Field E, Nind D, Varga E, Martin M The effect of chlorhexidine irrigation on the incidence of dry socket: a pilot study. Br J Oral Maxillofac Surg. 1988; 26:395-401
Hermesch C, Hilton T, Biesbrock A Perioperative use of 0.12% chlorhexidine gluconate for the prevention of alveolar osteitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol. 1998; 85:381-387
Cardoso C, Rodrigues M, Júnior O Clinical concepts of dry Socket. J Oral Maxillofac Surg. 2010; 68:1922-1932
Birn H Etiology and pathogenesis of fibrinolytic alveolitis (‘dry socket’). Int J Oral Surg. 1973; 2:211-263
Sharif M, Dawoud B, Tsichlaki A, Yates J Interventions for the prevention of dry socket: an evidence-based update. Br Dent J. 2014; 217:27-30
Fazakerley M, Field EA Dry socket: a painful post-extraction complication (a review). Dent Update. 1991; 18:31-34
Alexander R Dental extraction wound management: a case against medicating postextraction sockets. J Oral Maxillofac Surg. 2000; 58:538-551
Daly B, Sharif M, Newton T Local interventions for the management of alveolar osteitis (dry socket). Cochrane Database Syst Rev. 2012; 12
Syrjänen S, Syrjänen K Influence of Alvogyl on the healing of extraction wound in man. Int J Oral Surg. 1979; 8:22-30
Miller W, Ripley J Foreign body potential of the constituents of BIPP. An analysis. Br Dent J. 1974; 137:278-280
Eslami A, Van Swol R, Sadeghi E Connective tissue reactions to 3% tetracycline ointment in rat skin. J Oral Maxillofac Surg. 1987; 45:866-872
Moore J, Brekke J Foreign body giant cell reaction related to placement of tetracycline-treated polylactic acid: report of 18 cases. J Oral and Maxillofac Surg. 1990; 48:808-812
Summers L, Matz L Extraction wound sockets. Histological changes and paste packs – a trial. Br Dent J. 1976; 141:377-379
Tasoulas J, Daskalopoulos A, Droukas C, Nikitakis N An unusual microscopic pattern of foreign body reaction as a complication of dry socket management. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015; 120
Abdullgaffar B Alvogyl dental dressing: a potential cause of complicated postextraction non-healing sockets: a clinicopathologic study of 7 cases. Int J Dent Oral Health. 2016; 2:(4)1-4
Alveolar osteitis (AO) is a painful complication experienced by approximately 3–4% of patients who have undergone a dental extraction. A frequently used intra-alveolar dressing material, such as Alveogyl is commonly used to treat sockets where a diagnosis of AO is made. However, unexpected problems may be encountered by the dentist when using such materials and this article explores a case where a diagnosis of a foreign body reaction to Alveogyl was identified in a symptomatic patient with no overt clinical or radiographical signs.
CPD/Clinical Relevance: Dental professionals should be aware of the possible complications with the use of Alveogyl in the treatment of alveolar osteitis, in particular foreign body reactions.
Article
Alveolar osteitis (AO), also known as dry socket, is a well-recognised complication that may occur following dental extractions. Its characteristic features include halitosis and severe pain commencing 2–3 days post-operatively, which has the potential to radiate within the maxillofacial region.1 The severity of the symptoms limits the patient's functional capability because they often present acutely to the dentist. The incidence of AO has been reported to be 3–4%.2,3
The aetiology of AO has been debated since its first identification in 1896, and a number of theories exist.4 Birn5 suggested that a combination of direct and indirect factors contributes to the development of AO, including surgical trauma and the effects of bacteria on the activation of the plasminogen pathway.6 This theory was supported by Fazakerley and Field7 who described the fibrinolytic process and the premature degradation of the blood clot in the socket. Hence, sockets are often found to contain debris and remnants of the dislodged clot.
A number of predisposing factors that increase the risk of developing AO have been identified, including tobacco use, female gender, increasing age, oral contraceptive pill use, third molar surgery and pre-existing dental disease, such as periodontitis.6 It is clear that a wide range of factors contributes to the development of AO. Therefore, dental professionals are likely to encounter cases of AO in both primary and secondary settings.
The management modalities available for treating AO include a spectrum of intra-alveolar medicaments.8 However, a Cochrane systematic review found there was insufficient evidence to support any one treatment option in the management of AO9 and there are reports that that intra-alveolar dressings can impede the healing process.10
Originally named Alvogyl and reformulated in 2011, Alveogyl is a proprietary dental dressing material containing eugenol (analgesic action) and penghawar djambi (fibres from the tree fern, Cibotium barometz), among other ingredients. Its fibrous and paste-like properties prevent easy dislodgment of the medicament.
Case report
A 74-year-old female patient was referred by her general dental practitioner (GDP) to a dental teaching hospital for the extraction of a symptomatic, fully erupted, lone standing and grade one mobile lower left third molar. Her past medical history included a background of medication-controlled hypertension, asthma and arthritis. She had never used tobacco or alcohol.
Extra-and intra-oral examinations revealed a lower left wisdom tooth (LL8) that was tender on percussion, and mobile, but with no associated swellings. She was partially dentate and displayed good oral hygiene with no evidence of active periodontal disease. A diagnosis of chronic peri-apical periodontitis was made taking into account the clinical and radiographic findings. The LL8 was uneventfully extracted under local anaesthetic, with no complications. Appropriate departmental guidelines were followed with regards to post-operative advice and care.
The patient presented to the department 6 days post-operatively with symptoms suggestive of AO from the extraction site. Following review, a clinical diagnosis of AO was made, and the socket was irrigated with 0.2% chlorhexidine gluconate mouth rinse and Alveogyl dressing was placed as per the manufacturer's guidance. Unfortunately, the pain did not abate, and she returned with persistent symptoms from the LL8 socket. A similar approach as above was undertaken and Alveogyl was used again to provide therapeutic relief. She was reviewed after 2 weeks, and discharged into primary care because her symptoms had resolved.
Approximately 12 months later, the patient was re-referred to the department with new-onset ‘low grade’ pain from the LL8 region. A thorough examination revealed no abnormalities with no signs of infection or inflammation. There was complete mucosal coverage. Radiographic examination excluded retained tooth fragments. There was evidence of bony healing, as expected, and no remnants of tooth fragment were found. This was reassuring, yet confusing, as the patient's symptoms continued to persist.
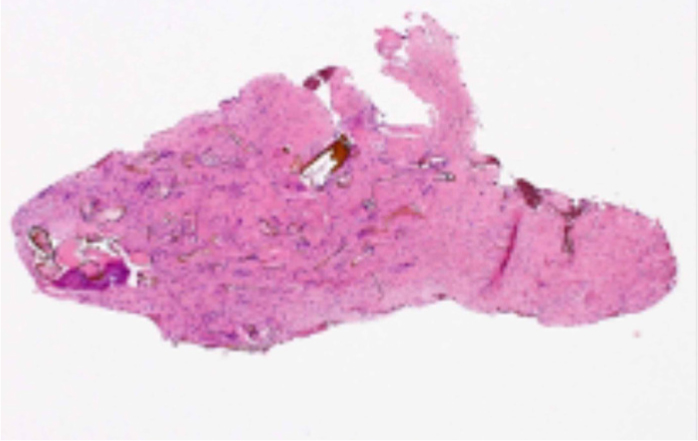
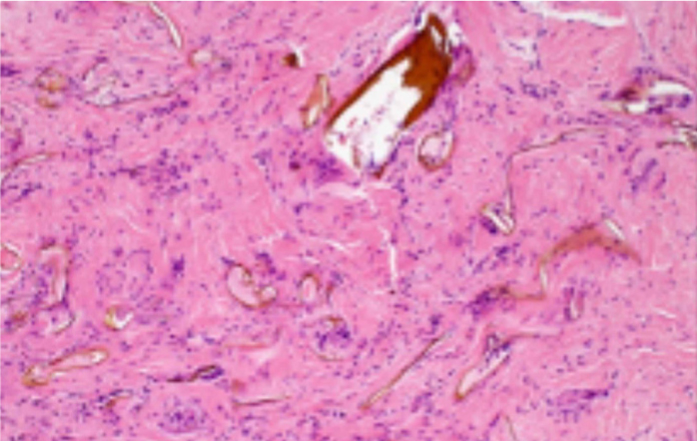
An examination under local anaesthetic uncovered the presence of granulation tissue with brownish material at the site of the previous extraction. This was removed and sent for histopathological examination (Figures 1 and 2). The histology report revealed ‘a fragment of dense fibrous tissue containing numerous refractile brown exogenous foreign materials consistent with Alveogyl dressing material, with an associated foreign body type multinucleate giant cell reaction.’ A diagnosis of a foreign body reaction to Alveogyl was recorded. On review, the patient's symptoms had resolved.
Figure 1. Cellular fibrous tissue with scattered brown exogenous material.Figure 2. Cellular fibrous tissue with scattered brown exogenous material some associated with foreign body-type giant cell reaction.
Discussion
The use and study of intra-alveolar medicaments has long been documented, and there is mounting evidence that they can cause impairment to the healing process.11,12,13,14,15 The nature of their non-dissolvable properties makes them prime candidates for potential foreign body reactions to occur. They rely on complete self-elimination out of the extraction socket. Alveogyl is a foreign biomaterial that is frequently used by dentists in the management in AO for its therapeutic properties.
The literature, however, highlights some areas of concern when using Alvogyl/Alveogyl in AO. One study found ‘retardation of healing and marked inflammation’ following the use of Alvogyl in the tooth sockets of dogs who had undergone extractions.15 Another case documented similar symptoms, but with radiographic abnormalities from the Alvogyl in contrast to the bony infiltration noted in this case.16 In a study that assessed the histological findings of extraction sockets dressed with and without Alvogyl, evidence of delayed wound healing, and a higher level of fibrous tissue inflammatory reaction and giant cells were found in the sockets dressed with Alvogyl.10
Other materials, such as BIPP, have also been reported to cause a foreign body reaction and delay wound healing.11 To date there is a lack of evidence to substantiate and support the use of intra-alveolar medicaments in the treatment of AO.9
It has been proposed that the penghawar djambi found in Alveogyl may be a causative factor in this inflammatory reaction.17 The fibres are haemostatic and their texture makes the product slow to dislodge from the extraction socket. While there are benficial local effects from the use of Alveogyl, it may be the case that if not all fibres are eliminated from the wound, a potential foreign body reaction may result.
It is prudent that dentists using Alveogyl, or other intra-alveolar medicaments, do so with due caution and care to ensure that healing progresses unhindered. Review patients who present with pain following intra-alveolar medicament use is important because the consequences of failed elimination may be avoidable pain and discomfort for t he patient.
Conclusion
This case demonstrates the effects of Alveogyl when it was retained within the socket and led to a foreign body reaction. The immediate resolution of symptoms is well achieved by Alveogyl; however, its fern-derived fibres are not self-eliminating and it must be used as per the manufacturer's guidance that it be loosely placed, not condensed, within the socket.18 Should a patient's pain continue following placement of Alveogyl, review is recommended to assess its elimination and healing of the extraction socket.