Araújo MG, Lindhe J Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J Clin Periodontol. 2005; 32:212-218 https://doi.org/10.1111/j.1600-051X.2005.00642.x
Kan JY, Rungcharassaeng K, Sclar A, Lozada JL Effects of the facial osseous defect morphology on gingival dynamics after immediate tooth replacement and guided bone regeneration: 1-year results. J Oral Maxillofac Surg. 2007; 65:(7)13-19 https://doi.org/10.1016/j.joms.2007.04.006
Isola G, Nucera R, Damonte S Implant site changes in three different clinical approaches: orthodontic extrusion, regenerative surgery and spontaneous healing after extraction: a systematic review. J Clin Med. 2022; 11 https://doi.org/10.3390/jcm11216347
Salama H, Salama M The role of orthodontic extrusive remodeling in the enhancement of soft and hard tissue profiles prior to implant placement: a systematic approach to the management of extraction site defects. Int J Periodontics Restorative Dent. 1993; 13:312-333
González-Martín O, Solano-Hernandez B, Torres Muñoz A Orthodontic extrusion: guidelines for contemporary clinical practice. Int J Periodontics Restorative Dent. 2020; 40:667-676 https://doi.org/10.11607/prd.4789
Reitan K Clinical and histologic observations on tooth movement during and after orthodontic treatment. Am J Orthod. 1967; 53:721-745 https://doi.org/10.1016/0002-9416(67)90118-2
Brown IS The effect of orthodontic therapy on certain types of periodontal defects. I. Clinical findings. J Periodontol. 1973; 44:742-756 https://doi.org/10.1902/jop.1973.44.12.742
Ingber JS Forced eruption. I. A method of treating isolated one and two wall infrabony osseous defects-rationale and case report. J Periodontol. 1974; 45:199-206 https://doi.org/10.1902/jop.1974.45.4.199
Oppenheim A Artificial elongation of teeth. Am J Orthodont Oral Surg. 1940; 26:931-940
Caberlotto M, Gobbo M, Bettio E Combining orthodontic extrusion and guided bone regeneration (GBR) for bone augmentation and implant placement in the aesthetic zone: technical issues and case report. Oral ' Implantology. 2018; XI:(1)24-30
Heithersay GS Combined endodonticorthodontic treatment of transverse root fractures in the region of the alveolar crest. Oral Surg Oral Med Oral Pathol. 1973; 36:404-415 https://doi.org/10.1016/0030-4220(73)90220-x
Pontoriero R, Celenza F, Ricci G, Carnevale G Rapid extrusion with fiber resection: a combined orthodontic-periodontic treatment modality. Int J Periodontics Restorative Dent. 1987; 7:30-43
Korayem M, Flores-Mir C, Nassar U, Olfert K Implant site development by orthodontic extrusion. A systematic review. Angle Orthod. 2008; 78:752-760
Stefanini M, Marzadori M, Aroca S Decision making in root-coverage procedures for the esthetic outcome. Periodontol 2000. 2018; 77:54-64 https://doi.org/10.1111/prd.12205
Elian N, Cho SC, Froum S A simplified socket classification and repair technique. Pract Proced Aesthet Dent. 2007; 19:99-104
Tonetti MS, Jung RE, Avila-Ortiz G Management of the extraction socket and timing of implant placement: consensus report and clinical recommendations of group 3 of the XV European Workshop in Periodontology. J Clin Periodontol. 2019; 46:183-194 https://doi.org/10.1111/jcpe.13131
Alsahhaf A, Att W Orthodontic extrusion for pre-implant site enhancement: principles and clinical guidelines. J Prosthodont Res. 2016; 60:145-155 https://doi.org/10.1016/j.jpor.2016.02.004
Cordaro M, Staderini E, Torsello F Orthodontic extrusion vs. surgical extrusion to rehabilitate severely damaged teeth: a literature review. Int J Environ Res Public Health. 2021; 18 https://doi.org/10.3390/ijerph18189530
A multidisciplinary approach for implant placement in the aesthetic zone: A case report and literature review Maria Costanza Soldini Ramon Pons Federica Bertuzzo Claudio Soldini Dental Update 2025 52:5, 347-352.
Authors
Maria CostanzaSoldini
DDS, MSc, Specialist Periodontist, Studio dentistico SBM, Vicenza, Italy
Achieving an optimal aesthetic outcome with implant-supported crowns in the aesthetic zone remains one of the biggest challenges in implant dentistry. A 34-year-old female patient, with no significant systemic pathology, came to the dental office to receive treatment for an anterior open bite and gingival recession in tooth UL1. This case report demonstrates how a multidisciplinary approach, which includes orthodontic treatment, periodontal plastic surgery, guided bone regeneration, and an implant-supported crown, can effectively restore both function and aesthetics for the patient. Additionally, a narrative review of the literature is presented alongside the case presentation.
CPD/Clinical Relevance:
This case report illustrates a multidisciplinary approach that effectively addresses complex cases in aesthetic dentistry.
Article
Achieving an optimal aesthetic outcome with implant-supported crowns in the aesthetic zone is still one of the greatest challenges in implant dentistry. The result of the implant-supported restoration in the aesthetic zone is demanding since its success depends on its visual integration with the adjacent teeth and soft tissues. Aesthetic outcomes are influenced by multiple surgical and prosthetic factors that must be meticulously managed before tooth extraction. Indeed, after tooth extraction, some dimensional alterations of the alveolar ridge can be expected. The buccal bone tends to resorb, followed by the collapse of soft tissue, thereby aesthetically compromising the restored site.1,2 Consequently, pre- and peri-implant hard and soft tissue management is often required to ensure the long-term success of dental implants.3
Currently, orthodontic extrusion, or forced eruption, is a non-surgical procedure indicated to enhance soft and hard tissue architecture before implant placement.4 This is a noninvasive technique based on the periodontium's ability to respond to the magnitude and direction of the tooth movement applied.5 Indeed, during active orthodontic treatment, it is possible to differentiate between pressure and tension forces.6 At the bone level, pressure forces typically provoke a localized physiological response, leading to increased osteoclast activity and subsequent bone resorption. Conversely, tension forces stimulate bone apposition through enhanced osteoblastic activity.6 Careful case selection is crucial when considering this technique. It should be avoided in cases of ankylosis or hypercementosis, as the additional load may result in intrusion of the anchoring teeth. Other contraindications include vertical root fractures, close proximity to the roots of adjacent teeth, severe internal or external root resorption, short root length, untreated periodontitis or peri-apical disease, and situations where it may expose the furcation in multirooted teeth.5
Extrusive tooth movements have the potential to induce the coronal displacement of surrounding bone7,8 and soft tissue by supraphysiological elongation of gingival collagen fibre bundles in a vertical direction.9 As a result, extrusive tooth movements can cause coronal displacement of the surrounding bone, which may help address significant anatomical deficiencies before implant placement.4,5 However, in cases of severe vertical bone loss, additional intervention may be required. In such situations, a multidisciplinary approach that integrates orthodontic extrusion with guided bone regeneration may be crucial.10
This article presents a clinical case in which a multidisciplinary approach, involving orthodontic extrusion, periodontal plastic surgery and guided bone regeneration were involved in the rehabilitation of a patient through the placement of a single dental implant in an aesthetic zone.
Case presentation
A 34-year-old female patient presented for dental treatment with the chief complaint of an anterior open bite (AOB) and gingival recession at UL1. The patient reported no significant medical history.
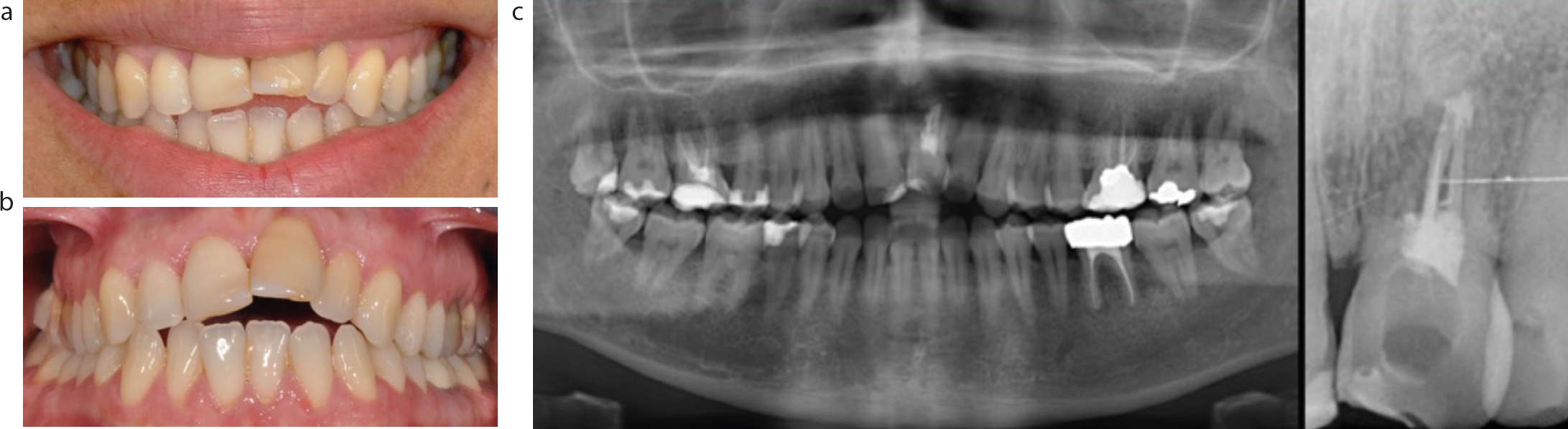
The dental team performed a clinical and radiographic examination of the patient (Figure 1). An AOB was diagnosed, with external root resorption associated with UL1. The prognosis for UL1 was judged to be poor, making its extraction mandatory. Periodontal analysis revealed a probing depth (PPD) of 8 mm on the mesial aspect of UL1; all other teeth exhibited a PPD of less than 4 mm. Bleeding on probing was observed only mesial to UR8 and UL8. Professional supragingival instrumentation was carried out, and oral hygiene instruction was provided.
Figure 1.
(a–c) Clinical and radiographic examination of the patient.
Based on the information gathered, the proposed treatment plan included orthodontic treatment for the AOB and a dental implant to restore UL1. Orthopantomograms, teleradiographs and dental casts were collected to enable a cephalometric analysis for evaluation by the orthodontist. Following a thorough multidisciplinary examination by an orthodontist and a periodontist, orthodontic treatment of the AOB was recommended, with the concomitant extrusion of UL1 to facilitate the surgical phases prior to the dental implant placement. Indeed, periodontal plastic surgery and guided bone regeneration (GBR) procedures were planned to improve the soft tissue aesthetic and bone volume. The patient was informed about the treatment procedures, and at least 1 week passed between the provision of this information and the signing of the informed consent form.
Orthodontic treatment
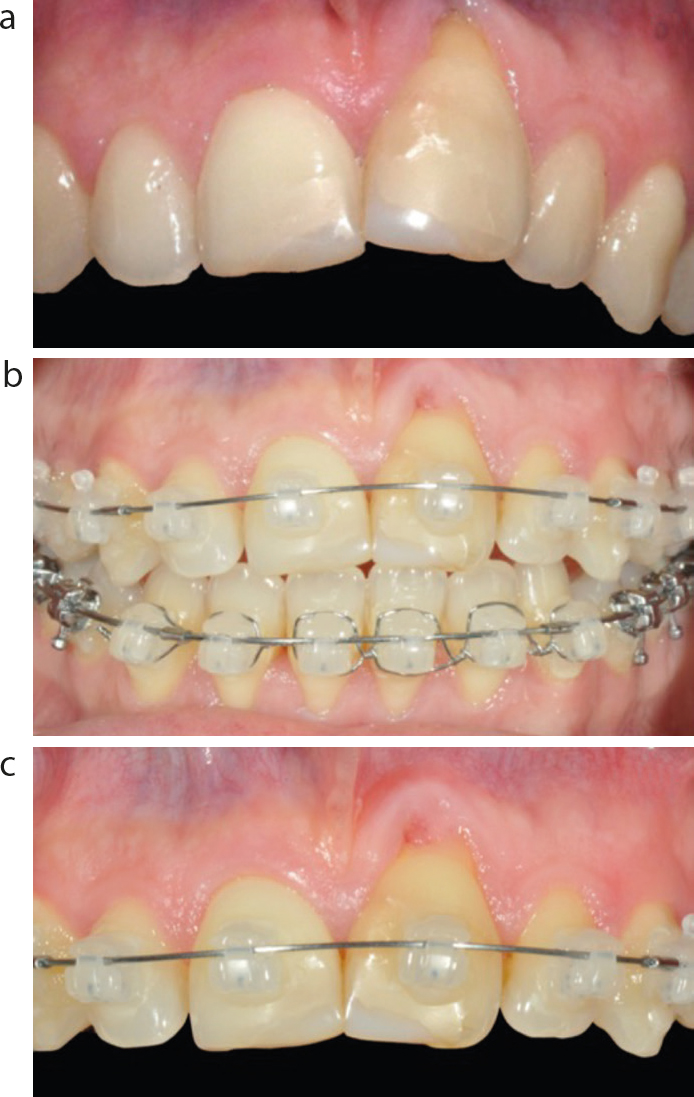
After the periodontal phase (Figure 2a), a full ceramic fixed orthodontic appliance (upper and lower) was installed for orthodontic correction with dental compensation for 24 months. The bracket on the resorbed incisor was positioned apically and a 0.14” copper–nickel–titanium wire was applied for the first 3 months (Figure 2b,c). For extrusion of UL1, activations were made every 4 weeks for 24 weeks, with a total of six activations.
Figure 2.
(a–c) Placement of a full ceramic fixed orthodontic appliance.
Orthodontic extrusion was carried out to move the root of the tooth in a coronal direction, towards the occlusal plane. It was performed to change tooth position or induce therapeutic changes in the surrounding alveolar bone and soft tissue
Mucogingival surgery
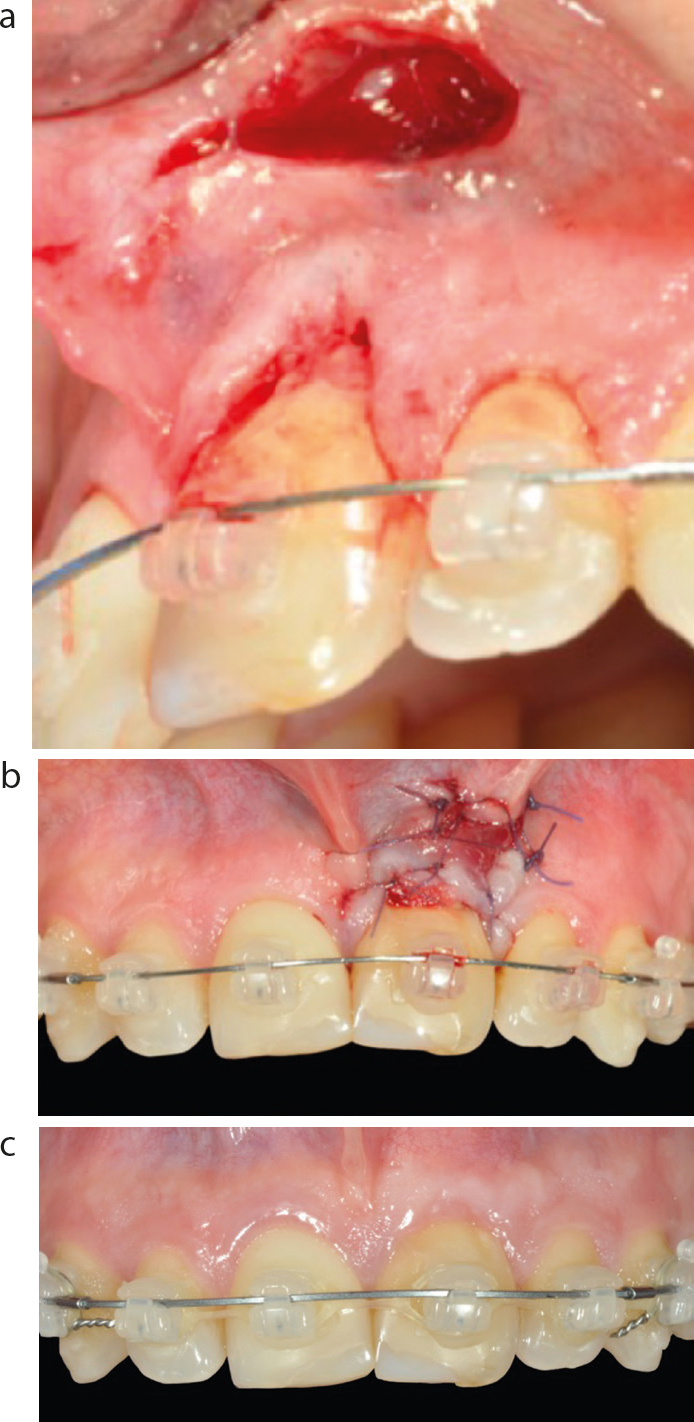
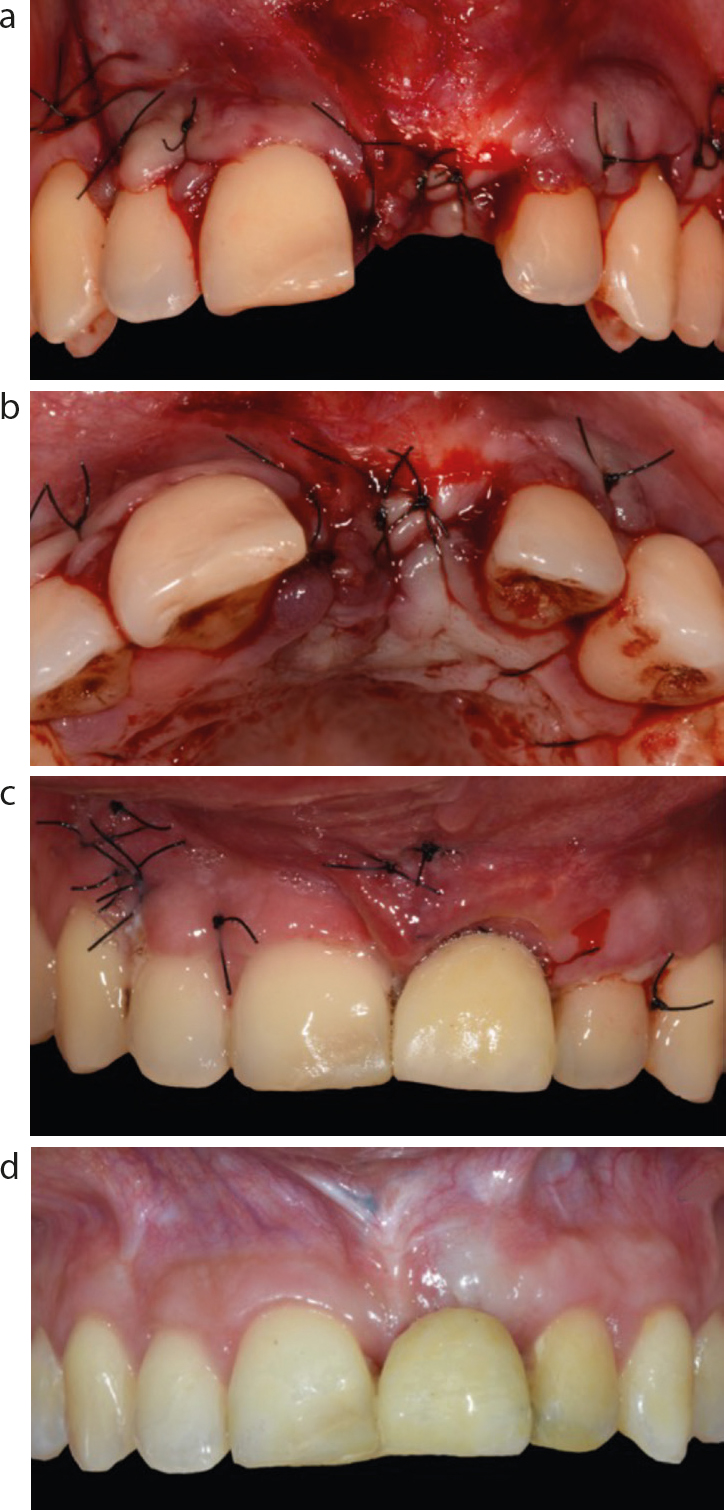
At the end of the extrusion procedure, a mucogingival procedure was performed to improve the soft tissue aesthetic of UL1. A horizontal vestibular access incision was made apically to the mucogingival junction (MGJ) of UL1. The incision was extended down to the bone to create a subperiosteal tunnel, allowing exposure of the vestibular bone plate and root dehiscence.
The tunnel elevation was carried out apically to the base of the vestibule and coronally to the gingival margin and interproximal papillae. This technique allowed for tension-free detachment and facilitated the coronal advancement of the flap (Figure 3a). Then, a free connective tissue graft was harvested from the palatal area at the level of teeth UR4–UR6}, the donor area was sutured with a polyamide 5-0 suture (Supramid, B Braun, Melsungen AG, Germany). The graft was carefully de-epithelialized and inserted in the subperiosteal tunnel. To stabilize the gingival margin, sling sutures with 5-0 polyglactin sutures (Vicryl, Ethicon, Johnson & Johnson Medical Spa, Pomezia, Italy) were employed, while the access incision was secured with simple sutures (Figure 3b).
Figure 3.
(a–c) Mucogingival surgery and 6 weeks follow-up.
After 6 weeks, the gingival margin of UL1 was observed to be completely level with that of the contralateral tooth (Figure 3c).
Guided bone regeneration
Once the orthodontic treatment was completed, a cone beam computed tomography (CBCT) scan was performed to evaluate the feasibility of implant rehabilitation. The CBCT analysis revealed insufficient bone volume to place a dental implant, thus a guided bone regeneration (GBR) surgery was scheduled, and impressions for a provisional Maryland bridge were taken.
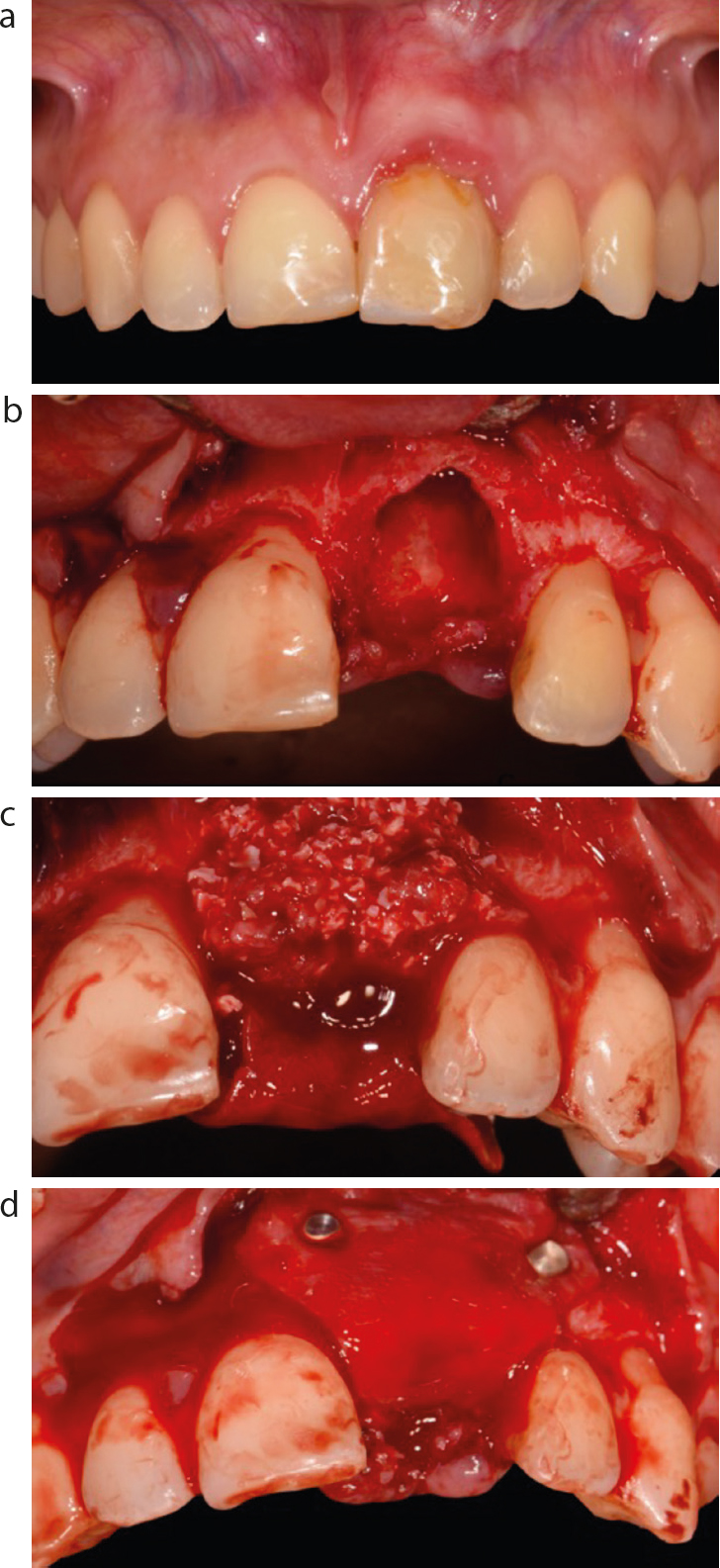
On the day of the surgery, local anaesthesia comprising articaine 4% with 1:100,000 epinephrine was administered. Papilla preservation incisions were made from the midpoint of UR3 to the distal of UL3, where vertical releasing incisions were made. UL1 was extracted, and granulation tissue was meticulously removed (Figure 4a). Then, the palatal flap of UL1 was gently tunnelled to secure a collagen-resorbable barrier (Bio-Gide, Geistlich, Wolhusen, Switzerland) with a pin in the palatal bone. Then, a mixture of 50% autogenous bone harvested from the mandibular ramus with the use of a bone scraper (Safescraper Curve TWIST, META, Reggio Emilia, Italy) and 50% inorganic bovine bone (Bio-Oss, Geistlich, Wolhusen, Switzerland) was placed in the recipient site (Figure 4b). The occlusal portion of the graft was then covered with the collagen-resorbable barrier pulled from the palatal side and blocked on the bone with two buccal pins (Figure 4c).
Figure 4.
(a–d) Guided bone regeneration procedure.
Subsequently, periosteal incisions were made to mobilize the buccal flap. The flap was repositioned and secured using simple and horizontal sutures with a 5-0 polyamide suture (Supramid) (Figure 5a,b). Finally, the metal-reinforced laboratory-fabricated Maryland bridge was cemented with adhesive cement (Variolink Ivoclar Vivadent Naturno (BZ), Italy) at the lingual aspect of the teeth UR1 and UL3 (Figure 5c). Amoxicillin 875 mg + clavulanic acid 125 mg (Augmentin, GlaxoSmithKline, Verona, Italy) was prescribed to be taken twice daily for 7 days. The patient was instructed to rinse with 0.12% chlorhexidine solution twice daily for 14 days post-surgery. As a painkiller, 600 mg ibuprofen was prescribed to be taken up to four times daily for 7 days after surgery if needed.
Figure 5.
(a–d) Sutures after GBR procedure and temporary restoration using a Maryland bridge.
Uneventful healing was observed at the time of suture removal. After 6 months, the patient was scheduled for a CBCT, and the dental implant placement was planned (Figure 5d).
Implant surgery and prosthesis delivery
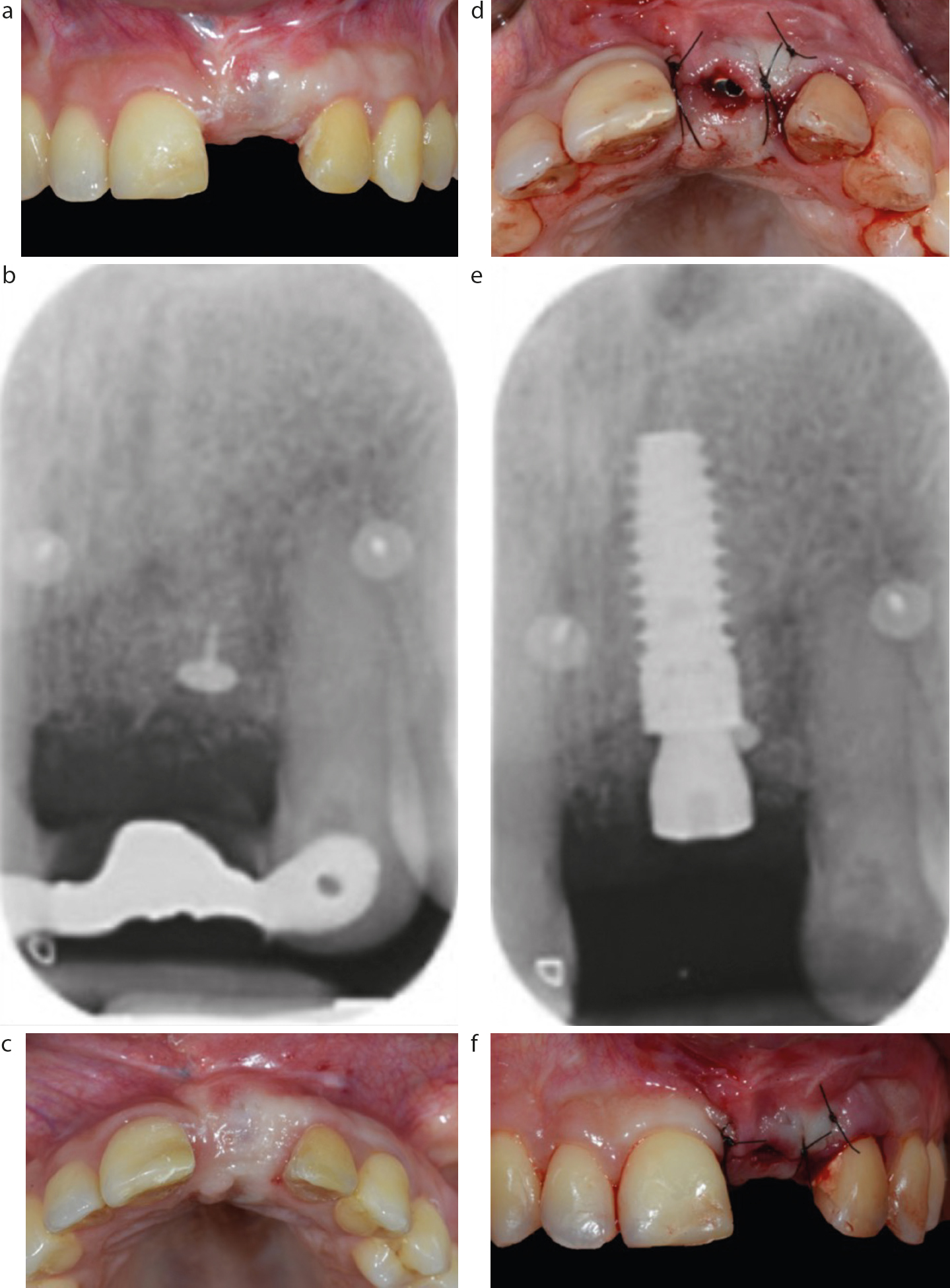
The patient was premedicated one day before surgery with 1 gram of amoxicillin every 12 hours, followed by 1 gram to be taken twice daily for 6 days following surgery. On the day of the surgery (Figure 6a–c), the Maryland bridge was removed and local anaesthesia comprising articaine 4% with 1:100,000 epinephrine was administered. One dental implant with a moderate rough surface (OGI, surface) of 4 mm diameter and 12 mm length was placed in position UL1 (CLC Conic, CLC Scientific, Vicenza, Italy). In the apico-coronal dimension, the implant shoulder was positioned 2 mm subcrestally, apical to the cemento-enamel junction of the adjacent tooth. The insertion torque of the implant at the time of placement was 35 Ncm, a healing cap was placed (CLC Scientific) (Figure 6d,f). The flap was sutured with a 5-0 polyamide suture (Supramid) (Figure 6e). Finally, the metal-reinforced laboratory-fabricated Maryland bridge was cemented at the lingual aspect of UR1 and UL3.
Figure 6. Clinical and radiographic situation (a–c) pre and (d–f) immediately post implant placement.
The patient was instructed to rinse with 0.12% chlorhexidine solution twice a day for 14 days post-surgery. As a painkiller, 600 mg of ibuprofen was prescribed to be taken up to four times daily for 7 days after surgery, if required.
At 16 weeks post-surgery, the Maryland bridge was removed, and analogue impressions were taken to deliver the provisional restoration (Figure 7a).
Figure 7.
(a,b) 16 weeks after implant surgery and screwed provisional restoration delivery.
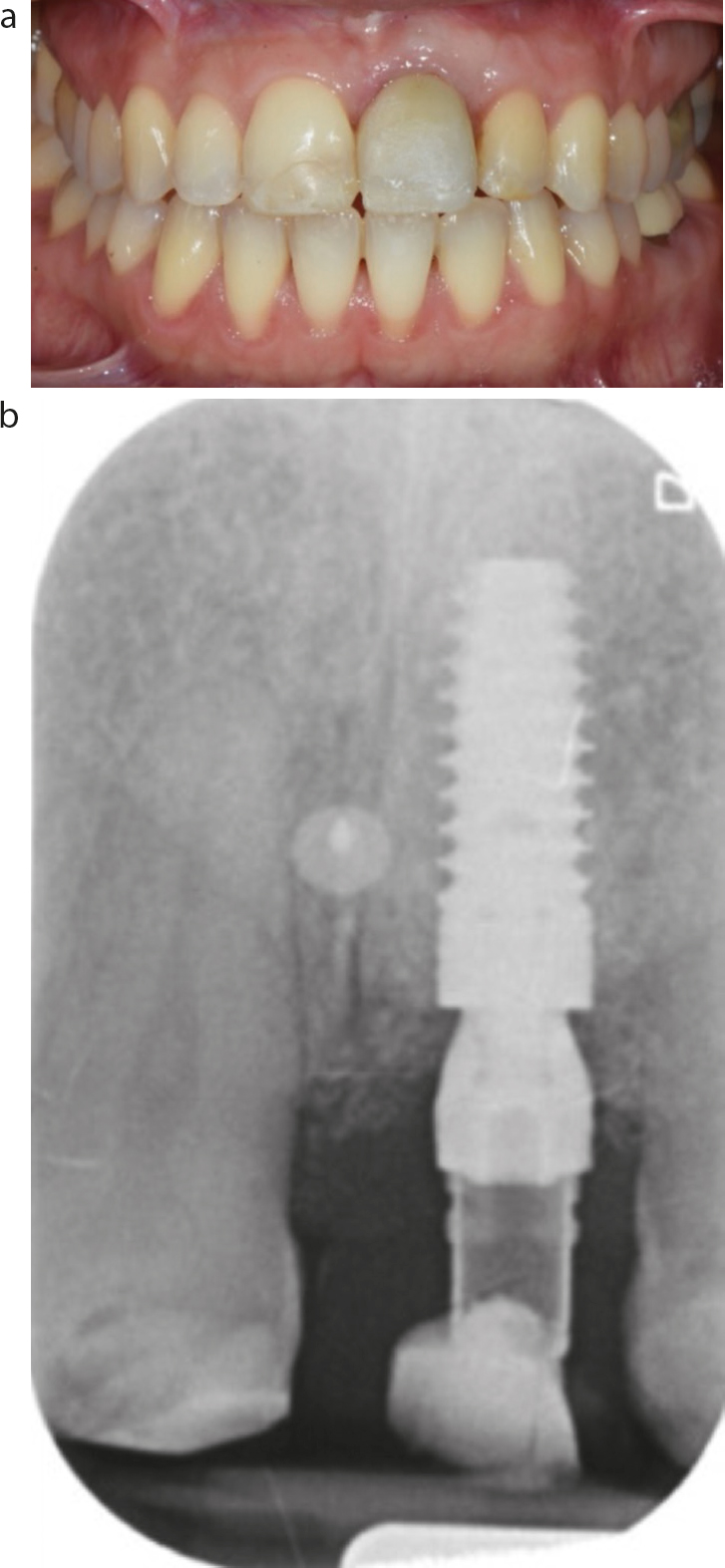
After 12 weeks, the final single metal–ceramic crown was delivered. From the baseline situation (Figure 8a,b), UL1 was successfully rehabilitated (Figure 8c,d).
Figure 8.
(a,b) Baseline and (c,d) final follow-up with the definitive metal-ceramic crown.
Discussion
The use of orthodontic extrusion (OE) for therapeutic purposes beyond the orthodontic alignment was first proposed by Heithersay in 1973. His pioneering study explored the feasibility of restoring subgingival root fractures in endodontically treated teeth by orthodontically repositioning the remaining root structure to a more coronal position.11 After that, several authors proposed different protocols for OE. Pontoriero et al introduced the term ‘rapid extrusion’ that was accompanied by fibre resection,12 while Malmgren et al described the use of rapid OE without the fibrotomy.13 Subsequently, Salama and Salama introduced the term ‘orthodontic extraction’ to describe the use of OE to induce changes in the surrounding alveolar bone and soft tissue, creating a more favourable environment for implant placement.4 Even if in their original protocol no information was provided about the orthodontic forces that need to be applied, it is generally acknowledged that to achieve a tooth extrusion (i.e. orthodontic extraction) with traction of both gingival tissues and alveolar bone, light forces are recommended.
Specifically, forces of 15 g applied to thin roots and of 60 g applied to molars are enough for a slow extrusion.14 However, the force applied will depend on the patient's physiological response, requiring dynamic adjustments during periodic visits to achieve the desired outcome without complications.5 This clinical protocol is also known as ‘slow orthodontic extrusion’ because it enables tooth movement while simultaneously displacing the surrounding bone and soft tissue at an approximate rate of 0.5–1 mm per month.5
This case report presents a challenging clinical scenario for the successful implant rehabilitation of UL1. First, UL1 presented with a vestibular malposition and an 8-mm gingival recession, making it impossible to effectively address through any periodontal plastic procedures without prior orthodontic treatment.15 Secondly, the site presented with a complete absence of labial plate, accompanied by vertical and horizontal bone loss. These anatomical factors must be considered and addressed before tooth extraction, as the outcome will result in a Type III socket, where both the facial soft tissue and the buccal bone plate will be significantly compromised following the extraction, thereby preventing implant placement.16 In our clinical case, the orthodontic treatment corrected the malposition of UL1, thereby enabling the successful outcome for the mucogingival surgery, which effectively transformed the future Type III socket into a Type II socket.
It is acknowledged that Type II sockets require treatment, and immediate implant placement should be avoided. A staged approach, including additional hard tissue procedures before implant placement, is recommended.16,17 In our clinical case, orthodontic treatment enhanced the hard tissue contour of the socket and the bone peak between UR1 and UL1, facilitating the guided bone regeneration procedure. Additionally, the prior effective soft tissue management facilitated a tension-free primary closure of the wound, resulting in uneventful healing.18
Salama and Salama4 introduced a classification system for OE that focuses on the residual defect morphology and the regenerative potential of the extraction site. According to their classification, site UL1 was identified as a Type III site, marked by inadequate vertical and bucco-lingual bone dimensions.4 For these Type III sites, additional augmentation interventions should be considered, even though orthodontic extrusion has the potential to significantly enhance the site's anatomy, as demonstrated in our clinical case.19
By combining orthodontic therapy with implant placement, the literature reported successful results in the medium follow-up, however current knowledge about pre-implant orthodontic extrusion is mostly based on case reports and case series, which managed the cases using different techniques.14,19 Nevertheless, it is crucial to acknowledge that this technique is not devoid of potential complications. Orthodontic movements, particularly when applied to previously traumatized teeth or under excessive force, may lead to root resorption or induce ankylosis as a result of increased mechanical stress on the periodontal ligament.20
Based on this case report, a multidisciplinary approach that includes orthodontic treatment should be considered for rehabilitating complex cases in aesthetic areas. The success of this treatment depends on a comprehensive understanding of the interplay between hard and soft tissue profiles, an accurate diagnosis, thorough treatment planning and a meticulous implementation of all procedures.