Rivkin CJ, Keith O, Crawford PJ, Hathorn IS. Dental care for the patient with a cleft lip and palate. Part 1: From birth to the mixed dentition stage. Br Dent J. 2000; 188:78-83
Bokhout B, Hofman FX, van Limbeek J, Kramer GJ, Prahl-Andersen B. Incidence of dental caries in the primary dentition in children with a cleft lip and/or palate. Caries Res. 1997; 31:8-12
Grant HR. Cleft palate and glue ear. Arch Dis Child. 1988; 163:176-179
Ponduri S, Bradley R, Ellis PE, Brookes ST, Sandy JR, Nees AR. The management of otitis media with early routine insertion of grommets in children with cleft palate – a systematic review. Cleft Palate Craniofac J. 2009; 46:30-38
Williams A, Semb G, Bearn D, Shaw W, Sandy J. Prediction of outcomes of secondary alveolar bone grafting in children born with unilateral cleft lip and palate. Eur J Orthod. 2003; 25:205-211
Kindelan JD, Nashed RR, Bromige MR. Radiographic assessment of secondary autogenous alveolar bone grafting in cleft lip and palate patients. Cleft Palate Craniofac J. 1997; 34:195-198
Bergland O, Semb G, Abyholm FE. Elimination of the residual alveolar cleft by secondary bone grafting and subsequent orthodontic treatment. Cleft Palate J. 1986; 23:175-205
Revington PJ, McNamara C, Mukarram S, Perera E, Shah HV, Deacon SA. Alveolar bone grafting: results of a national outcome study. Ann R Coll Surg Engl. 2010; 92:643-646
Rivkin CJ, Keith O, Crawford PJ, Hathorn IS. Dental care for the patient with a cleft lip and palate. Part 2: The mixed dentition stage through to adolescence and young adulthood. Br Dent J. 2000; 188:131-134
Management of patients with non-syndromic clefts of the lip and/or palate part 2: from primary surgery to alveolar bone grafting Grant T McIntyre Dental Update 2024 41:9, 707-709.
Part 1 of this series of articles addressed the care of the child with a cleft of the lip and/or palate from antenatal diagnosis until primary surgery. The second part of this article discusses their care from primary surgery until alveolar bone grafting.
Clinical Relevance: Dentists should be aware of the different types of cleft lip and/or palate that occur and the role of the dentist in the overall management of patients who have clefts.
Article
After primary surgery has been completed, parents of babies with clefts can re-establish the family routine and enjoy their baby's growth and development. Parents are encouraged to wean babies with clefts in the same manner as a child without a cleft.
Age 6 months to toddler stage
Speech
Babies begin the babbling phase of speech development at around 6 months of age and, as a result, speech and language therapists encourage parents of children with clefts to spend as much time as possible developing good patterns of babbling through repetition of speech sounds. Forward sounds, such as /p, b, t/etc, are encouraged, whilst backing sounds, such as /k, g/etc, are discouraged as the latter may lead to substitution for certain words (eg saying ‘goy’ for ‘toy’ or ‘gaggy’ for ‘daddy’). As the baby becomes a toddler, babbling develops into more recognizable sounds and syllables. Where any anomalies are detected by the speech and language therapist, parents will be given advice about correcting the speech patterns at an early stage.
Hearing
Further audiological assessment is next carried out at 6–9 months of age using otoscopy, audiometry and tympanometry. Thereafter, hearing assessments are carried out annually until school entry at age 5 using otoscopy, age appropriate audiological assessment (with insert earphones or headphones being used whenever possible in order to gain ear specific information) and tympanometry.
Dental development
Many parents have concerns about the effect of the cleft on the dentition before any teeth erupt and therefore appreciate input from a primary care dentist or specialist in paediatric dentistry at an early stage.1 The parents are therefore encouraged to register the child with a primary care dentist. As children with clefts have an increased caries prevalence when compared with children without clefts,2 the primary care dentist has an important role in providing prevention advice and to encourage regular dental examinations, either personally or through a dental hygienist/dental therapist. This is to familiarize the child with the dental environment owing to the likelihood of multiple dental and orthodontic appointments in the years to come. Lack of sulcus depth in children with repaired clefts of the lip require the toothbrushing technique to be modified. The parents should be encouraged to lift the lip to allow the labial surfaces to be cleaned using a small-headed toothbrush.1
Age 3 to 5 years
Speech and hearing
As speech patterns develop and the toddler grows the speech and language therapist will continue to liaise with the family at multidisciplinary clinics and, where any speech anomalies are detected, a course of therapy will be offered.
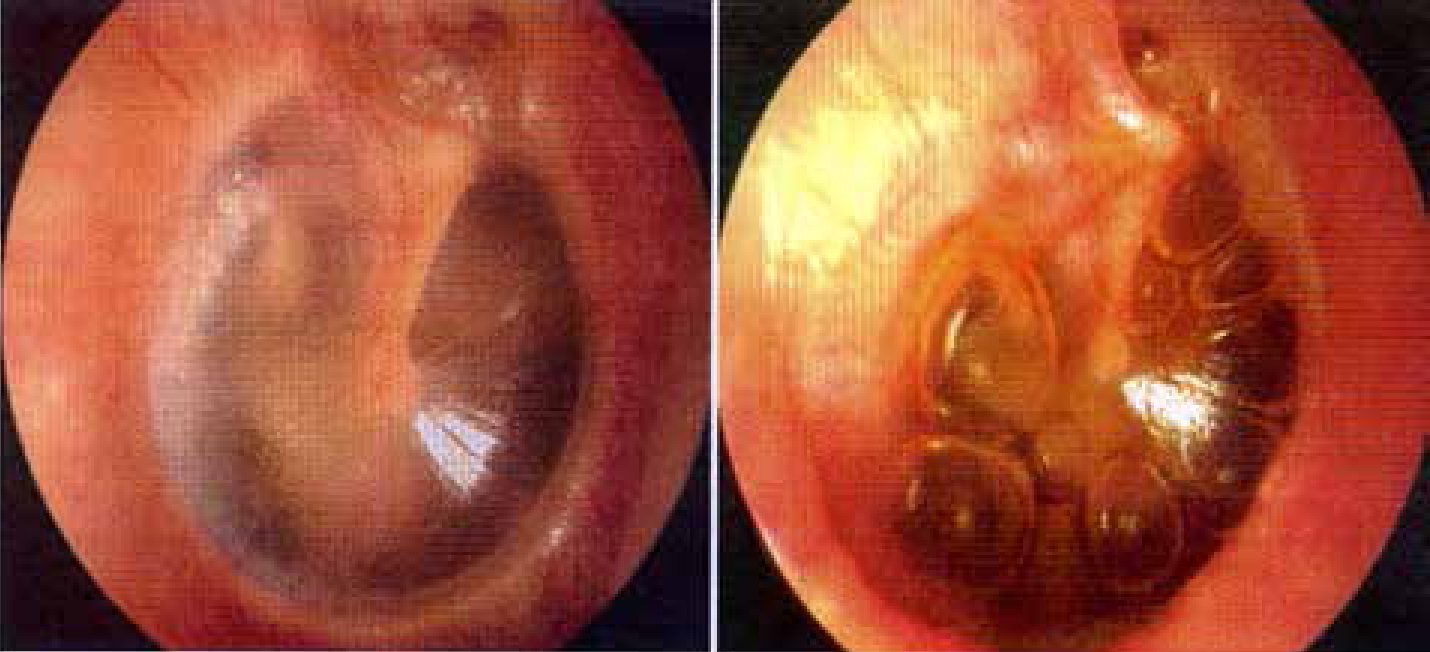
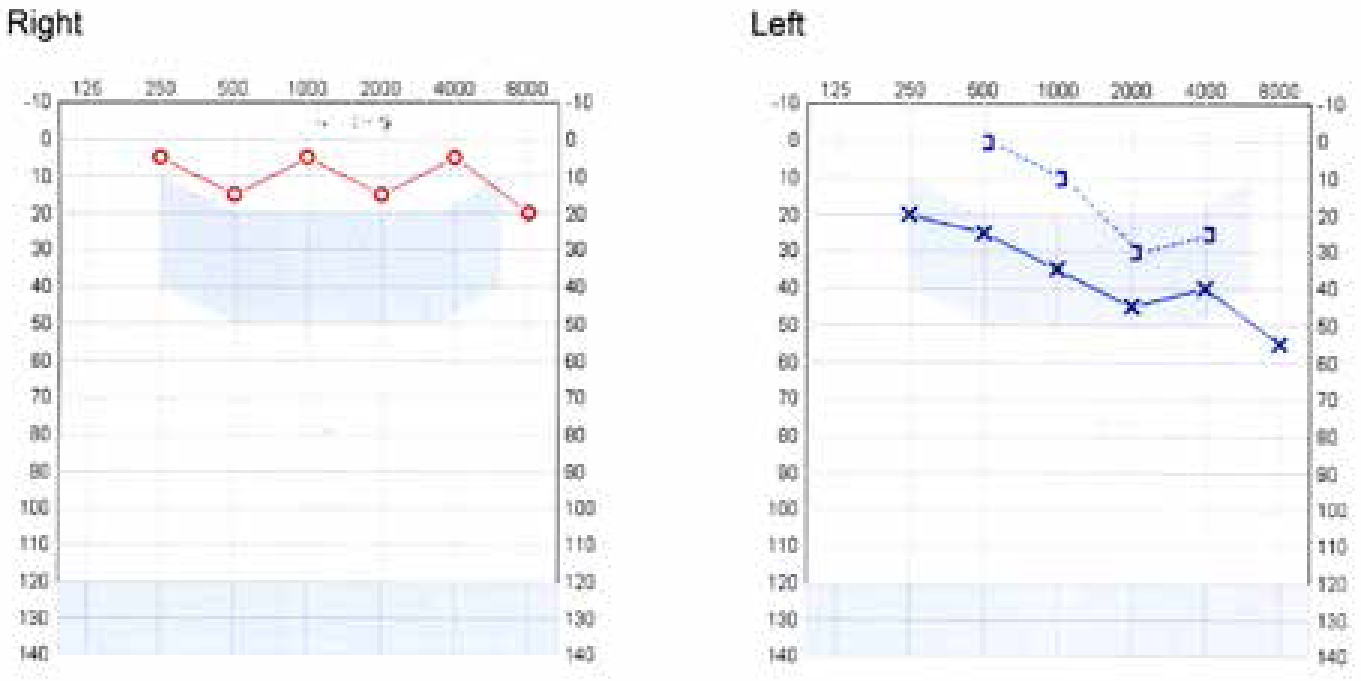
Hearing is linked to speech development and hearing loss is most commonly related to otitis media with effusion (OME) (Figure 1). It has been estimated that 97% of patients with a cleft palate will suffer from a degree of hearing loss. In the non-cleft population this is normally 20%.3 Otitis media occurs in children with clefts because the palatal aponeurosis does not function normally to open the eustachian tube (via the tendon from the tensor veli palatini muscle, which attaches to the membranous portion of the eustachian tube and passes around the pterygoid hamulus). A diagnosis of otitis media is made by testing conductive hearing loss (Figure 2). Children with persistent otitis media require myringotomy and insertion of ventilation tubes (grommets). Early insertion is routine in some centres, although there is insufficient evidence to justify this.4 Any dental treatment that is needed at this stage can be carried out during the same anaesthetic and therefore liaison between the primary care dentist and ENT surgeon may be required. Any concerns about otitis media during the subsequent years of growth and development will trigger an audiological assessment.
Figure 1. Normal tympanic membrane (left) and otitis media with effusion (right). (Reproduced from Farboud A, Skinner R, Pratap R. Otitis media with effusion (“glue ear”). Br Med J 2011; 343: d3770 with permission from BMJ Publishing Group Ltd.)Figure 2. Audiogram showing mild-moderate hearing loss in the left ear due to OME.
Speech development and quality is linked not only to hearing but also to cognitive development and, despite early intervention, not all children develop optimal speech. For some children, signs of global delay will have become evident by this stage and an overall multi-agency education package, including both cognitive and speech and language development skills, will be provided.
Dental care
Children with clefts are encouraged to establish good dental health in the mixed dentition and most multidisciplinary teams provide additional preventive dental care, particularly for patients who are not regular attenders with a primary care dentist. This can have advantages for other family members as well. Early loss of deciduous teeth due to caries complicates any subsequent orthodontic treatment resulting from loss of arch length.2 It is therefore preferable to restore deciduous molars with stainless steel crowns using the ‘Hall’ technique than to have them extracted. Any deciduous maxillary incisor tooth that fails to develop in the region of the cleft should be noted and the parents informed that there is a high chance that the permanent successor will be absent as well.
Cleft clinic
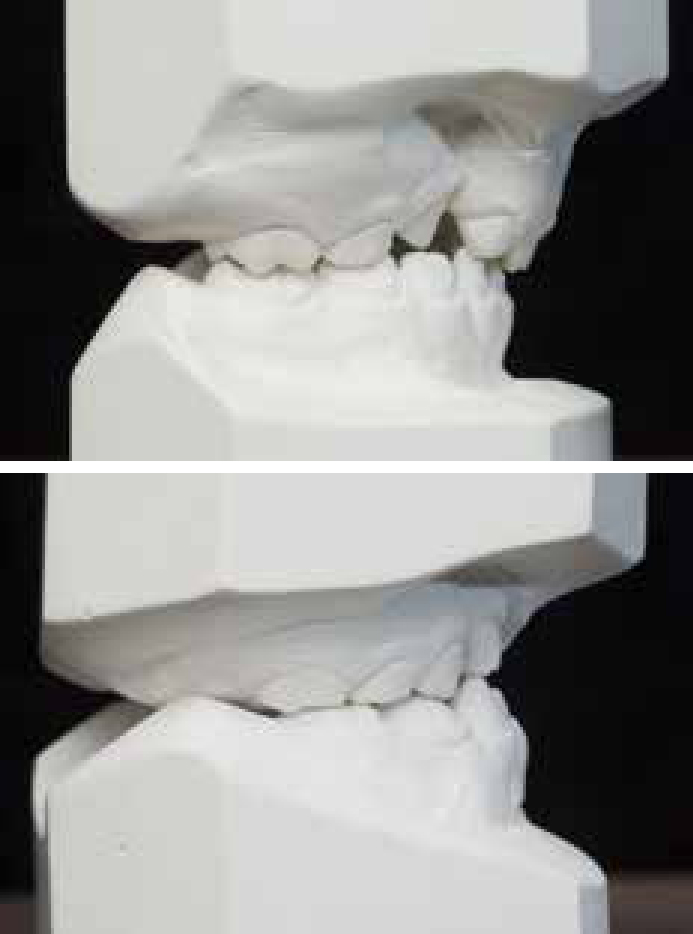
Age 5 is a key milestone for the child with a cleft. The child will attend the multidisciplinary cleft clinic for an assessment of his/her overall progress and the assessments detailed in Table 3 of Part 1 will measure the outcome of the primary surgery (Figure 3), evaluate speech and language development, audiological status and determine any necessary dental care. A clinical psychological assessment and an evaluation of parent satisfaction is undertaken by many teams at this time. Other assessments may be necessary, depending on the clinical needs of the individual child. Any revision surgery should be complete before the child starts school. This may involve grommets (re-insertion), lip scar revision, repair of any oro-nasal fistula (see below).
Figure 3. Models showing (a) good and (b) poor outcomes as judged using the 5-year index.
Age 5 to 7 years
Speech and hearing
Children with a cleft palate and/or velopharyngeal insufficiency (VPI) [malfunctioning resulting in imperfect closure of the velopharyngeal apparatus] are at risk of articulatory problems, nasal emission, hypernasal resonance and hearing problems, all having an impact on intelligibility. An assessment by a specialist speech and language therapist will identify the nature and extent of these problems with a management plan being determined for each patient. Most parents recognize that improved communication has a positive impact on literacy, social skills, peer relationships, self-confidence and behaviour. As these are paramount in educational achievement, contact will be made by the link Speech and Language Therapist with the school class teacher.
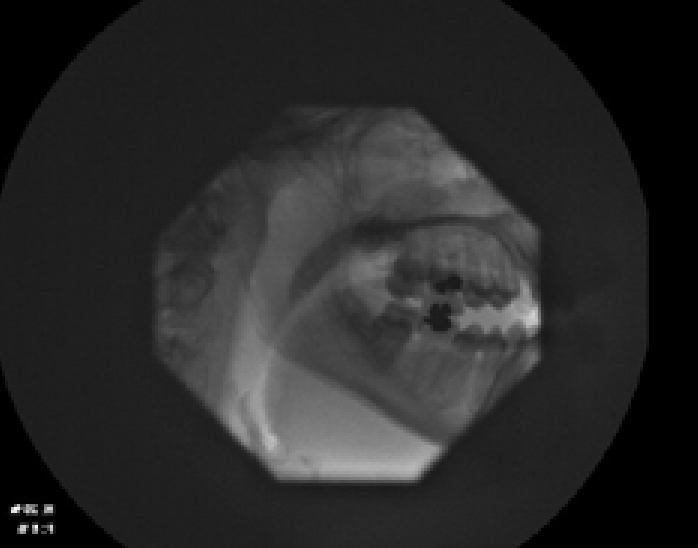
During the early school years, velopharyngeal insufficiency (VPI) may become apparent in children where the soft palate fails to make contact with the posterior pharyngeal wall. This frequently manifests as hypernasality and, on occasions, as poor intelligibility of speech. The investigation of VPI requires a lateral videofluoroscopy examination (Figure 4) and, depending on the maturity of the child, nasendoscopy can help visualize the location of the problem. Where VPI is diagnosed as a consequence of a soft-palate/pharyngeal structural anomaly, consideration will be given to a palate re-repair or a pharyngoplasty, either involving further soft palate surgery to increase the mobility of the soft palate through a re-orientation of the soft palate muscles or, alternatively, using a pharyngeal flap (a superiorly based midline pharyngeal flap producing two portals) or sphincter technique (Hynes/orticochoea) to increase the bulk of the pharyngeal wall.
Figure 4. Lateral videofluoroscopy.
Where hearing impairment impacts on educational achievement and social contact, conventional ‘Behind the Ear’ (BTE), mini BTE or other types of hearing aids will be prescribed and, in cases of profound deafness, the child may require additional support in school through the ‘Teacher of the Deaf’ programme.
As children grow, fistulae that have previously caused little trouble can enlarge. Should a fistula be affecting speech (hypernasality and nasal emission) or occasional regurgitation of fluid/food into the nose, surgical closure is indicated (Figure 5). Whilst this can be done at the same time as the alveolar bone graft for children with an alveolar cleft (as this also allows the nasal floor to be repaired) using local flaps, other surgical techniques can be considered for a persistent fistula, such as a buccal or a tongue flap.
Figure 5. Fistula requiring surgical closure.
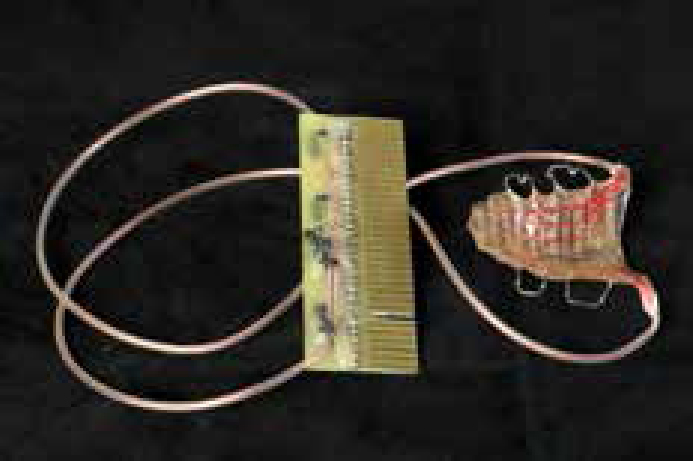
Articulation disorders are similarly challenging speech problems and occur among patients both with and without clefts. For patients with clefts, articulation disorders can be difficult to resolve as errors in tongue placement can be related to learned poor speech patterns, tissue deficiency in the cleft region, abnormal skeletal relationships and malocclusion among others. These can all reduce the overall intelligibility of speech. Articulation disorders can be diagnosed using electropalatography (EPG), which provides real time visual feedback about tongue to palate contact for the patient. The appliance (Figure 6) is constructed in a similar manner to an orthodontic removable appliance, with the electrodes and associated wires being incorporated in the acrylic. Patients wear the appliance during their speech therapy sessions and the therapist can demonstrate the ideal tongue position using an appliance first. In some regions, patients can borrow a portable unit to use at home with parental support.
Figure 6. Electropalatography appliance.
Dental care
The primary care dentist should ensure that the dentition is caries free and oral hygiene is excellent. Dietary counselling to prevent caries and erosion should be offered at each appointment. For children considered ‘high risk’ of further caries, toothpaste with 1450 ppm fluoride should be used and permanent molars fissure sealed as they erupt (in areas where tap water is non-fluoridated). The eruption of the permanent incisors should be monitored. Any suspicion of non-eruption of teeth should be investigated by palpation and supplemented by an intra-oral radiograph where necessary. For children with a cleft involving the alveolus, the maxillary permanent central incisor may be rotated as it erupts, sometimes as much as 90 degrees (Figure 7). Parents should be advised that this cannot be corrected until after bone grafting has been carried out, as derotating the tooth into an area of bone deficiency will compromise the vitality of the tooth. On occasions, areas of hypoplasia affect the labial surface. The incisor relationship should be monitored and, where incisor crossbites are noted, contact should be made with the orthodontist on the multidisciplinary team for advice and treatment, as necessary.
Figure 7. Rotated central incisor in a child with a cleft of the lip and alveolus before alveolar bone grafting.
Orthodontic care
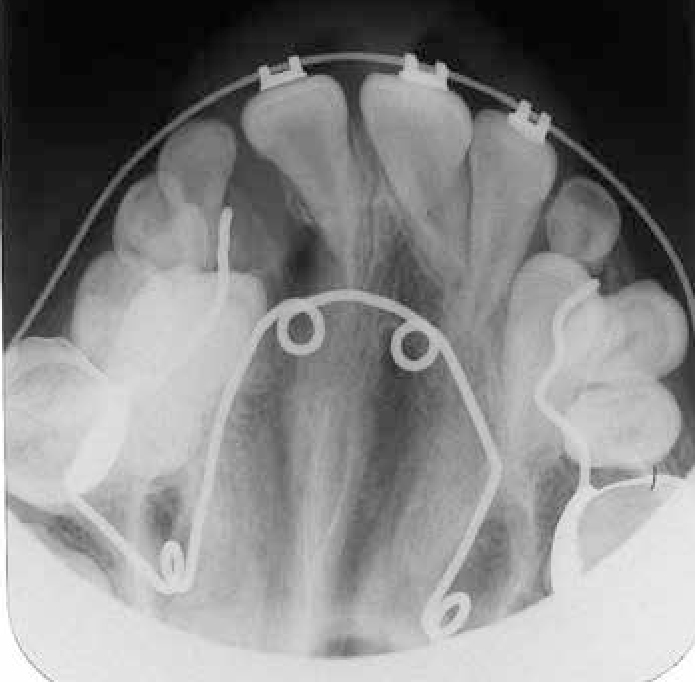
Permanent central incisor crossbites are generally corrected with a standard removable appliance, whilst for patients requiring a bone graft, incisor proclination can be incorporated, along with later pre-bone graft orthodontic treatment with a fixed appliance (Figure 8) to mimimize the overall burden of care.
Figure 8. Fixed appliance to correct incisor crossbites during pre-alveolar bone grafting orthodontic treatment radiograph. (The quad-helix for maxillary expansion can be clearly seen.)
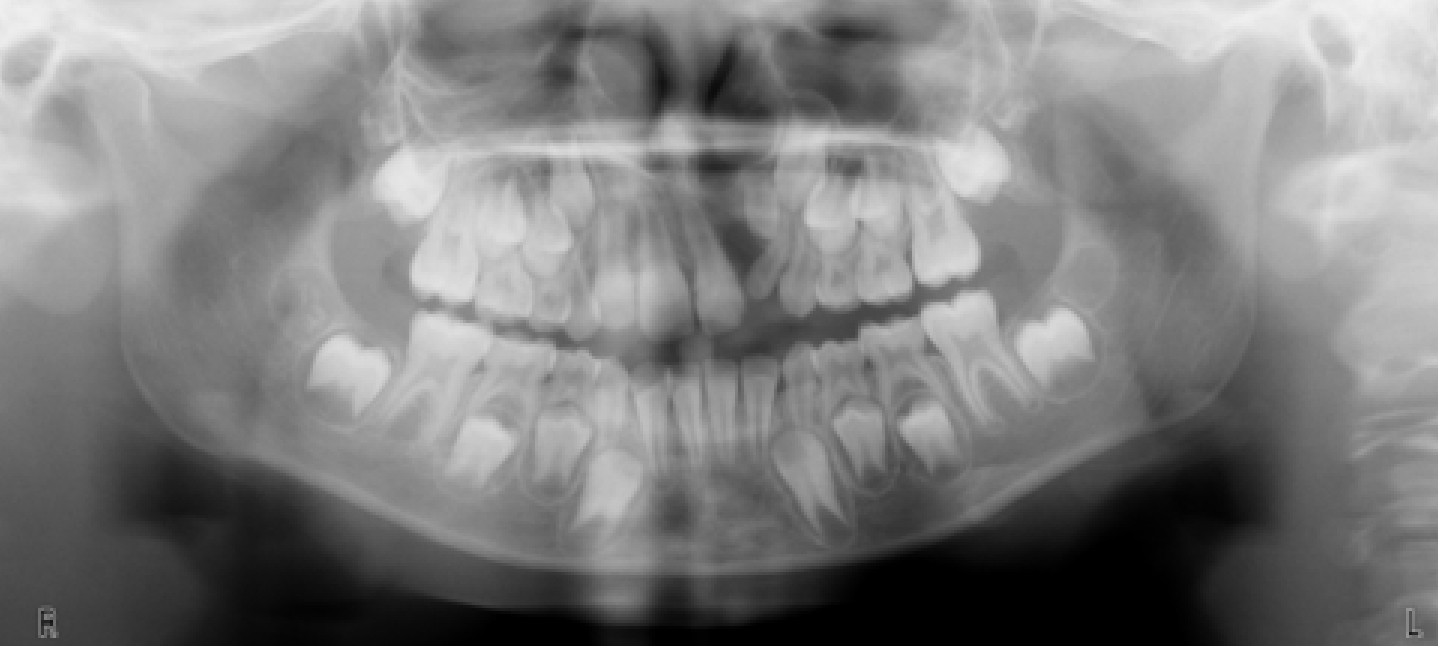
Where the cleft involves the alveolus, the presence or absence of the permanent maxillary lateral incisor and the developmental stage of the rest of the dentition is important in determining the ideal stage for the alveolar bone graft to be carried out. Therefore, at age 7, all children with an alveolar cleft should have a panoramic radiograph taken to assess the possibility of a viable lateral incisor in the line of the cleft (Figure 9). Where this is absent, consideration can be given to an early alveolar bone graft in order to promote early eruption of the permanent canine into the graft site. This may avoid the need for a bridge/implant-retained crown to replace the missing lateral incisor in adulthood. Where the permanent maxillary lateral incisor is present, the stage of development of the maxillary permanent canine can be assessed with a view to carrying out the bone graft when the canine root is approximately half to two-thirds formed. This requires a degree of forward planning and the degree of development of the other permanent teeth will act as a clinical guide. Supernumerary and supplemental teeth in the area of the alveolar defect, along with erupted teeth that may affect wound closure, should be removed around three months before the bone graft surgery (Figure 10).
Figure 9. Panoramic radiograph showing a developmentally absent permanent maxillary lateral incisor, presence of a supernumerary tooth in the cleft and the permanent maxillary canine root starting to develop.Figure 10. Supernumerary teeth (should be removed 3 months pre-alveolar bone graft).
Psychology
Young children can unwittingly pose unwelcome questions about lip scars, speech, hearing and other problems to children with clefts. Others may deliberately tease children with clefts who have yet to develop the cognitive skills to deal with such unwanted attention. As a result, the clinical psychologist and other members of the multidisciplinary team may need to provide support for the child, parents and school to help manage such problems to avoid them escalating.
Age 8 to 10 years
Alveolar bone graft
An alveolar bone graft is required for most children where the cleft affects the alveolus and is considered by most cleft teams as the final ‘compulsory’ surgical procedure. It has the following objectives:
Eruption of the canine into sound alveolar bone;
Provision of bony support for teeth on either side of the cleft;
Improved stability of cleft segments, especially the premaxilla in BCLP cases;
Facilitation of fistula closure;
To obviate/minimize the need for prosthetic replacement of teeth in the line of the cleft;
Improved contour of, and support for, the alar base.
For children with minor alveolar clefts, which can be detected by digital palpation as an alveolar notch and confirmed by an intra-oral radiograph, grafting is unlikely to be required. Alveolar bone grafting is a time critical procedure and, as detailed above, is governed by dental development. Grafts undertaken before canine eruption have good success rates5 and, therefore, most cleft teams plan to carry out surgery by the age of 11 years, where possible.
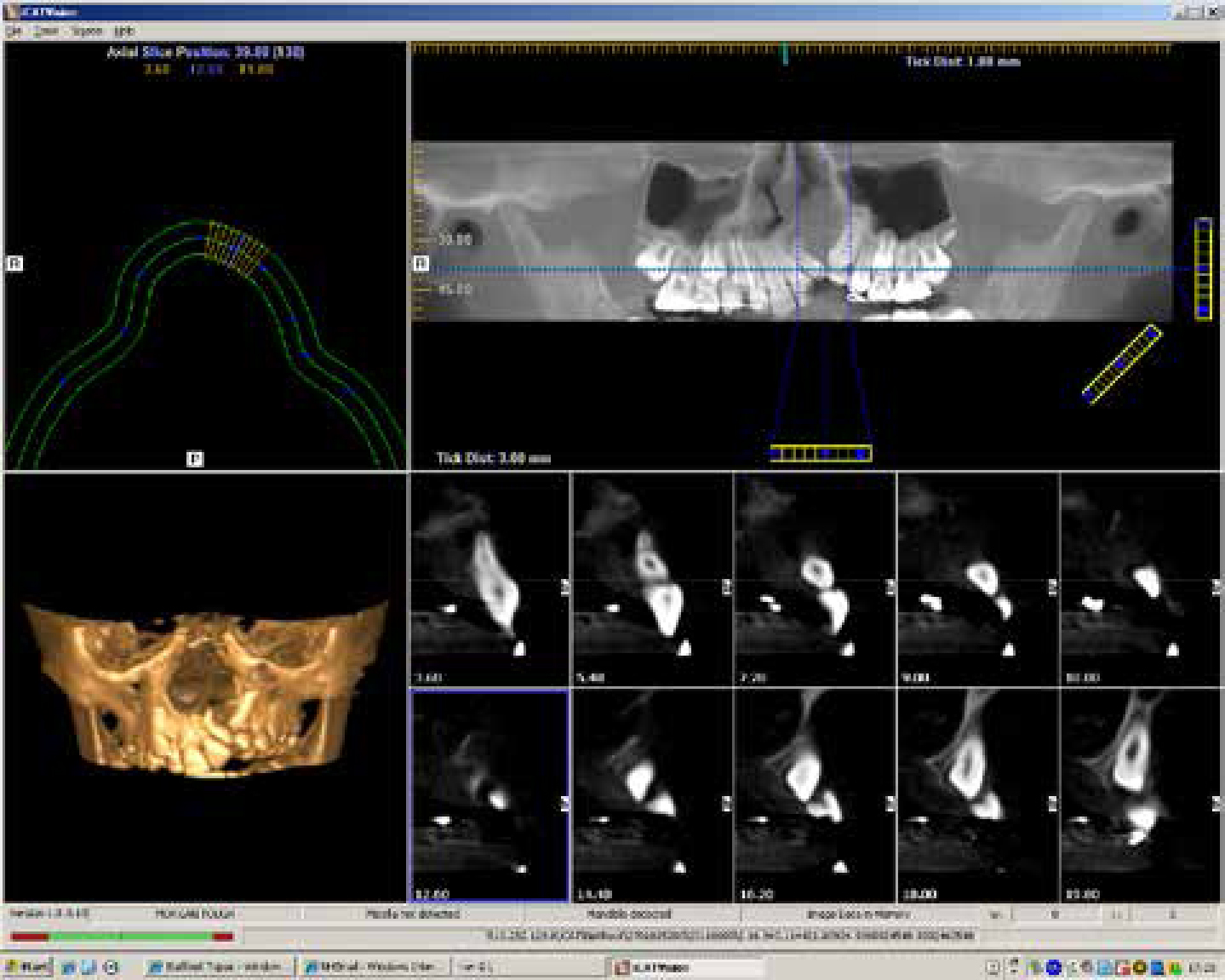
In preparation for the alveolar bone graft, the orthodontist and cleft surgeon will determine the need for pre-bone graft expansion. This is needed in cases where there has been collapse of the maxillary segments into the cleft manifesting as a full tooth crossbite. Whilst arch collapse reduces the size of the defect, the amount of bone that can be grafted is reduced and the likelihood of success is commensurately reduced. Maxillary expansion is traditionally undertaken in the UK with a quad-helix appliance to expand the alveolar defect area, whilst in other areas of the world, rapid maxillary expansion is favoured. Immediately before surgery, the size of the alveolar defect is assessed. In some units, an occlusal radiograph is used (Figure 10), whilst in others, cone-beam CT and 3D volumetric measurement is becoming standard practice (Figure 11). The primary care dentist has an important role to ensure that the patient has excellent oral hygiene and no unrestored carious lesions at the time of surgery. Any intra-oral reservoir of micro-organisms will result in poor wound healing and any periodontopathic micro-organisms can destroy the grafted bone before it has integrated.
Bone is usually harvested from the iliac crest and the nasal mucosa is used to repair the floor of the nose. The intra-oral mucosal flaps are designed to avoid any communication between the surgical site and the oral cavity and, at the same time, promote healthy periodontal tissues. Post-operatively, most patients find the hip donor site more painful than the alveolar wound. Patients are encouraged to become mobile as soon as possible and are usually discharged in around 3 to 5 days. Post-operatively, it is crucial that oral care is maintained, and for toothbrushing to be supplemented with an antimicrobial mouthwash. Bone healing is assessed on an occlusal radiograph taken 3 to 6 months after surgery using the Kindelan Index, a 4-point scale depending on quantity of bone increase between pre-and post-operative radiographs.6Figure 12 shows an example of a good result and Figure 13 shows an example of a fixed retainer used to maintain arch expansion. The overall success of bone grafting cannot be determined until the canine is fully erupted and is done using the Bergland Index, a 4 point scale grading the height of the interdental septum.7 Success rates of alveolar bone grafting in the UK are good, with 85% of cases being successful in a recent UK national study.8
Figure 11. Cone-Beam CT scan to determine 3D nature of alveolar defect.Figure 12. Post-operative occlusal radiograph showing excellent bone integration.Figure 13. Fixed retainer to maintain arch expansion.
An orthodontic assessment to determine the future orthodontic requirement is normally undertaken at this stage.
Dental care
The primary care dentist should continue to offer preventive dental care and encourage the children to take responsibility for their own dental health as they progress through the mixed dentition and mature.9 Liaison with the paediatric dentist on the cleft team may be necessary where there are difficulties resulting from lack of co-operation/missed appointment for the provision of preventive/restorative care, particularly around the time of alveolar bone grafting.
The third part of this article will detail the care of patients with clefts from the age of 10 until adulthood.