Floriano PN, Christodoulides N, Miller CS, Ebersole JL, Spertus J, Rose BG Use of saliva-based nano-biochip tests for acute myocardial infarction at the point of care: a feasibility study. Clin Chem. 2009; 55:1530-1538
Andersen DH. Cystic fibrosis of the pancreas and its relation to celiac disease: a clinical and pathological study. Am J Dis Child. 1938; 56:344-399
Slomiany BL, Aono M, Murty VL, Slomiany A, Levine MJ, Tabak LA. Lipid composition of submandibular saliva from normal and cystic fibrosis individuals. J Dent Res. 1982; 61:1163-1166
Wiesman UN, Boat TF, diSant'Agnese PA. Flow-rates and electrolytes in minor-salivary-gland saliva in normal subjects and patients with cystic fibrosis. Lancet. 1972; 2:510-512
Blomfield J, Rush AR, Allars HM, Brown JM. Parotid gland function in children with cystic fibrosis and child control subjects. Pediatr Res. 1976; 10:574-578
al-Bayaty HF, Aldred MJ, Walker DM Salivary and serum antibodies to gliadin in the diagnosis of celiac disease. J Oral Pathol Med. 1989; 18:578-581
Hakeem V, Fifield R, al-Bayaty HF Salivary IgA antigliadin antibody as a marker for coeliac disease. Arch Dis Child. 1992; 67:724-727
Zerah M, Pang SY, New MI. Morning salivary 17-hydroxyprogesterone is a useful screening test for nonclassical 21-hydroxylase deficiency. J Clin Endocrinol Metab. 1987; 65:227-232
Parry JV, Perry KR, Panday S, Mortimer PP. Diagnosis of hepatitis A and B by testing saliva. J Med Virol. 1989; 28:255-260
Thieme T, Piacentini S, Davidson S, Steingart K. Determination of measles, mumps, and rubella immunization status using oral fluid samples. J Am Med Assoc. 1994; 272:219-221
Malamud D. Saliva as a diagnostic fluid. Br Med J. 1992; 305:207-208
Cordeiro ML, Turpin CS, McAdams SA. A comparative study of saliva and OraSure oral fluid. Ann NY Acad Sci. 1993; 694:330-331
Gaudette D, North L, Hindahl M, Griffin K, Klimkow N, Thieme T. Stability of clinically significant antibodies in saliva and oral fluid. J Clin Immunoassay. 1994; 17:171-175
Ben-Aryeh H, Spielman A, Szargel R Sialochemistry for diagnosis of Sjögren's syndrome in xerostomic patients. Oral Surg Oral Med Oral Pathol. 1981; 52:487-490
Stuchell RN, Mandel ID, Baurmash H. Clinical utilization of sialochemistry in Sjögren's syndrome. J Oral Pathol. 1984; 13:303-309
Tan EM. Antinuclear antibodies: diagnostic markers for autoimmune diseases and probes for cell biology. Adv Immunol. 1989; 44:93-151
Horsfall AC, Rose LM, Maini RN. Autoantibody synthesis in salivary glands of Sjögren's syndrome patients. J Autoimmun. 1989; 2:559-568
Hu S, Wang J, Meijer J Salivary proteomic and genomic biomarkers for primary Sjögren's syndrome. Arthritis Rheum. 2007; 56:3588-3600
Robbins SL, Cotran RS. In: Kumar V, Abbas AK, Fausto N (eds). New Delhi: Saunders; 2004
Tavassoli M, Brunel N, Maher R, Johnson NW, Soussi T. p53 antibodies in the saliva of patients with squamous cell carcinoma of the oral cavity. Int J Cancer. 1998; 78:390-391
Mizukawa N, Sugiyama K, Fukunaga J Defensin-1, a peptide detected in the saliva of oral squamous cell carcinoma patients. Anticancer Res. 1998; 18:4645-4649
Franzmann EJ, Reategui EP, Carraway KL, Hamilton KL, Weed DT, Goodwin WJ. Salivary soluble CD44: a potential molecular marker for head and neck cancer. Cancer Epidemiol Biomarkers Prev. 2005; 14:735-739
Streckfus C, Bigler L, Tucci M, Thigpen JT. A preliminary study of CA15–3, c-erbB-2, epidermal growth factor receptor, cathepsin-D, and p53 in saliva among women with breast carcinoma. Cancer Invest. 2000; 18:101-109
Chien DX, Schwartz PE. Saliva and serum CA 125 assays for detecting malignant ovarian tumors. Obstet Gynecol. 1990; 75:701-704
Drobitch RK, Svensson CK. Therapeutic drug monitoring in saliva. An update. Clin Pharmacokinet. 1992; 23:365-379
Haeckel R, Hanecke P. Application of saliva for drug monitoring. An in vivo model for transmembrane transport. Eur J Clin Chem Clin Biochem. 1996; 34:171-191
Penttila A, Karhunen PJ, Pikkarainen J. Alcohol screening with the alcoscan test strip in forensic praxis. Forensic Sci Int. 1990; 44:43-48
Kaufman E, Lamster AB. The diagnostic applications of saliva – a review. Crit Rev Oral Biol Med. 2002; 13:197-212
Kidwell DA, Holland JC, Athanaselis S. Testing for drugs abuse in saliva and sweat. J Chromatogr B Biomed Sci Appl. 1998; 713:111-135
Wang DY, Fantl VE, Habibollahi F Salivary oestradiol and progesterone levels in premenopausal women with breast cancer. Eur J Cancer Clin Oncol. 1986; 22:427-433
Marchetti P, Benzi L, Masoni A Salivary insulin concentrations in type 2 (non-insulin-dependent) diabetic patients and obese non-diabetic subjects: relationship to changes in plasma insulin levels after an oral glucose load. Diabetologia. 1986; 29:695-698
Guyton AC, Hall JE.New Delhi: W B Saunders; 2000
Stroud LR, Salovey P, Epel ES. Sex differences in stress responses: social rejection versus achievement stress. Biol Psychiatry. 2002; 52:318-27
Sapolsky RM, Krey LC, McEwen BS. The neuroendocrinology of stress and aging: the glucocorticoid cascade hypothesis. Endocr Rev. 1986; 7:284-301
Rohleder N, Nater UM, Wolf JM, Ehlert U, Kirschbaum C. Psychosocial stress-induced activation of salivary alpha-amylase – an indicator of sympathetic activity?. Ann NY Acad Sci. 2004; 1032:258-263
Quissell DO. Steroid hormone analysis in human saliva. Ann NY Acad Sci. 1993; 694:143-145
Malamud D. Saliva as a diagnostic fluid. Dent Clin N Am. 2011; 55:159-178
Esposito S, Tremolati E, Begliatti E, Bosis S, Gualtieri L, Principi N. Evaluation of a rapid bedside test for the quantitative determination of C-reactive protein. Clin Chem Lab Med. 2005; 43:438-440
Christodoulides N, Mohanty S, Miller CS, Langub MC, Floriano PN, Dharshan P Application of microchip assay system for the measurement of C-reactive protein in human saliva. Lab Chip. 2005; 5:261-269
Karon BS, Gandhi GY, Nuttall GA, Bryant SC, Schaff HV, McMahon MM, Santrach PJ. Accuracy of Roche Accu Chek Inform whole blood capillary, arterial, and venous glucose values in patients receiving intensive intravenous insulin therapy after cardiac surgery. Am J Clin Pathol. 2007; 127:919-926
Yamaguchi M, Kanemaru M, Kanemori T, Mizuno Y, Yoshida H. Salivary amylase activity monitor used for stress evaluation. Conf Proc IEEE Eng Med Biol Soc. 2003; 4:3075-3078
Granger DA, Kivlighan KT, el-Shaikh M, Gordis EB, Stroud LR. Salivary alpha-amylase in biobehavioural research – recent developments and applications. Ann NY Acad Sci. 2007; 1098:122-144
Saliva is the most easily available and accessible body fluid, which makes it one of the most sought after tools in diagnostic pathology. Markers expressed in saliva can be used for diagnosis and concurrent patient follow-up of diseases ranging from hereditary disorders to infections, as well as malignancies and also analysis of therapeutic levels of drugs. The emergence of hand-held devices has made possible the elucidation of point-of-care methods and research in the field has resulted in the assimilation of knowledge useful for clinical applications.
Clinical Relevance: This article describes some of the latest research in saliva diagnostics and provides some information on the various hand-held devices available.
Article
Saliva is the fluid secreted by the salivary glands of the oral cavity. It is easy to collect from the patient, as it does not require an invasive procedure.1 It performs various functions, such as lubrication, protection, digestion, and is mainly formed of two components, namely, macromolecular components consisting of the proteins present in the saliva or the molecules present in the saliva; and the fluid component which forms the bulk of saliva.2 The constituents of saliva are derived as a filtrate of plasma, obtained from the local vasculature,3 as well as from the gingival crevicular fluids which also contains serum constituents. Thus, saliva consists of various proteins in proportion to their serum levels, and these can be used as markers. The presence of these markers therefore makes it a useful tool in the diagnosis of various conditions. It can be used to detect a number of diseases, and the development of microchips for the collection and quantification of salivary constituents will offer still further possibilities for its use in point-of-care testing,4 making possible the potential development of ‘lab-on-a-chip’ platforms.1 To understand the existence of these proteins in saliva, a basis for the formation and stimulation of saliva is important.
Why saliva?
The collection of saliva is a safe, non-invasive and simple method compared to the collection of blood.5 It can be collected without much patient discomfort, and the advantage over other fluids, such as sweat, is that it can be collected at the patient's convenience. Between plasma and serum, plasma is preferred, but it undergoes enzymatic degradation at a relatively faster rate, unless centrifuged, in contrast to saliva, which can be stored immediately at sub-zero temperatures. Also, the substrate concentration in blood for proteomic analysis shows sufficient variation, and also non-specific cross reaction, making it difficult to detect. A severe limitation with cancer biomarkers in blood is the limited expression due to the comorbidity effects of one disease influencing the biomarker's profile.6
Saliva can be collected either following stimulation, or unstimulated. The patient is simply asked to chew on a wax block for the collection of stimulated saliva, or allowed to drool directly into a sterile beaker for the collection of unstimulated saliva. The rate of flow can be calculated, which may serve as an aid in diagnosis of conditions such as xerostomia. Also, the use of a cannula can help in the collection of gland-specific saliva, which may be of use in the study of certain markers secreted by specific glands. The cannula is inserted in the duct of the gland from which saliva is to be obtained and attached on the other end to a collecting vessel.
Formation and stimulation of saliva
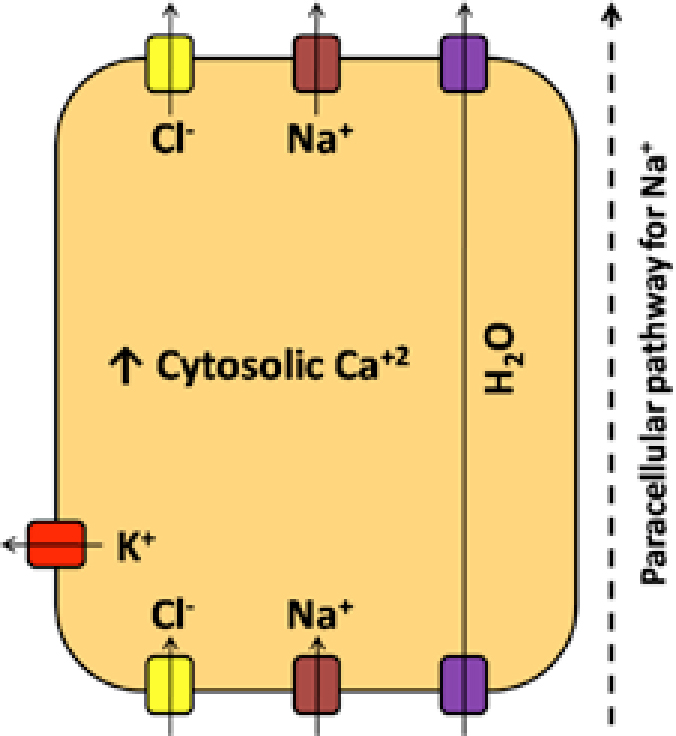
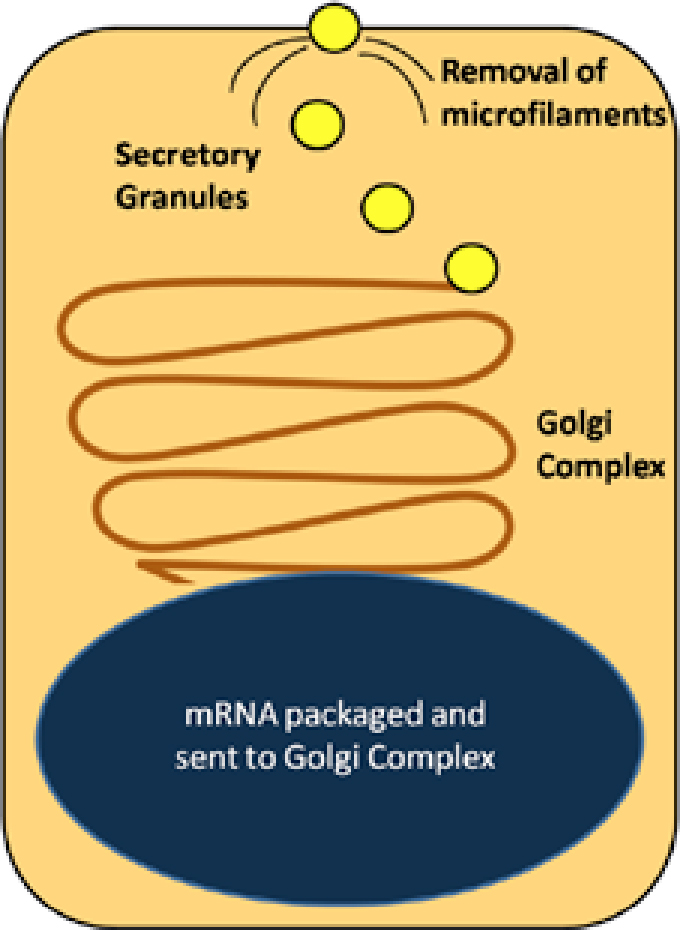
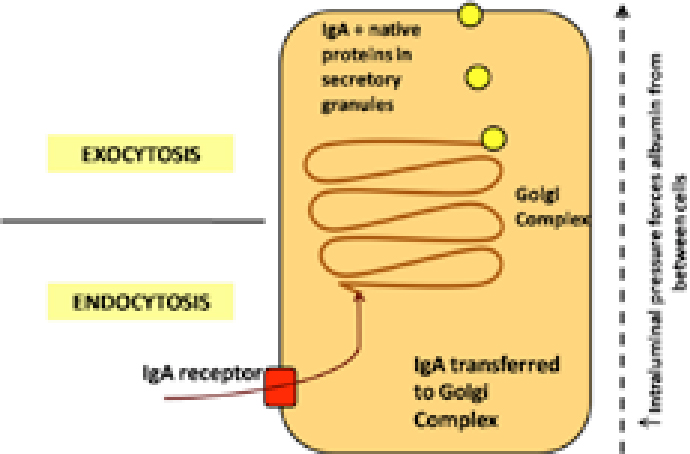
Saliva consists chiefly of macromolecular and fluid components. The fluid component consists mainly of water and forms the bulk of saliva. Water is taken in exchange for various ions by osmosis via the respective channels in the glandular cells (Figure 1). The macromolecular component is formed in two ways. It is taken up by endocytosis, and then released with native proteins by exocytosis (Figure 2). Also, the protein can be transferred to the saliva across the epithelial cell junctions (Figure 3).
Figure 1. Following release of free calcium (Ca+2), the increase in its cytosolic levels causes a compensatory change of potassium (K+) and chlorine (Cl-) channels opening, causing a compulsory uptake of sodium (Na+2) and chlorine. Sodium may also enter through paracellular pathway resulting in a flux of water through osmotic coupling forming salt (NaCl) and water (H2O). Hence, saliva is thought to be produced transcellularly.Figure 2. mRNA is manufactured in the nucleus and sent to the Golgi Complex, from where it is packaged in the secretory vacuoles. These carry them to the surface, and on response to stimulus fuse with the cell membrane after removing the web of microfilaments and discharge the contents in the lumen.Figure 3. IgA binds to a receptor at the basolateral surface from where it is relocated to the golgi complex (Endocytosis). It is packaged into secretory granules with the native proteins being secreted and released via exocytosis. Also, increase in intraluminal pressure causes the plasma proteins, such as albumin, to reach saliva by parting of the tight junctions.
The complex nervous stimulation of saliva has been studied extensively in the nervous system of animals as well as resin cast models in the past century.7 The salivary glands receive post ganglionic secretomotor nerves from both sympathetic and parasympathetic sources, from where they distribute to the muscle arterioles, secretory cells of the terminal end pieces, myoepithelial cells and cells of the intercalated and striated ducts, following the course of the local vasculature.2,8
There are two patterns of innervations in relation to the salivary glands:9
Epilemmal: the axons are separated from the secretory cells by a basement membrane. In the adjacent exoplasm, numerous secretory vesicles with neurotransmitter substances are present, which can diffuse 100–200 nm across the basement membrane before affecting the secretory cell;
Hypolemmal: the axons can penetrate their basement membrane by losing their Schwann cell covering, and they run between secretory cells separated by a gap of 10–20 nm. The presence of small mitochondria and vesicles with neurotransmitter substances on the sides of the bare axons in the form of beadings helps a signal axon to rapidly affect several secretory cells.
Secretion of saliva is usually elicited in response to stimulation of the autonomic innervation to the glands. Both salivary output and composition depend on the activity of the autonomic nervous system, and any modification of this activity can be observed indirectly by alterations in the salivary excretion.7 Parasympathetic impulses are the major nerve impulses created for the salivary control in general10 and their stimulation results in a copious flow of saliva, low in organic and inorganic compound concentrations, caused by a variable degree of exocytosis.11 Sympathetic stimulation, on the other hand, is present intermittently and produces saliva which is low in volume. It tends to modulate the composition of saliva by increasing exocytosis from certain cells, causing a higher organic and inorganic content, as seen in most of the other glands.10,12 The higher content is through the activity of adenyl-cyclase, causing elevated levels of total protein, especially the digestive enzyme alpha-amylase.12
Besides the type of autonomic receptor being activated, the intensity and the duration of stimulation to the glands also affects the salivary composition.7 The differences in composition on stimulation appear to be due to alterations in membrane permeability of secretory cells leading to changes in the rate at which electrolytes are lost from these cells. The parasympathetic nerve stimulation of the microcirculation of the glands results in different responses around the acini and ducts. Where the flow in acini slows initially before increasing, the flow in interlobular ducts increases soon after beginning stimulation.3 The sympathetic stimulation causes a marked increased degree of vasoconstriction7 and the response of myoepithelial cells and blood vessels of glands can also modify the quantity and composition of the elaborated saliva.8 Also, factors such as circannual rhythms and reflex-induced secretomotor responses might influence salivary secretion.2
Markers for various diseases
Biochemical markers are measurable and quantifiable biological parameters (eg specific enzyme concentration, specific hormone concentration, specific gene phenotype distribution in a population, presence of biological substances) which serve as indices for health- and physiology-related assessments, such as disease risk, psychiatric disorders, environmental exposure and its effects, disease diagnosis, metabolic processes, substance abuse, pregnancy, cell line development, epidemiologic studies, etc.13 These markers aid in diagnosing the disease, and also aid in determining the progress and prognosis of any specific condition.
Systemic conditions
Acute myocardial infarction can be feasibly diagnosed with a cocktail of saliva-based biomarkers consisting of C-reactive protein, myoglobin and myeloperoxidase which, along with ECG, provide excellent screening results.14
Cystic fibrosis is a genetically transmitted disease of children and young adults, which is considered as a generalized exocrinopathy.15 The elevated salivary calcium and phosphate levels,16 and also that of sodium with a decreased flow rate of saliva,17 may explain the demonstration of higher occurrence of calculus. The submandibular saliva demonstrates more lipids,16 although the parotid saliva does not demonstrate qualitative changes.18
Coeliac disease is a congenital disorder of the small intestine involving malabsorption of gluten. Higher levels of salivary IgA–AGA have been reported to be a sensitive and specific method for the screening of coeliac disease, and for monitoring compliance with the required gluten-free diet.19,20
21-hydroxylase deficiency is an inherited disorder of steroidogenesis leading to congenital adrenal hyperplasia wherein early morning salivary levels of 17-hydroxyprogesterone (17-OHP) were reported to be an excellent screening test for the diagnosis21
Viral
Saliva was found to be a useful alternative to serum for the diagnosis of viral hepatitis. Acute hepatitis A (HAV) and hepatitis B (HBV) were diagnosed based on the presence of IgM antibodies in saliva.22 Also, detection of antibodies in oral fluid samples produced sensitivity and specificity of 97% and 100% for measles, 94% for mumps, and 98% for rubella, respectively, in comparison with detection of serum antibodies for these viruses.23
Human Immunodeficiency Virus (HIV) can be assessed in saliva based on a specific antibody that is equivalent to serum in accuracy, and therefore applicable for both clinical use and epidemiological surveillance.24 Several salivary and oral fluid tests have been developed for HIV diagnosis, such as OraSure® (OraSure Technologies, Bethlehem, Pa, USA), which is a testing system that is commercially available in the United States and can be used for the diagnosis of HIV. The test relies on the collection of an oral mucosal transudate (and therefore IgG antibody). IgG antibody to the virus is the predominant type of anti-HIV immunoglobulin.25,26
Auto-immune disorders
Sjögren's syndrome (SS) is an auto-immune exocrinopathy of unknown aetiology with increased concentrations of sodium and chloride. Elevated levels of IgA, IgG, lactoferrin, and albumin, and a decreased concentration of phosphate were reported in saliva of patients with SS.27,28 SS is characterized by auto-antibodies to the La and Ro ribonucleoprotein antigens targeting intracellular proteins that may be involved in the regulation of RNA polymerase function.29 Auto-antibody, especially of the IgA class, can be synthesized in salivary glands and can be detected in the saliva of SS patients prior to detection in the serum.30 Recent advances in proteomic and genomic profiles of salivary markers have determined a series of biomarkers that could detect primary Sjögren's syndrome.31
Malignancy
p53 is known as the ‘molecular policeman’ in the cell cycle of keratinocytes and prevents multiplication of malignant cells.32 p53 antibody can be detected in the saliva of patients diagnosed with oral squamous cell carcinoma (SCC), and can thus assist in the early detection of, and screening for, this tumour.33 Defensins are peptides which possess antimicrobial and cytotoxic properties. Elevated levels of salivary defensin-1 were found to be indicative of the presence of oral SCC.34 Recently, sol CD44 is a salivary marker which has been effectively detected for head and neck squamous cell carcinoma at all stages.35
Elevated levels of recognized tumour markers c-erbB-2 (erb) and cancer antigen 15–3 (CA15–3) were found in the saliva of women diagnosed with breast carcinoma, as compared with patients with benign lesions and healthy controls.36
CA 125 is a tumour marker for epithelial ovarian cancer. Elevated salivary levels of CA 125 were detected in patients with epithelial ovarian cancer as compared with patients with benign pelvic masses and healthy controls.37
Drugs
Saliva has been used for monitoring systemic levels of drugs38 as they are known to appear via passive diffusion across a concentration gradient in saliva.39 Also, apart from diagnostic purposes, salivary levels of drugs can be used as an excellent tool for monitoring drug concentrations in the body.
Of particular interest is the use of saliva for the evaluation of illicit drug use. Following drug use, the appearance of the drug in saliva follows a time course that is similar to that of serum. In contrast, drugs appear at a later time in urine.40
Saliva may be used for monitoring patient compliance with psychiatric medications, anti-epileptic, anti-cancer, immunosuppressant and bronchodilating drugs.41 Also, other recreational drugs that can be identified in saliva are amphetamines, barbiturates, benzodiazepines, cocaine, phencyclidine (PCP), and opioids.42
Endocrinal status
Oestradiol can be detected in saliva in concentrations that are only 1–2% of serum concentrations.43 Insulin can be detected in saliva, and salivary insulin levels have been evaluated as a means of monitoring serum insulin levels.44
Stress
Research has focused on markers for conditions which are otherwise difficult to diagnose, like stress. Stress stimulates the hypothalamus, which in turn transmits the signals downwards through the reticular formation of the brain stem and the spinal cord,45 thus inducing the sympathetic impulses which cause an increase in exocytosis, resulting in more protein being secreted.10,12
Cortisone is a neutral steroid and therefore readily diffuses into saliva. Increase in serum cortisol has been used as a marker for psychological stress.46 However, owing to a longer latency of secretion,47 it is unsuitable to assess acute stress conditions.48 Also, the actual salivary cortisol levels are lower than the serum levels, possibly due to enzymatic degradation in the salivary epithelial cells during transcellular diffusion.49 The serum cortisol levels were not accurately reflected in salivary cortisol levels and thus it was considered to be not of much significance.50 Alpha-amylase is found in saliva as well as pancreatic secretions, with the salivary function chiefly being that of digesting starch. Salivary alpha amylase (sAA) has been known as a marker for adrenergic activity for a long time. The levels of salivary alpha amylase correlate to the levels of activity of the sympathoadrenal medullary system (SAM) and serves as an easy-to-use marker.48 Various other markers have been identified to analyse stress, such as substance P, lysozyme.51
Saliva as a tool for immediate diagnosis
Recent trends have shifted the idea of diagnosis towards simpler methods and immediate results, such as those offered by hand-held devices. These have been developed for various reasons, such as those for identifying C-reactive protein in inflammatory conditions, as well as cardiac abnormalities,52,53 checking glucose levels wherein coefficients of variants between the hexokinase method and the Accu-chek® method were less than 2%.54 A test strip with a salivary transcription device containing an optical analyser was developed and gave satisfactory readings.55 A study conducted by our group on patients with recurrent aphthous stomatitis suggested the rise of sAA levels during the occurrence of the lesions and a drop in sAA levels on resolution of the lesions (unpublished observations). The readings were obtained with a chairside kit (Cocorometer, Nipro Corp, Japan) for the measurement of the sAA levels.
Conclusion
Despite limitations, the use of saliva for diagnostic purposes is increasing in popularity. Several diagnostic tests are commercially available and are currently used by patients, researchers and clinicians. Saliva is particularly useful for qualitative diagnosis (detection of the presence or absence of a marker) rather than quantitative diagnosis. This makes it an important means for the detection of viral infection (especially HIV owing to the non-invasive method of collection), past exposure and immunity, and the detection of illicit drug use. It is also useful for the monitoring of hormone levels, especially steroids, and facilitates repeated sampling at shorter durations, which may be particularly important in avoiding patient compliance problems.
With the advent of technology, and as mentioned earlier, the use of various hand-held devices, the identification of biomarkers has been made easier. As more biomarkers are discovered, the diagnosis of disease and follow-up for the patient will continue to improve. Although encouraging, the growing literature on these biomarkers must be reviewed cautiously and monitored with care.56