Baccetti T A controlled study of associated dental anomalies. Angle Orthod. 1998; 68:267-274
Groper JN Macrodontia of a single tooth: review of literature and report of case. J Am Dent Assoc. 1987; 114
Brook AH Dental anomalies of number, form and size: their prevalence in British schoolchildren. J Int Assoc Dent Child. 1974; 5:37-53
Ooshima T, Ishida R, Mishima K, Sobue S The prevalence of developmental anomalies of teeth and their association with tooth size in the primary and permanent dentitions of 1650 Japanese children. Int J Paediatr Dent. 1996; 6:87-94
Rajab LD, Hamdan MA Supernumerary teeth: review of the literature and a survey of 152 cases. Int J Paediatr Dent. 2002; 12:244-254
Dugmore CR Bilateral macrodontia of mandibular second premolars: a case report. Int J Paediatr Dent. 2001; 11:69-73
Thomas MB, Greenhalgh CM, Addy L ‘Double-veneers’ – a novel approach to treating macrodontia. Dent Update. 2008; 35:479-484
Fleming PS, Xavier GM, DiBiase AT, Cobourne MT Revisiting the supernumerary: the epidemiological and molecular basis of extra teeth. Br Dent J. 2010; 208:25-30
Brook AH A unifying aetiological explanation for anomalies of human tooth number and size. Arch Oral Biol. 1984; 29:373-378
Brook AH, Elcock C, Aggarwal M Tooth dimensions in hypodontia with a known PAX9 mutation. Arch Oral Biol. 2009; 54:S57-62
Khalaf K, Robinson DL, Elcock C, Smith RN, Brook AH Tooth size in patients with supernumerary teeth and a control group measured by image analysis system. Arch Oral Biol. 2005; 50:243-248
Khalaf K, Smith RN, Elcock C, Brook AH Multiple crown size variables of the upper incisors in patients with supernumerary teeth compared with controls. Arch Oral Biol. 2009; 54:S71-S78
Bishara SE Impacted maxillary canines: a review. Am J Orthod Dentofacial Orthop. 1992; 101:159-171
Chadwick SM, Kilpatrick NM Late development of supernumerary teeth: a report of two cases. Int J Paediatr Dent. 1993; 3:205-210
Cho SY, So FH, Lee CK, Chan JC Late forming supernumerary tooth in the premaxilla: a case report. Int J Paediatr Dent. 2000; 10:335-340
Aguilo L, Gandia JL Late development of maxillary supernumerary tooth: a case report. J Clin Pediatr Dent. 1997; 22:41-44
Is there a relationship between increased tooth number and increased tooth size? a case report Jadbinder Seehra Mike Harrison Martyn T Cobourne Dental Update 2024 41:6, 707-709.
Authors
JadbinderSeehra
BDS(Hons), MFDS, MSc, MOrth, FDS
Senior House Officer, Unit of Oral Medicine, The School of Dentistry, University of Manchester, Higher Cambridge Street, Manchester, M15 6FH, UK
Senior Lecturer/Hon Consultant in Orthodontics, Department of Orthodontics and Craniofacial Development, Floor 22 Guy's Hospital, GKT Dental Institute, King's College London, London SEI 9RT, UK
A unifying theory has been proposed that links anomalies of tooth size and number. Application of this theory suggests that anomalies of tooth size and number may share a common aetiology but could also be predicted. This article highlights an association between macrodontia and hyperdontia as demonstrated by two clinical cases. These cases demonstrate a localized association and effect on the dentition and highlight the possible predictive application of this theory.
Clinical Relevance: Clinicians should be made aware of the possibility of supernumeraries associated with macrodont teeth.
Article
A number of dental anomalies exist that involve the formation of increased amounts of hard tissue. In particular, these include both macrodontia and supernumerary teeth, which appear to occur as distinct entities.1 Macrodontia or increased tooth size can be classified as true or relative, and can be generalized or isolated.2 The incidence of macrodontia in the permanent dentition ranges from 1.1% to 1.9%, depending upon the population studied,3,4 but is more common in the primary dentition.3 Supernumerary teeth are those present in addition to the normal complement within the dentition and occur with an incidence of around 0.1–3.8%, being more common in the permanent dentition.5 Despite these fundamental epidemiological differences, a number of features are seen that are common between these two conditions, which include a higher prevalence in males than females,3,5 unilateral or bilateral distribution,5,6 and occurrence within both dental arches.5,6,7 Both genetic and environmental factors have been implicated in the aetiology of both anomalies.8,9
A unifying theory has been proposed that links anomalies of tooth size and number.9 Interpretation of this theory suggests that, in cases of hypodontia, reduced dimensions of the dentition can be expected. In contrast, in cases of hyperdontia, an increase in tooth dimensions is present. Application of this theory suggests that anomalies of tooth size and number may share a common aetiology but could also be predicted. A genetic basis appears to have been identified, supporting the association between generalized microdontia and hypodontia.10 However, the association between hyperdontia and macrodontia appears to be less clear. Recent evidence suggests that this association might operate at a local level, affecting individual or groups of teeth.11,12 This article highlights an association between macrodontia and hyperdontia, as demonstrated by two clinical cases. These demonstrate a localized association as opposed to a generalized effect on the dentition and the possible predictive application of this theory.
Case 1
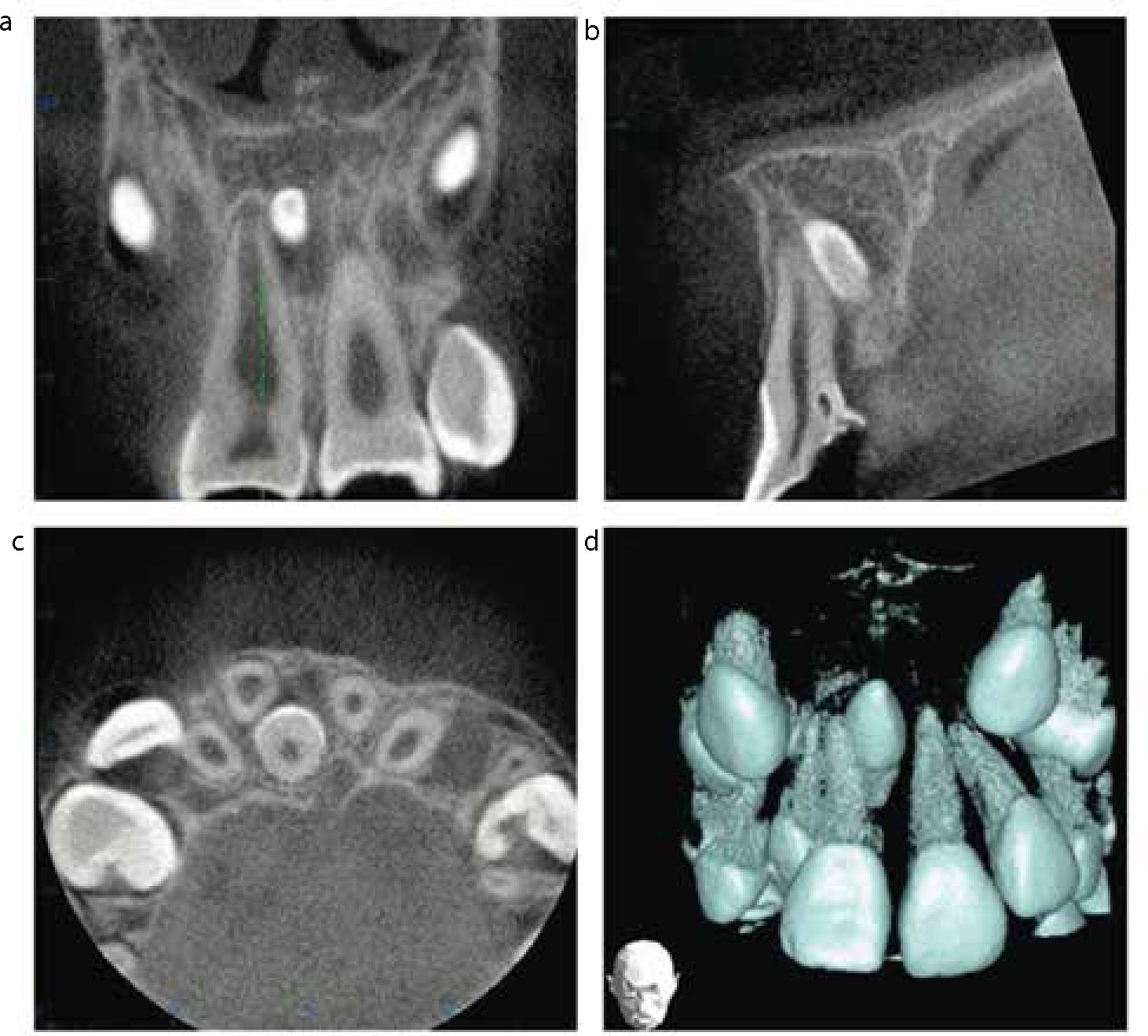
A medically fit 8-year-old female was referred by her specialist practitioner to the orthodontic department at Guy's Hospital regarding the appearance of an UR1 and unerupted midline supernumerary. She presented in the mixed dentition with significant crowding localized to the upper labial segment. On examination, the UR1 had a macrodont crown appearance with supplemental hard tissue mass located on the palatal aspect of this tooth. The mesio-distal dimension of the UR1 was measured at 11.5 mm and its antimere was 9.5 mm. Radiographic examination confirmed the presence of a macrodont crown and root associated with the UR1 and the presence of an inverted, conical supernumerary tooth (Figure 1). This was found to be positioned palatally following Cone Beam Computed Tomography (CBCT) (Figure 2a–d).
Figure 1. Periapical radiograph of macrodont UR1 and inverted conical supernumerary in Case 1.Figure 2. CBCT images of inverted conical supernumerary positioned palatally to the root of the UR1 in Case 1: (a) frontal; (b) sagittal; (c) transverse; (d) three-dimensional.
Case 2
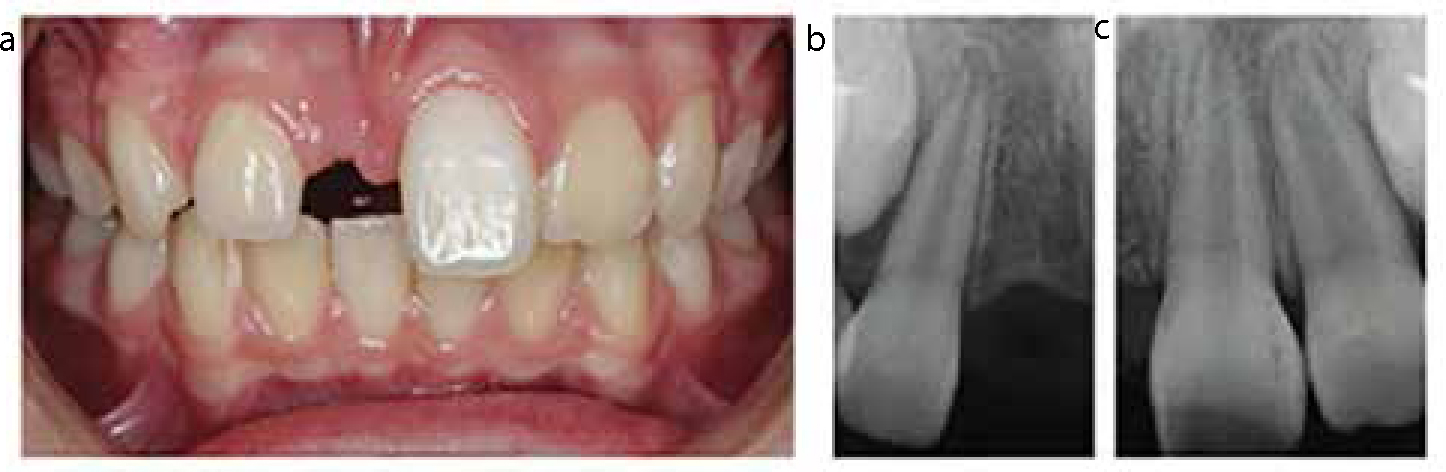
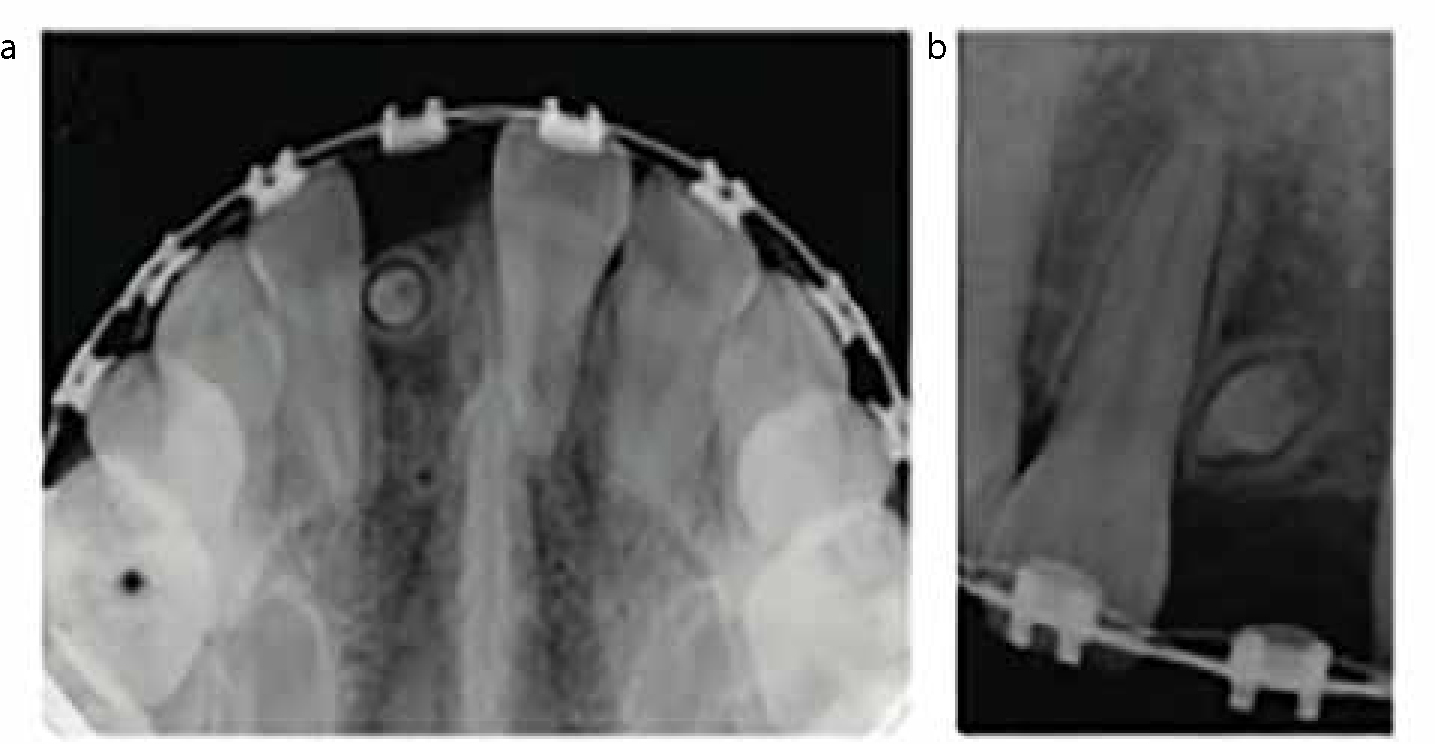
A medically fit 12-year-old female with a previous history of traumatic loss of the UR1 was undergoing a course of fixed appliance therapy within the orthodontic department at Guy's Hospital to correct her mild Class II malocclusion. Prior to treatment, a macrodont crown and root associated with the UL2 had been identified but there was an absence of any residual pathology (Figure 3a–c). The mesio-distal dimension of the UL2 was measured at 9.5 mm, which was significantly greater than the antimere (7 mm). Treatment progress with fixed appliances was uneventful; however, radiographs taken near the end of treatment revealed the incidental finding of a conical-type, late-forming supernumerary tooth located in the region of the previously avulsed UR1 (Figure 4a, b).
Figure 3. Pre-treatment view of avulsed UR1 and macrodont UL2 in Case 2: (a) intra-oral view; (b, c) periapical radiographs.Figure 4. Late-forming conical supernumerary tooth in the region of the avulsed UR1 in Case 2: (a) anterior occlusal radiograph; (b) periapical radiograph.
Discussion
The absolute criteria for macrodontia are difficult to define as diagnosis is based on clinical examination of the dentition; in particular, the affected tooth, its antimere and the adjacent teeth. Macrodontia has been defined as a tooth with a mesio-distal dimension at least 3.5 standard deviations (SD) greater than its sex-specific mean tooth size.4 Recent investigations involving measurement analysis have reported mean and SD of mesio-distal dimensions of samples and control groups.11 Using the reported female SD values11 for normal maxillary central (0.44 mm) and lateral incisor (0.46 mm) mesio-distal dimensions, the diagnosis of macrodontia in Case 1 (11.5 mm) and Case 2 (9.5 mm) is confirmed.4
The presence of associations between different tooth anomalies is clinically relevant, because the early diagnosis of one might indicate an increased risk of others.1 Indeed, there are numerous reports detailing many dental anomalies associated with palatally displaced canines.13 However, the association between tooth size and tooth number is less straightforward and requires further investigation and clarification. Classically, hypodontia is associated with a generalized reduction in dimensions of the dentition and, recently, a mutation in the PAX9 gene has been reported that is common to both microdontia and hypodontia.10 To date, most investigations into the relationship between hyperdontia and macrodontia have involved measurement analysis of dentitions associated with supernumeraries and in comparison to control groups. A generalized and larger mesio-distal tooth dimension in dentitions associated with supernumeraries has been described compared to control groups.11 This suggests that the mesio-distal dimensions of the dentition may be under genetic control. However, statistical significance was only reached for the incisors in this dimension. Similar findings for the upper incisors were confirmed in a later study.12 The results of both studies suggest that the association between macrodontia and hyperdontia may act locally, rather than the generalized effect seen between hypodontia and microdontia. In addition, supernumeraries are commonly seen in the premaxilla,5 a region in close proximity to the upper incisors, leading to the suggestion of a local field effect in this region.12 In this report, Case 1 clearly demonstrates a localized, direct association. However, Case 2 is more suggestive of a local field effect, as the supernumerary was detected on the contra-lateral side of the dental arch. In addition, Case 2 supports the possible predictable nature of the unifying theory, as the isolated macrodont UL2 was identified prior to development of the supernumerary.
Despite this evidence, a large sample study has reported no significant association between the presence of supernumerary teeth and other dental anomalies. Hyperactivity of the dental lamina is commonly cited as a possible aetiological factor in the development of supernumeraries; however, its role in determining tooth dimension is unknown. In addition, late-forming supernumeraries have been reported to develop in the premaxilla without the presence of other associated anomalies.14,15,16 Differences between these study conclusions could be explained by varying diagnostic criteria used to identify macrodontia and variation of gender specific mean tooth sizes. This lack of consistency prevents the true comparison of results within the literature. It is clear that further research into the relationship between tooth number and size is warranted at both the epidemiological and molecular level. Despite this, clinicians should be made aware of the possibility of supernumeraries if macrodont teeth are identified clinically within the dental arches.