Steele J, O'Sullivan I.: The NHS Information Centre for Health and Social Care; 2011
Henderson SJ. Risk management in clinical practice Part 11 – Oral surgery. Br Dent J. 2011; 210:17-23
Meechan JG, Greenwood M. General medicine and surgery for dental practitioners Part 9: Haematology and patients with bleeding problems. Br Dent J. 2003; 195:305-310
Robinson PD.Oxford: Elsevier; 2000
Carrotte PV, Waterhouse PJ. A clinical guide to endodontics – update Part 2. Br Dent J. 2009; 206:133-139
Wassell RW, Barker D, Walls AWG. Crowns and other extra-coronal restorations: impression materials and technique. Br Dent J. 2002; 192:679-690
Blinder D, Manor Y, Martinowitz U, Taicher S, Hashomer T. Dental extractions in patients maintained on continued oral anticoagulant: comparison of local haemostatic modalities. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999; 88:(2)137-140
Blinder D, Manor Y, Martinowitz U, Taicher S. Dental extractions in patients maintained on oral anticoagulant therapy: comparison of INR value with occurrence of postoperative bleeding. Int J Oral Maxillofac Surg. 2001; 30:(6)518-521
Carter G, Goss A. Tranexamic acid mouthwash – a prospective randomized study of a 2-day regimen vs 5-day regimen to prevent postoperative bleeding in anticoagulated patients requiring dental extractions. Int J Oral Maxillofac Surg. 2003; 32:(5)504-507
Thomson PJ, Greenwood M, Meechan JG. General medicine and surgery for dental practitioners. Part 6 Cancer, radiotherapy and chemotherapy. Br Dent J. 2010; 209:65-68
Perry DJ, Noakes TJC, Heliwell PS. Guidelines for the management of patients on oral anticoagulants requiring dental surgery. Br Dent J. 2007; 20:389-393
Scully C, Wolff A. Oral surgery in patients on anticoagulant therapy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002; 94:57-64
Birkhahn R Shock index in diagnosing early acute hypovolemia. Am J Emerg Med. 23:(3)323-326
Ballinger A, Patchett S. Pocket Essentials of Clinical Medicine, 4th edn. Oxford: Elsevier Saunders; 2008
The management of bleeding complications following a dental extraction is an essential skill for the dental practitioner. Extractions are often carried out on patients with complex medical histories and a long list of medications. This paper aims to help the clinician manage post-extraction haemorrhage. A review of the management of patients on anti-thrombotic medications will be covered in a subsequent paper.
Clinical Relevance: This article reviews the management of haemorrhage following tooth extraction; from the risk assessment of any underlying medical conditions and medications, to the clinical techniques used to control bleeding following an extraction.
Article
Haemostasis at the site of a dental extraction is considered to be a prerequisite before the patient leaves the clinic. Failure of haemostasis could occur in any patient; however, a number of different medical conditions and medications may interfere with this process.
The most recent Adult Dental Survey (2009) has shown a growing number of our patients are remaining dentate.1 People are living longer as a result of increasing health awareness and the success of medical treatments. The concept of ‘polypharmacy’ management requires dental clinicians to have an increased knowledge of the drugs that may affect dental treatment and their potential for drug interactions. Some drug therapies can increase the potential for bleeding post-operatively.
Risk assessment prior to embarking on a tooth extraction can allow the operator to foresee complications such as a haemorrhage. This involves careful planning and a thorough analysis of the medical history.2Table 1 shows the haemorrhage risk factors surrounding a dental extraction.
A sound knowledge of the physiology of haemostasis is important in understanding how haemorrhage may occur. A full description of the process is outside the remit of this paper; however, several key points are worth noting.
The process of haemostasis involves:
Vasoconstriction – vascular spasm in smooth muscle in the walls of blood vessels;
Platelet plug formation – adhesion, interaction and aggregation of platelets;
Coagulation cascade/network – clotting factors in the extrinsic, intrinsic and common pathways lead to the formation of fibrin.
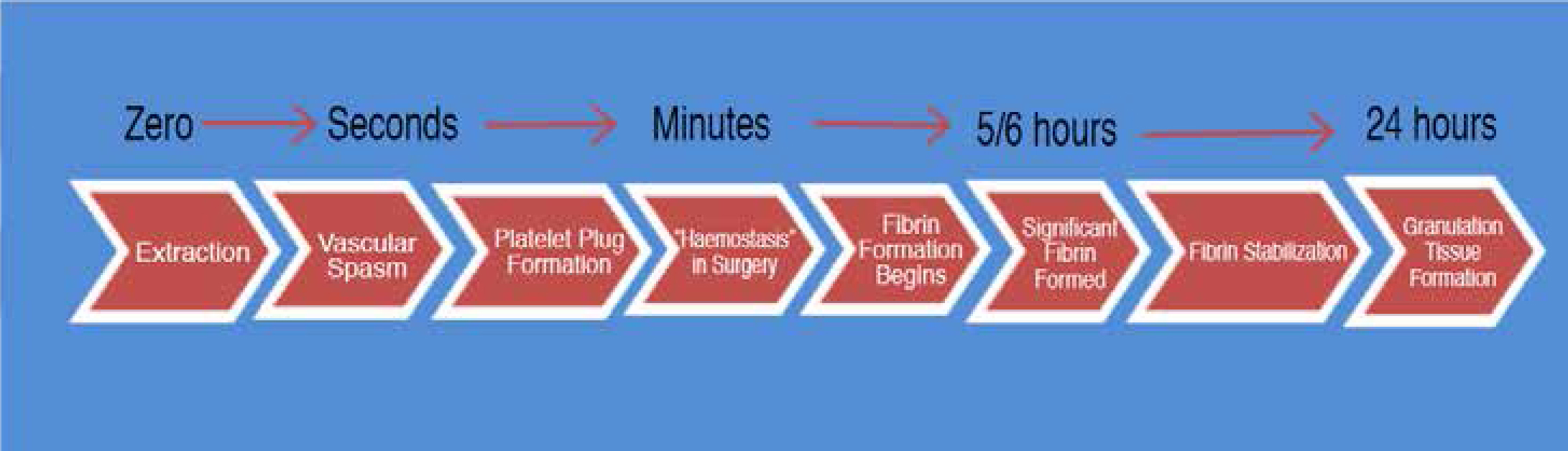
Clot formation is a dynamic process, involving a balance between the haemostatic and the fibrinolytic systems. The involvement of numerous cells, chemicals and plasma proteins are all required for successful haemostasis. Fibrinolysis occurs when the plasma enzyme plasminogen activates plasmin, which digests the fibrin threads in the clot. In health, this will occur once the site is repaired. Figure 1 outlines the timeline of clot formation.
Figure 1. Timeline of clot formation.
Consideration of the normal mechanism allows the clinician to interpret which patients may be at high risk of poor haemostasis. This may be the result of underactive clotting or overactive fibrinolysis. Systemic disease may interfere with clotting. The majority of clotting factors are produced by the liver, whereas platelets are produced in red bone marrow. Problems relating to clotting factors and platelets may be congenital or acquired.3 An example of a congenital deficiency of clotting factors is Haemophilia A (Factor VIII deficiency). Acquired liver disease may reduce production of clotting factors. Table 2 outlines the conditions that may give rise to a higher risk of post-extraction haemorrhage.
Clotting Factor Deficiencies
Haemophilia A (Factor VIII)
Haemophilia B (Factor IX)
Von Willebrand's Disease (vWF Factor)
Vitamin K Deficiency (Factor II, VII, IX and X)
Acquired liver disease – hepatitis/cirrhosis
Platelet Deficiency (Thrombocytopenia)
Idiopathic
Drug Induced (Antiplatelet therapy)
Anticoagulant Therapy
Vascular Anomalies
Atriovenous malformation
Hereditary haemorrhagic telangiectasia
Collagen disorders
Types of post-extraction haemorrhage
The classification of a haemorrhage is important as it has direct clinical implications. Post-extraction haemorrhage may be categorized in relation to timing:4
Primary haemorrhage – the bleeding occurs at the time of the surgery;
Reactionary haemorrhage – 2–3 hours after the procedure as a result of cessation of vasoconstriction;
Secondary haemorrhage – up to 14 days after the surgery. The most likely cause of this is infection.
The haemorrhage may also be classified according to the site affected:
Soft tissue;
Bone;
Vascular.
The diagnosis informs the management as described below.
Armamentarium for dealing with post-extraction haemorrhage
A key responsibility for a clinician is to ensure that his/her surgery is adequately equipped to deal with commonly occurring scenarios. Haemostatic agents and equipment have a wide range of uses beyond post-extraction haemorrhage. Several invasive procedures, such as non-surgical periodontal therapy, periodontal surgery, pulpotomy5 and the preparations of teeth for indirect restorations6 may all require the use of appropriate haemostatic agents. All dental practices should be prepared to deal with the initial management of a haemorrhage, even if onward referral is needed for definitive treatment. Table 3 shows a list of equipment that is useful in dealing with a post-extraction haemorrhage. The appropriate use of each will be described.
When faced with a post-extraction haemorrhage the dentist should remain calm and ensure that the area can be well visualized. This will allow the best opportunity to make the correct diagnosis, identifying the type of post-extraction haemorrhage and the site of the haemorrhage, therefore enabling quick and effective management.
Immediate post-extraction management
Once a tooth has been removed, pressure should be placed on the buccal and lingual/palatal surfaces of the alveolus around the socket. Extraction of a tooth via the intra-alveolar approach causes expansion of the alveolus around the root(s) of the tooth. The immediate bucco-lingual pressure reduces the ‘dead space’ of the wound and is the first step to help gain haemostasis. This should be done immediately following the extraction of a tooth with intact apices, usually termed digital pressure. A piece of sterile gauze may then be rolled up so that it is big enough to cover the socket. This can be placed directly over the socket area and the patient asked to bite down to apply the necessary pressure. It is important to note that, if an edentulous area opposes the extraction site, biting together may not apply enough firm pressure. It is advisable in this case to use finger pressure on the gauze for several minutes.
In many cases, this firm pressure will allow initial haemostasis to be achieved. The clot should begin at the base of the socket. It is a good idea to check that the clot is not removed with the gauze. A second piece of gauze can be placed in the same way. This time removal should show no fresh bleeding.
Whilst waiting for haemostasis to occur, or once haemostasis is confirmed, the patient should be given clear instructions on his/her post-operative management of the socket. This stage must not be overlooked, as failure to care for the area appropriately may cause a secondary haemorrhage. The instructions should be given verbally by the clinician who carried out the procedure. This will allow the provision of the core instructions, as well as any tailored instructions that are suitable to a particular patient (eg high risk of haemorrhage or a tobacco smoker). An extraction can be a traumatic event for some patients. These patients may not be able to recall a long list of instructions immediately afterwards. It is therefore advisable to provide a concise instruction leaflet that the patient can refer to in his/her own time (Table 4). However, providing the leaflet without comprehensive verbal instructions is unacceptable.
Do Not:
Rinse your mouth out today (may dislodge clot if fibrin stabilization has not occurred).*
Drink alcohol or hot drinks today (may increase blood pressure or induce hyperaemia).
Smoke or use tobacco products for at least 24 hours (causes vasoconstriction and possible increase in dry socket).
Chew food for 4 hours, avoid hard foods for 24 hours (may disturb clot, possible self harm if area still anaesthetized).
Carry out any physical activity today (increasing blood pressure).
Do:
Sip lukewarm drinks carefully (helps avoid clot removal by washing out socket).
Bite on gauze or clean, damp handkerchief for 10 minutes if area bleeds, preferably sitting upright in a chair.
Rinse mouth gently with hot salt mouthwash or Chlorhexidine (0.2%) mouthwash after 24 hours. Continue regular mouthwash use over the following week, especially after meals.
Clean teeth as normal, avoiding area of surgery for 24 hours.
Include contact details for advice and treatment for ‘out of hours’ care
*In brackets: rationale for the suggestion.
Patients having treatment under IV or inhalation sedation may have their ability to retain information reduced significantly in the immediate post-operative period. The clinician must allow for this, giving the aftercare instructions at the previous appointment or pre-operatively. The patient's chaperone must have adequate information to ensure the aftercare is safe and appropriate.
As mentioned above, if immediate pressure to the socket does not control bleeding, a diagnosis needs to be made regarding the aetiology.
Soft tissue haemorrhage
The intra-oral soft tissues are highly vascularized and may be the site of substantial haemorrhage. Diagnosis is made using good visualization, requiring good lighting and appropriate suction. Soft tissue bleeding may be prolonged as a result of inflamed tissues or a mucosal tear. A local anaesthetic containing a vasoconstrictor may minimize the bleed initially. A large area of infection causes granulation tissue to form at the base of the socket. This may impair clotting and bleed profusely. Any unattached clots should be cleaned from the mouth and an assessment made. If the diagnosis is a soft tissue haemorrhage, the correct equipment should be used to achieve haemostasis.
Suturing equipment
Sutures will aid socket closure and help bring the tissues together. They are available in different sizes and materials.7 Suture materials may be classified into:
Braided or monofilament;
Resorbable or non-resorbable;
Synthetic or natural.
These can then be placed with various techniques and using needles of different sizes and shapes. Each classification of material has its advantages and disadvantages, the most notable being that non-resorbable sutures require removal after a suitable healing period, whereas resorbable sutures will break down over time.
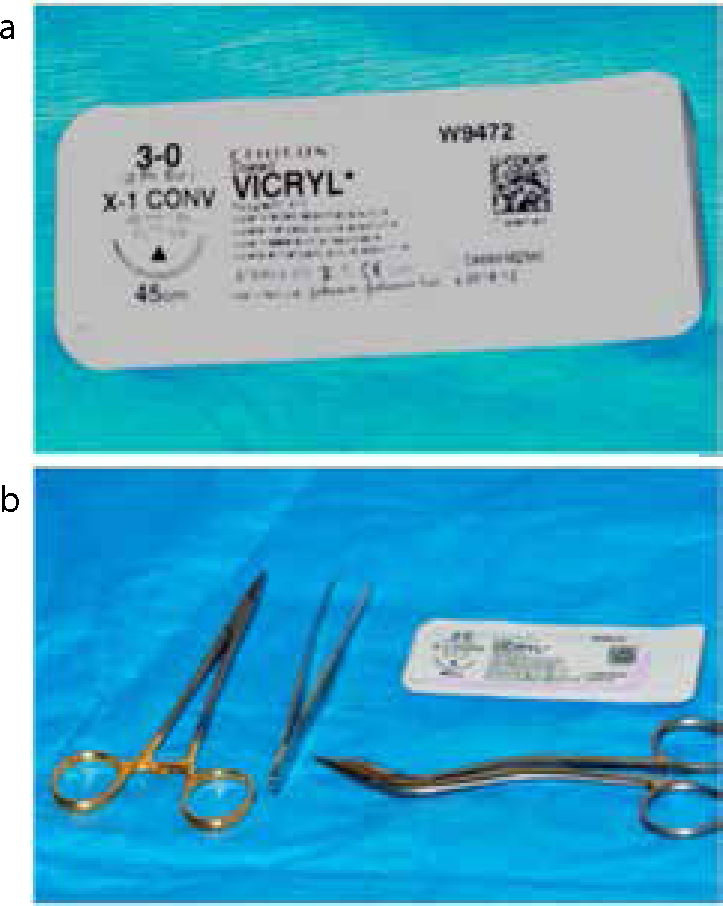
A 3.0 suture (Figure 2) on a ½ circle curved needle is a very useful suture for intra-oral wounds. A resorbable material, such as vicryl® 3.08 (a synthetic, braided and resorbable material made of polygactin) is recommended. This will offer between 7–10 days of support before being resorbed, enough for sufficient healing to have taken place. A simple interrupted suture is the most commonly placed,9 however, a horizontal mattress suture may provide suitable socket closure.
Figure 2. 3.0 Vicryl suture with suturing equipment.
Chemical haemostatic agents
Several agents that may help haemostasis are available to the dental practitioner. These include:
Tranexamic acid;
Ferric sulphate;
Silver nitrate.
Tranexamic acid
Tranexamic acid can be effective in the control of post-operative bleeding.10,11 The British Committee for Standards in Haematology advise that patients on oral anticoagulants requiring dental surgery can be prescribed 5% tranexamic acid mouthwash, to be used as a rinse, four times daily, for two days post-operatively.12 It is worth noting that tranexamic acid is not readily available in the primary care setting. It is not first line management for soft tissue haemorrhage, suturing and haemostatic gauze being the preferred option.
Ferric sulphate
Ferric sulphate is a commonly used astringent solution (15.5%) that has multiple uses in dentistry. It may be employed as part of a gingival retraction technique for impressions in crown/bridge work. It is also used as a haemostatic agent during pulpotomy. It is not widely used primarily to control post-extraction haemorrhage, however, it may offer assistance with mucosal tears or uncontrolled bleeding in gingival tissues.
Silver nitrate
Silver nitrate is included in this section for completeness. It is available in the form of a pencil (Figure 3) which contains 95% silver nitrate. It may be used to aid haemostasis in areas where suturing or finger pressure is not possible. A typical indication would be after a mucosal biopsy is taken from an area such as the hard palate or retromolar pad. Silver nitrate is a powerful chemical cauterizing agent; the pencil tip can be pressed directly on the bleeding area. After a few minutes, the silver nitrate should be de-activated by gently swabbing the area with saline solution to avoid damage to surrounding structures.
Figure 3. 95% Silver nitrate pencil.
Bleeding from the socket
Bony haemorrhage
Bleeding from a bony origin may occur following any dental extraction. This can be deep in an exposed socket, with the blood flow, making it difficult to visualize. In most cases, bleeding from within the socket can be arrested by inserting a pack. Cancellous bone can be burnished with a flat plastic instrument or a Mitchell's trimmer to help compress the bone in the area.
Haemostatic gauze
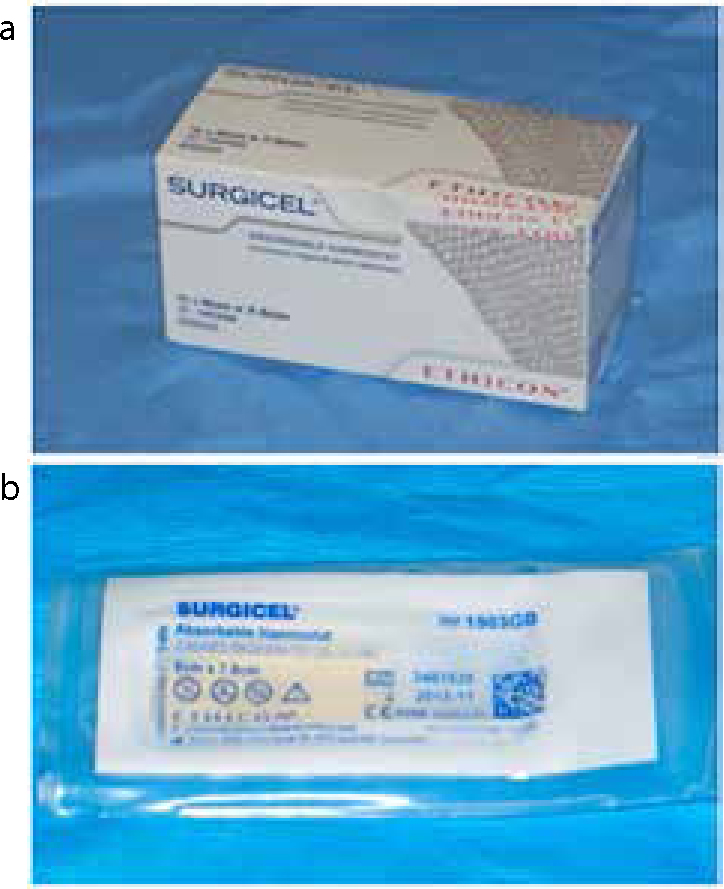
The availability of resorbable haemostatic dressing materials means that, in many instances, the clinician will choose to pack the socket with a dressing and then place a suture. The use of oxidized regenerated cellulose13 (Surgicel® – Figure 4), a collagen sponge (Haemocollagen®) or a resorbable gelatin sponge (Gelfoam®) is recommended, along with suture placement when the patient is at high risk of a post-operative haemorrhage.14,15 Non-resorbable dressings are also available (Kaltostat®), however, these are less desirable as they require removal and therefore the socket area has to be disturbed.
Figure 4. Surgicel®, which is oxidized regenerated cellulose.
Bone wax
Bone wax (Figure 5) consists of beeswax, paraffin and a softening agent. It may be used to control bleeding within cancellous bone. The origin of the bleed must be confirmed, and the wax is packed into the spaces within the bone. The pressure provided from the wax aids haemostasis. Bone wax is non-resorbable and the host may treat it as a foreign body. This means preferably bone wax should be removed after placement when haemostasis has occurred, although it often remains in situ, as complete removal can be difficult. Wax placement is usually followed by placement of haemostatic gauze and a suture to maintain pressure on the socket.
Figure 5. Bone wax.
Vascular haemorrhage
This type of haemorrhage may cause the most distress to a patient given the excessive amount of blood flow. A large vessel may require ligation, whereas smaller vessels can be cauterized. If the vessel is not visible, a flap may have to be raised to allow access and identification. If the practitioner does not feel confident in managing this, the patient should immediately be referred to the local accident and emergency department or maxillofacial unit. The dental professional should always be aware of the local services in the region.
Electrocautery
Electrocautery is the process of sealing the exposed end of the vessel with heat conduction. If electrocautery is available, the haemorrhaging vessel should be identified and cauterized.
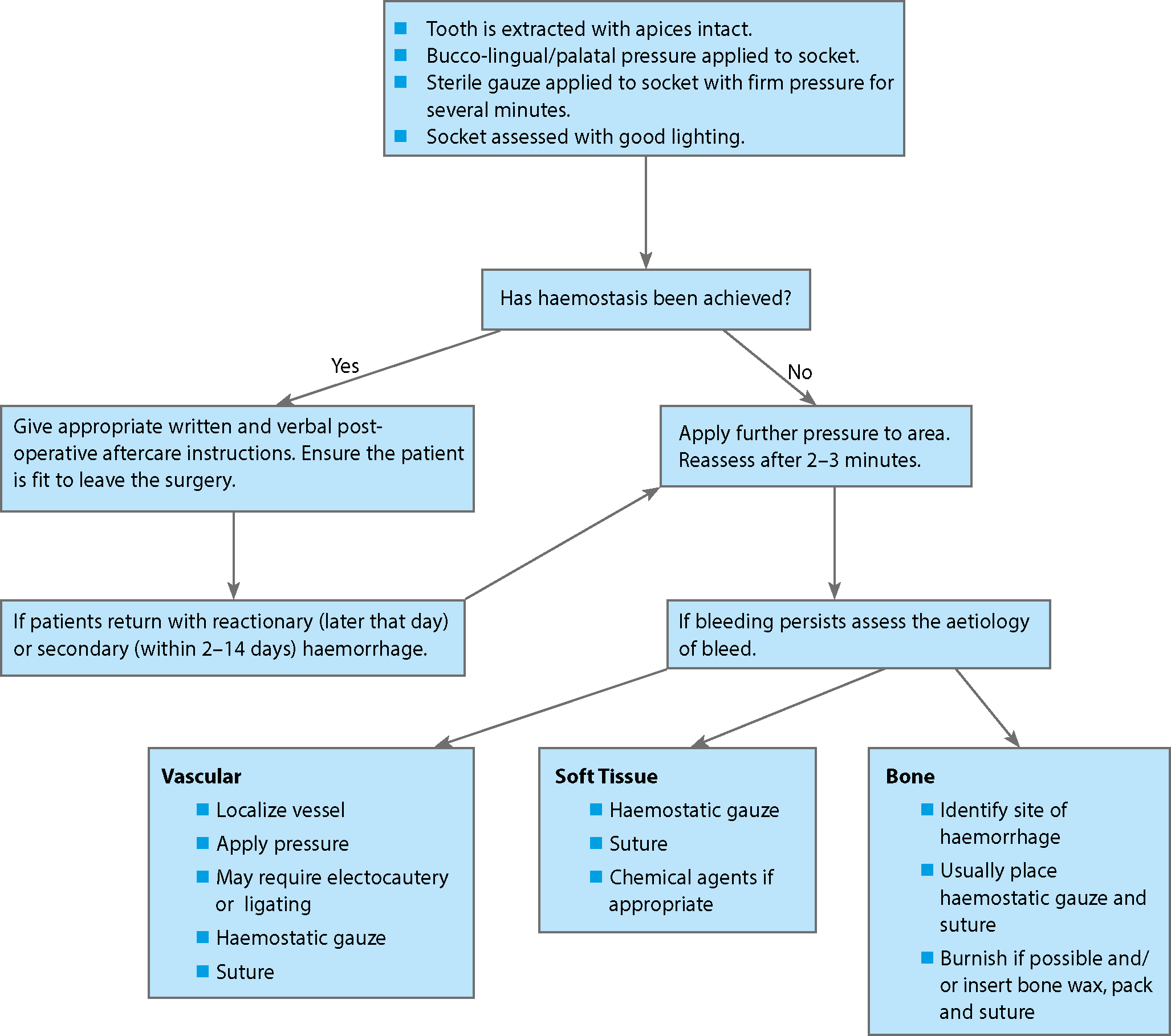
Figure 6 summarizes the suitable management of a post-operative haemorrhage.
Figure 6. Management of post-extraction haemorrhage.
Systemic monitoring
Monitoring equipment is helpful in assessing the significance of the bleed on the patient's systemic health. This is of particular importance when dealing with a secondary haemorrhage. Although the above methods may manage the haemorrhage, one must consider how much blood the patient may have already lost before presentation. The patient's blood pressure should be monitored using a sphygmomanometer, whilst heart rate can be measured manually or in combination with saturated oxygen levels using a pulse oximeter. A patient should be referred to accident and emergency if it is not possible to arrest haemorrhage and his/her readings show:
Diastolic blood pressure is consistently less than 60 (hypotensive state) in a short monitoring period;
Systolic blood pressure is consistently less than 100 in a short monitoring period.16
Heart rate is consistently raised (tachycardia) over 100 bpm, particularly with normotensive or hypotensive readings.17
Patients showing the above signs will require urgent assessment and fluid replacement as these are signs of surgical (hypovolaemic) shock.
Conclusion
A post-operative haemorrhage may occur as a complication of any dental extraction. The correct diagnosis of the aetiology will provide the quickest route to successful management.