel etching: a microleakage and scanning electron microscopic study. Quintessence Int. 1999; 30:712-718
McLean JW, Wilson AD Fissure sealing and filling with an adhesive glassionomer cement. Br Dent J. 1974; 136:269-276 https://doi.org/10.1038/sj.bdj.4803174
Yip HK, Smales RJ Glass ionomer cements used as fissure sealants with the atraumatic restorative treatment (ART) approach: review of literature. Int Dent J. 2002; 52:67-70 https://doi.org/10.1111/j.1875-595x.2002.tb00602.x
Frencken JE, Wolke J Clinical and SEM assessment of ART high-viscosity glassionomer sealants after 8–13 years in 4 teeth. J Dent. 2010; 38:59-64 https://doi.org/10.1016/j.jdent.2009.09.004
Assistant Professor, Paediatric Dentistry, Department of Public and Child Dental Health, Dublin Dental University Hospital, Trinity College Dublin, Ireland
Fissure sealants (FS) are micro-invasive procedures that have proved to be effective in caries prevention in caries-free, first permanent molars. Within high-caries risk individuals, fissure sealants arrest the caries process in early caries lesions stages. Composite resin (CR) sealants have been recognized as the gold standard FS material; however, new evidence has emerged in relation to GIC sealants in their applicability and longevity. This review provides evidence-based information supporting the effectiveness of GIC sealants in caries prevention in comparison to CR sealants, by assessing their properties, methodology and utility in healthy and anomaly-affected teeth.
CPD/Clinical Relevance: This article will inform clinicians about the effectiveness of GIC sealants and CR sealants in caries prevention.
Article
Dental caries, regarded as the most preventable dental disease, impacts quality of life, particularly in those in lower socio-economic groups. Described as a non-communicable, dynamic biofilm-induced disease, dental caries develops from the imbalance between remineralization and demineralization processes in dental hard tissues and is influenced by biological, behavioural, and environmental factors.1 In the paediatric population, dental caries affects approximately 60–90% of school children globally, and negatively impacts eating, development and general psychosocial wellbeing resulting in the loss of school days and the inability to learn.1,2
Over the years, primary care has focused on delivering upstream interventions at a community level, and disease prevention at an individual level.1 Interventions such as fluoridated water or topical fluoride agents, diet advice, oral hygiene and fissure sealants are non-or minimally invasive approaches, which have been implemented to address the ongoing caries concern.1,2,3
Fissure sealants (FS) specifically, gained notice as as an effective, local intervention for providing protection against pit and fissure caries in privileged and underprivileged children. First introduced in the 1960s, FS involve the placement of a liquid material into the pits and fissures of teeth that are susceptible to caries.4 The micromechanical or chemically bonded protective layer from the liquid material acts as a barrier between cariogenic bacteria and the tooth surface.5 The thought behind placing sealants was to protect the molars during their eruption phase and development when they are prone to demineralization and plaque accumulation.6 FS are inexpensive, and are available in a variety of materials including carbomers, glass ionomer cement (GIC) and composite resin (CR).7,8
The effectiveness of FS is based on the ability to prevent enamel and dentine caries, whereby retention and integrity are considered to be surrogate endpoints to facilitating the preventive effect.7,9 Many studies have advocated the use of CR sealants as the gold standard in caries prevention, although other studies have recognized a similar caries prevention rate with GICs.10 The following literature review discusses and compares the GIC and CR sealants in their overall effectiveness in caries prevention.
Glass ionomer cements and composite resin: the two broad categories of sealant materials
The two broad categories of sealant materials are GICs and CRs. Other novel materials such as glass carbomers (a novel glass ionomer material containing fluorapatite with nanosize particles) and compomers have recently become available, but are not discussed.11 GIC sealants have evolved from low-viscosity cements (LVGIC) to high-viscosity cements (HVGIC). Their composition includes a glass component (fluoraluminosilicate particles) and organic acids (aqueous polymeric acid), which are set by an acid–base reaction.12 The advantages of GICs include the ability to chemically bond to enamel and dentine through covalent bonding, a reduced vulnerability in the presence of moisture, easy material manipulation and ongoing fluoride release from the cement reservoir.12 Disadvantages, however, include poor compressive and tensile strengths, poor resistance to wear and an increase in cohesive failure owing to internal porosities.12,13
CR sealants are composed of methacrylate and are a popular material for sealing fissures. They may include filler particles and are set using autopolymerization or photopolymerization reactions.1 Unlike their glass ionomer counterparts, resin sealants require micromechanical retention and adhesion, have a low modulus of elasticity, are highly sensitive to moisture and can undergo polymerization shrinkage.1,12 A summary of the material properties of GICs and CRs is given in Table 1.
Table 1. Comparison of the material properties of GIC and CR sealants.11,12,14,15
Properties
Glass ionomer cements
Composite resins
Biological/biocompatibility
Good: have a fluoride reservoir where fluoride ions can replace the hydroxy ions in hydroxyapatite, resulting in a greater resistance to acid attacks and caries owing to a lower critical pH of 4.5
Good: generally acceptable biocompatibility. BPA was a component of concern but has been eliminated from most resin-based materials
Mechanical
Poor: material is brittle with a flexural strength of 15–20 MPa, a tensile strength of 12 MPa, and the tendency to undergo cohesive failure with a stress of 5 MPa
Good: depends on the filler content and type, and degree of porosity. Lower modulus of elasticity that increases breakdown at margins
Physical
Good: powder and liquid ratios are pre-mixed by a manufacturer resulting in dense material with trituration versus a crumbly material
Poor: polymerization shrinkage increases with the amount of filler particles and results in dimensional changes
Rheological
Fair: working time and setting time are both reasonable
Good: working time is good with the absence of direct light, and setting time is quick, but is dependent on ideal light activation
Chemical
Poor: mature glass ionomers are particularly susceptible to acid erosion from saliva, plaque, and acidic drinks and often need varnish to protect them
Fair: light units are required to emit wavelengths, in the range 480–530 nm, to cure the composite. These units are depth-dependent, and curing effectiveness reduces as the depth of the composite increases
Thermal
Good: thermal diffusivity value is similar to dentine, which helps protect the pulp from thermal insults
Good: depends on the inorganic filler content (the higher the filler content, the lower the coefficient of thermal expansion), but thermal diffusivity is similar to dentine
Adhesive
Good: uses chemical bonding to adhere to enamel and dentine and does not fully depend on conditioner for adhesion
Fair: successful bonding to enamel and/or dentine requires a multi-step process involving etchant, primer and bond. Optimal results rely on moisture control
Aesthetic
Fair: reasonable shade match for most teeth, but not all
Good: shade match applies to almost all teeth and provides an optimum appearance
Applicability of composite resin and glass ionomer sealants
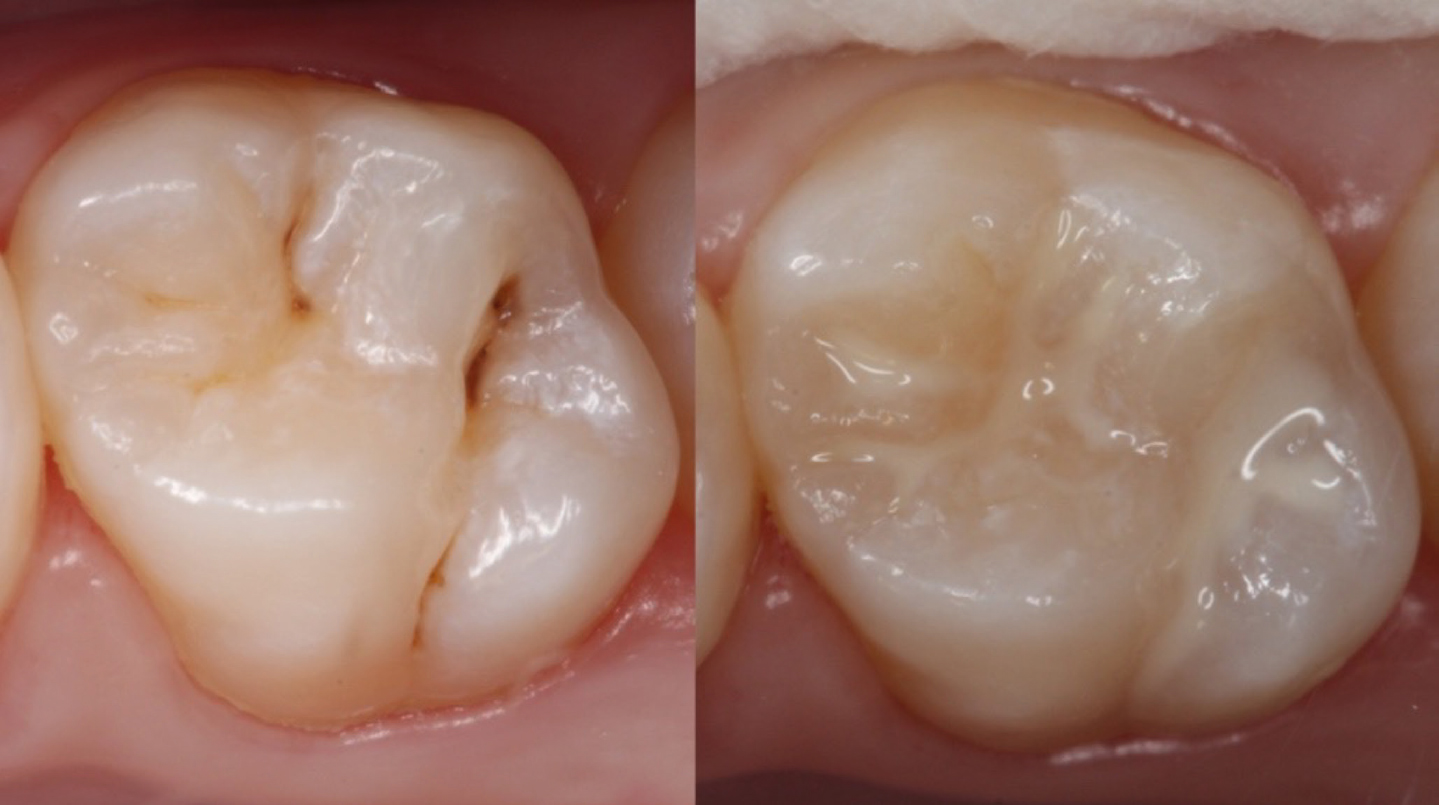
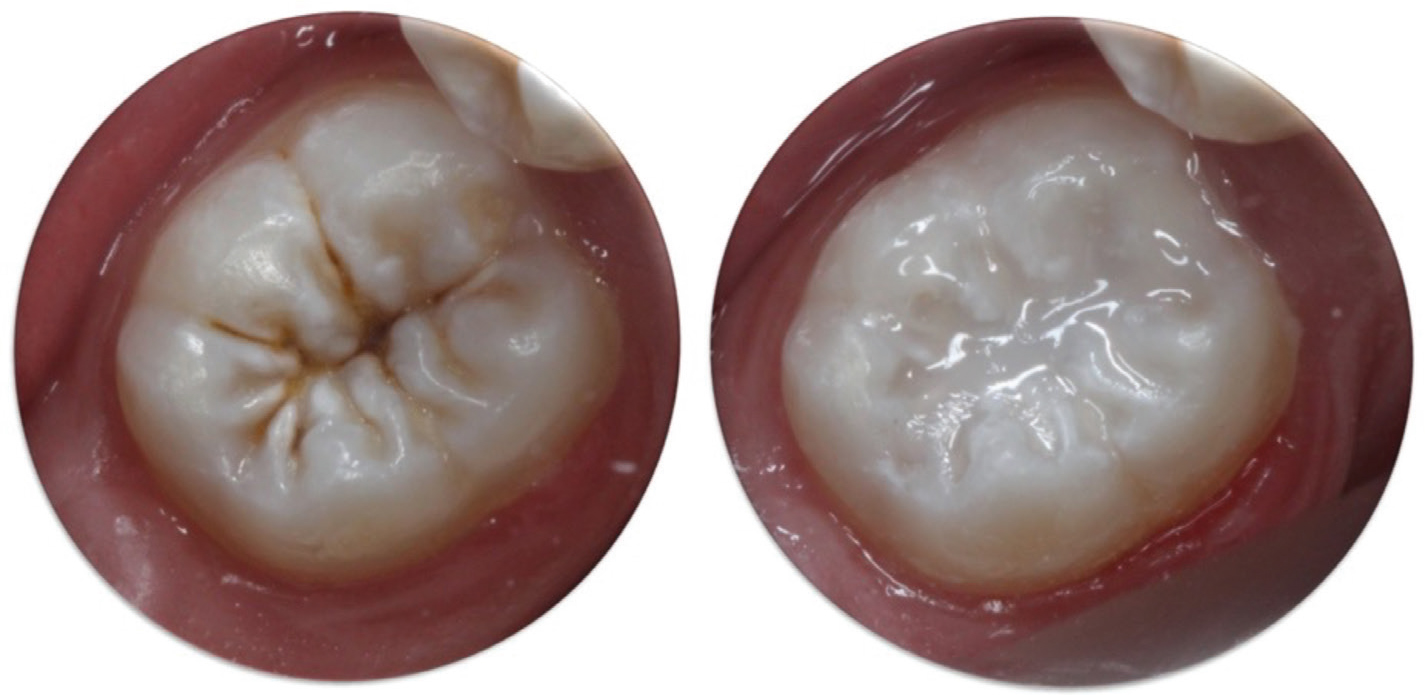
The technique and applicability of CR sealants (Figure 1) is dependent on moisture control, good isolation, and an even application with a probe to provide a barrier between bacteria and the tooth surface. Although their longevity is satisfactory, they are difficult to place in erupting teeth and are prone to adhesive failure, necessitating re-application. GIC sealants (Figure 2) have earned a place in caries prevention as an effective atraumatic restorative technique, a minimally invasive treatment modality in which hand instruments are used and GIC is placed as a restorative material.16 The provision of GIC sealants has been associated with an increased preventive effect following loss of retention as a result of cohesive failure and increased effectiveness in preventing caries in patients with and without dental anomalies, such as molar–incisor hypomineralization (MIH).
Figure 1. illustrates a before and after clinical example of a first permanent maxillary molar sealed using CR sealant (Helioseal, Ivoclar).Figure 2. illustrates the use of a high-viscosity GIC sealant (Fuji IX; GC Corp) in a partially erupted first mandibular molar.
Application technique for composite resin-based sealants5
Table 2 shows the steps involved in application of CR sealants.
Table 2. Technique and iIllustrations for the application of resin-based sealant.5
Step 1 Clean the surface using pumice and a prophylaxis brush to remove biofilm. Do not use oily prophylaxis pastes because they can interfere with adhesion Moisture control is fundamental when applying resin-based sealants. Rubber dam isolation can be used, however, a good isolation using cotton rolls and saliva ejector might also be effective
Step 2 Etch the surface using 35–37% phosphoric acid for 15 seconds
Steps 3–5 Rinse with water until complete removal of the acid for at least 10 seconds. After rinsing, make sure that the surface is completely dry
Step 6 The use of adhesive system (bond) beneath fissure sealants can increase the retention of the disuse sealants. Etch-and-rinse systems are recommended over self-etch ones. Apply a thin layer and air thin before light curing
Step 7 Apply the sealant using a dental probe or the applicator tip provided by the manufacturer, directing it towards the centre of the pits and grooves. Take care to not incorporate bubbles into the sealant material. All pits and fissures should be sealed Light cure for 20–40 seconds, according to the manufacturer's instructions
Step 8 Check your work: evaluate the entire surface of the sealant with a dental probe to ensure its integrity. Check the occlusal contacts using an occlusion paper. Carefully remove any excess with a composite finishing bur
The most common evidence-based technique for using GIC sealants is the atraumatic restorative technique. This technique can also be used outside a dental setting and is known to be a nonaerosol generating procedure. The use of a high-viscosity glass ionomer cement is recommended (Table 3).
Table 3. Technique and iIllustrations for the application of GIC sealants.
Step 1 Remove debris from the pits and fissures using a sharp probe or a toothbrush
Step 2 Apply the surface conditioner (polyacrylic acid) to the surface with a cotton wool pellet or micro-brush for 10 seconds.
Steps 3 and 4 Wash the surface using wet cotton pellets three times Dry the surface using dry cotton pellets three times Mix the GIC following the manufacturer's instructions (hand mixed or encapsulated)
Steps 5 and 6 Place the GIC mixture into the pits and fissures with the applier or a flat plastic and spread it over the pits and fissures
Step 7 Finger-press technique: press the GIC mixture with your index finger. A thin layer of petroleum jelly can be used
Steps 8–10 Remove excess glass ionomer material with hand instruments (probe) and floss between the contact points. Check the occlusion with occlusion paper and remove any excess material with a hand excavator Apply a new layer of petroleum jelly over the sealant Ask the patient not to eat for at least 1 hour
Failure and associated retention
CR sealants generally undergo adhesive failure as a result of poor moisture control, increased technique sensitivity and/or wear, in comparison to GIC sealants, which experience cohesive failure. The difference between the two materials lies in the location of the failure. Cohesive failure is the fracture of material, causing a layer of adhesive to remain on the adherend.17 Adhesive failure, on the other hand, is an interfacial fracture between the adhesive and adherend.17 In the context of sealants, adhesive failure associated with CR is considered to be a poor mechanical property, as the fracture of material would leave the pits and fissures of the tooth surface exposed to cariogenic bacteria, in comparison to their GIC analogues.
Implications of cohesive failure on caries prevention
From the current evidence, if a loss of retention in a GIC sealant occurs as a result of cohesive failure, the caries preventive effect still remains, unlike CR sealants that undergo adhesive failure leaving exposed, unprotected fissures. The caries preventive effect of GIC sealants is associated with the ongoing fluoride leaching and the barrier against bacterial invasion, from the fragments in the deeper pits and fissures.3,18
Clinical trials comparing both sealant materials
Multiple randomized controlled trials (RCT) and field studies have been published since the 1990s to compare the caries preventive effectiveness of GIC and CR sealants. For example, a split mouth trial compared GIC sealants to CR sealants with regards to retention and caries prevention.19 GIC sealants were 80.6% effective in caries prevention, had a 19% risk of developing caries in the sealed teeth and both CR and GIC sealants had an average retention rate of 4 years.19
Other studies showed promising results in caries prevention, while both materials showed similar retention failure rates.20,21,22 There tended to be fewer caries or no caries development in GIC sealed teeth despite the poor retention after a 1- and 4-year-follow up.20,21,22 Shortcomings in the studies regarding the difference in experience between professionals placing and assessing the sealants and technique were explained.21,22 To address these disadvantages, an RCT using one operator to place resin-modified GIC and high-viscosity GIC sealants was carried out. The results of the study were divided into traditional and modified categories for sealant retention and showed that over 2 years, high-viscosity GICs had excelled.9 Over 24 months, it was found that caries prevention was optimal in both sealants.9 These findings not only reiterated the inverse relationship between sealant retention and caries prevention, supported by electron microscopy, but eliminated the influence of operator application in the success of the sealant.
Systematic reviews have analysed the RCTs performed and the caries preventive effect over multiple years.10,23,24,25 Significant findings revealed that fewer caries had developed in GIC sealed teeth 4–5 years after placement compared to CR sealed teeth.10,23,25 However, after longer periods (approximately 7 years), there was an increase in caries development in GIC sealed teeth. This would be expected because the average clinical prognosis for GIC and CR sealants is approximately 4 years.10,23,24,25 The systematic reviews found similar rates of caries prevention for both GIC and CR sealed teeth, with neither material having superiority. However, the trials and reviews included poor-quality assessment with regards to the confounding factors, dissimilar units of randomization and lack of information regarding population caries risk, oral hygiene behaviours and systemic fluoride.10,21,23,25
In vitro studies assessing factors influencing caries prevention
Sealant penetration and fluoride leaching are factors that have been analysed in vitro. Torpa-Saarinen and Seppa examined the penetration of a GIC sealant material in the pits and fissures of molar teeth.26 Out of 28 teeth, there was full penetration into the deepest parts of the fissures in 67% of the teeth.26 High-viscosity GIC was also considered to be associated with full penetration of molar teeth when using the finger-press technique, as opposed to conventional GIC sealants that use the probe application technique.27,28,29,30 When assessing fluoride leaching, GIC sealants were associated with a fluoride reservoir that functions to release small amounts of fluoride over time.31 Multiple studies have advocated the rechargeability of GIC sealants with topical sodium fluoride application to promote ongoing remineralization; however, sealant materials should not completely depend on an adjunct to promote their intra-oral success.31,32,33,34
Evidence of sealant retention using microscopy
Numerous in vivo RCTs and case studies have compared the effectiveness of the sealants in caries prevention of the first permanent molars while using scanning electron microscopy (SEM) or stereomicroscopy to assess the sealant retention. Low-viscosity GIC sealants have been analysed under SEM and stereomicroscopy and compared with high-viscosity GIC sealants.6,26,30,35 The primary difference between the two was their retention.
Low-viscosity GIC sealants have shorter lifespans, predominantly as a result of their application with a probe. High-viscosity GIC sealants have a longer lifespan because the finger-press technique improves the sealing potential through calcium bonding, and facilitates fluoride leaching in the deeper areas of the pits and fissures of the teeth.16 Both low- and high-viscosity GICs were visible in the deeper parts of the pits and fissures, even if there had been complete clinical loss of the sealant. The results of the studies hypothesized and supported the ongoing caries-preventive effect, from the ongoing leaching of the fluoride from the GIC remnants present in the pits and fissures.6,26,30,35 Therefore, the clinical loss of a GIC sealant did not lead to the complete biological failure of the material's caries-preventive effect.
GIC sealants in teeth with anomalies
The application of sealants in various states of health is equally important in assessing caries prevention from a holistic point of view. Sealants should ideally protect teeth with anomalies, as well as healthy teeth, against caries. For example, molar–incisor hypomineralization affects 1 in 6 children worldwide, and can present with rapid caries progression owing to the increased sensitivity of the teeth and an inability to perform adequate oral hygiene.36
A 1-year RCT of a GIC sealant assessed its effect in preventing caries and posteruptive breakdown in patients with MIH patients.37 Among 34 MIH cases, there was a 77% increase in caries development in unsealed MIH-affected molars compared with those which received the GIC sealants.37 As observed with healthy teeth, the caries preventive effect is a result of the barrier formed between the pits and fissures and the oral environment and the ongoing release of fluoride. However, in the case of MIH, the application of GIC sealants also provides effective relief against dental hypersensitivity, which consequently enhances oral hygiene and makes plaque removal much more effective.38 Further research to appraise the effectiveness of GIC versus CR sealants should be performed to improve validity and identify any success of sealants in teeth with other anomalies.
Discussion
Multiple studies indicate that the retention and integrity of a sealant is not an indicator of its success against caries prevention.25 The trials were performed in multiple schoolchildren, 5–8 years of age, worldwide. Greater validity would be achieved if various populations, privileged and underprivileged, were included in the trials, versus school children alone. The presence of detection and selection bias was also questioned in certain systematic reviews, as the randomization in the trials was considered unclear and there was poor standardization in operator technique during the experiments.39
Although most clinical trials had a good research question encompassing a specific population, intervention, comparison, and outcome (PICO), all factors were not considered. There was a general lack of data discussing sealant success in various fissure patterns (U, V, I, K), the quantity of fluoride released from the GIC sealants, the quality of the remaining sealants, and the criteria used to determine a partially lost status. Systemic factors, including consumption of fluoridated water, milk, diet, etc. during the sealant placement and the caries preventive effect of sealants in dentitions affected by various genetic causes, such as amelogenesis imperfecta, were not considered. Further research should explore these local and systemic factors in relation to healthy and genetically affected teeth, and should compare which GIC sealant may be the best in terms of performance, penetration, fluoride release, etc to facilitate caries prevention. This research would benefit both privileged and underprivileged children in receiving interventions that are effective and available to all populations and all dentitions.
Conclusion
Multiple reviews, studies trials, and SEM reports have corroborated a similar effectiveness in caries prevention when comparing GIC and CR sealants over a 2–4-year period. The biological and adhesive properties of GIC sealants have led to their increased consideration in caries prevention. High-viscosity GIC sealants, specifically, have been effective in isolating tooth surfaces from the oral environment, improving ease of application in paediatric patients, and having an increased penetration rate using an atraumatic restorative technique protocol.
The versatile application and caries prevention rates therefore imply that GIC materials are as effective as CR in caries prevention. However, further studies should be undertaken to assess various outcomes and address methodological weaknesses in the current evidence.