Malden N, Beltes C, Lopes V. Dental extractions and bisphosphonates: the assessment, consent and management, a proposed algorithm. Br Dent J. 2009; 206:93-98
Rustemeyer J, Bremerich A. Bisphosphonate-associated osteonecrosis of the jaw: what do we currently know? A survey of knowledge given in the recent literature. Clin Oral Invest. 2010; 14:59-64
Bagan JV. Letter to the Editor. Jaw osteonecrosis associated with bisphosphonates: multiple exposed areas and its relationship to tooth extractions. Study of 20 cases. Oral Oncol. 2006; 42:327-329
Marx RE, Sawatari Y, Fortin M, Broumand V. Bisphosphonate-induced exposed bone (osteonecrosis/osteopetrosis) of the jaws: risk factors, recognition, prevention, and treatment. J Oral Maxillofac Surg. 2005; 63:1567-1575
Tortorici S, Burruano F, Difalco P. Maxillary bone necrosis following the use of formaldehyde containing paste: management and case series. Br Dent J. 2007; 203:(9)511-512
Bataineh AB, al-Omari MA, Owais AI. Arsenical necrosis of the jaws. Int Endod J. 1997; 30:(4)283-287
Loo Yi Kwan Nicotine-induced osteonecrosis. A case report. Dent Update. 2009; 36:289-291
McLeod NMH, Patel P, Kusanale A, Rogers SN, Brennann PA. Bisphosphonate osteonecrosis of the jaw – a literature review of UK policies versus international policies on the management of bisphosphonate osteonecrosis of the jaw. Br J Oral Maxillofacial Surg. 2011; 49:335-342
Filleul O, Crompot E, Saussez S. Bisphosphonate-induced osteonecrosis of the jaw: a review of 2400 patient cases. J Cancer Res Clin Oncol. 2010; 136:1117-1124
Seymour RA, Walton G. Effect of malignant disease and treatments on oral structures. Dent Update. 2009; 36:594-603
Markiewicz M, Maragone JE, Campbell JH, Aguirre A. Bisphosphonate-associated osteonecrosis of the jaws. A review of current knowledge. J Am Dent Assoc. 2005; 12:1669-1674
Ruggiero SL, Drew SJ. Osteonecrosis of the jaws and bisphosphonate therapy. J Dent Res. 2007; 86:(11)1013-1021
Johnson GK, Guthmiller JM. The impact of cigarette smoking on periodontal disease and treatment. Periodontol 2000. 2007; 44:178-194
Barker K, Rogers S. Bisphosphonate-associated osteonecrosis of the jaws: a guide for the general dental practitioner. Dent Update. 2006; 33:(5)270-275
Montefusco V, Gay F, Spina F, Miceli R, Maniezzo M, Teresa Ambrosini M Antibiotic prophylaxis before dental procedures may reduce the incidence of osteonecrosis of the jaw in patients with multiple myeloma treated with bisphosphonates. Leukemia Lymphoma. 2008; 49:(11)2156-2162
Moule I, Parsons PA, Irvine GH. Avoiding artefacts in oral biopsies: the punch biopsy versus the incisional biopsy. Br J Oral Maxillofac Surg. 1995; 33:244-247
Lynch DP, Morris LF. The mucosal punch biopsy: indications and technique. J Am Dent Assoc. 1990; 121:145-149
Reid IR, Bolland MJ, Grey AB. Is bisphosphonate associated osteonecrosis of the jaw caused by soft tissue toxicity?. Bone. 2007; 41:318-320
Patel V, McLeod MH, Rogers SN, Brennan PA. Bisphosphonate osteonecrosis of the jaw – a literature review of UK policies versus international policies on bisphosphonates and prevention. Br J Oral Maxillofac Surg. 2011; 49:251-257
Amin M, Glynn F, Phelan S, Sheahan P, Crotty P, McShane D. Silver nitrate cauterisation, does concentration matter?. Clin Otolaryngol. 2007; 32:(3)197-199
Alidaee MR, Taheri A, Mansoori P, Ghodsi SZ. Silver nitrate cautery in aphthous stomatitis: a randomized controlled trial. Br J Dermatol. 2005; 153:521-525
Frost DE, Barkmeier WW, Abrams H. Apthous ulcer – a treatment complication. Oral Surg Oral Med Oral Pathol. 1978; 45:(6)863-869
Sudhindra TV, Joseph A, Hacking CJ, Haray PN. Are surgeons aware of the dangers of diathermy?. Ann R Coll Surg Engl. 2000; 82:(1)31-32
Bashetty K, Nadig G, Kapoor S. Electrosurgery in aesthetic and restorative dentistry: a literature review and case reports. J Conserv Dent. 2009; 12:(4)139-144
Oliver RJ, Sloan P, Pemberton MN. Oral biopsies: methods and applications. Br Dent J. 2004; 196:329-333
Case report: beware the silver nitrate stick – a risk factor for bisphosphonate-related osteonecrosis of the jaw (BRONJ) Michelle C de Souza Gabriela Stepavoi Dental Update 2024 42:8, 707-709.
Authors
Michelle Cde Souza
BDS, MJDF RCS(Eng)
Specialty Doctor in Oral and Maxillofacial Surgery, Oral and Maxillofacial Surgery Department, Princess Alexandra Wing, Kingston Hospital, Surrey, KT2 7QB, UK
Associate Specialist in Oral and Maxillofacial Surgery, Oral and Maxillofacial Surgery Department, Princess Alexandra Wing, Kingston Hospital, Surrey, KT2 7QB, UK
Topical silver nitrate may be used in oral and maxillofacial clinical settings owing to its astringent, caustic and disinfectant properties. Uses of the toughened silver nitrate pencil stick include haemostasis at bleeding points and for the management of aphthous ulcers, hypergranulation tissue, warts and verrucas. We present an interesting case of apparent silver nitrate-induced, bisphosphonate-related osteonecrosis of the hard palate following mucosal lesion biopsy in a multiple myeloma patient receiving zoledronic acid intravenous infusions. Our review of the literature indicates that this is the first report of such a scenario.
CPD/Clinical Relevance: Clinicians must consider all potential sources of chemical and mechanical trauma to the bone and overlying mucosa when managing patients at risk of developing bisphosphonate-related osteonecrosis of the jaw.
Article
Topical silver nitrate, in its toughened pencil stick form (Figure 1), has a wide variety of medical uses in the head and neck region (Table 1). Its caustic nature dictates its cautious use. Overzealous use may result in painful chemical burns of the oral mucous membranes/skin. For the patient on bisphosphonate therapy, this may result in osteonecrosis of the underlying bone.
Figure 1. Typical silver nitrate stick used in UK Oral Surgery departments.
Composition
Typically 75% Silver nitrate* BP (AgNO3) fused with 25% potassium nitrate BP (KNO3) (*also available in 65% and 95% preparations)
Properties
Astringent/styptic (constrictor eg of blood vessels ie haemostatic)Caustic (burns/corrodes/destroys living tissue)Disinfectant (destruction of living organisms)
Uses
Management of hypergranulation tissue, warts and verrucasControl of bleeding points, epistaxisPain relief for aphthous ulcersWound dressings
Adverse Reactions
Dermatologic/mucocutaneous: burning, ulceration and skin irritationArgyria/tattooing (blackened staining of the skin and mucous membranes) – produced by silver depositionEndocrine and metabolic: HyponatremiaHaematologic: Methemoglobinemia
Mechanism of Action
Silver chloride is formed by free silver ions combining with chloride in tissue; bacterial proteins are precipitatedAn eschar (slough of dead tissue) is formed by the coagulation of cellular proteinEffect: growth inhibition of gram positive and gram negative bacteria
Contra-indications
Ophthalmic uses
Advantages
Ease of use (more convenient than surgery or cryotherapy)EconomicalDisposable
Disadvantages
CorrosiveIrritantToxicStaining
Bisphosphonate-related osteonecrosis of the jaw (or BRONJ/BONJ) is defined as a minimum eight-week history of exposed non-vital (necrotic) maxillary/mandibular bone in the absence of a history of radiotherapy to the jaw but in the presence of current or past bisphosphonate therapy (BST).1 It can develop spontaneously or following oral mucosal and/or bony trauma and can be a highly unpleasant and protracted problem for the affected patient. It is now a widely recognized and increasingly documented, though still considered rare, adverse consequence of BST.
Risk of developing BRONJ is higher for those on regular, long-term, high dose and potency intravenous BST2 (0.8–12%, compared to 0.0003–0.06% for oral BST).1 The clinical benefits of intravenous BST for patients with metastatic and osteolytic bone diseases, including multiple myeloma (MM) and hypercalcaemia of malignancy include reduction of bone pain and risk of pathological fracture. Given that no effective clinical treatment currently exists for managing BRONJ, emphasis lies on prevention and minimizing risk of BRONJ development.
The majority of BRONJ described in the literature is as a sequela of dental extraction.3,4 Existing literature reviews use the umbrella term ‘dento-alveolar surgery’ to categorize this local risk factor.1,3,5 The authors feel that this term fails to draw attention to other non-mechanical forms of trauma adequately (eg chemical and thermal forms of trauma), that are often part of dento-alveolar surgery.
MEDLINE and PubMed searches of English literature from 1960 to January 2012 were conducted using the following Medical Subject Headings (MeSH) terms: osteonecrosis, avascular necrosis, bisphosphonates, zoledronic acid, multiple myeloma, silver nitrate, haemostatic agents, chemical trauma. No previously documented cases of silver nitrate use as a risk factor for BRONJ were found. This article introduces a previously undocumented interesting chemical risk factor for BRONJ.
Case report
A 61-year-old carpenter was referred to the oral and maxillofacial department by his GDP in March 2011 regarding an asymptomatic ‘white patch’ on the hard palate. Otherwise unaware of the lesion or any potential causal/precipitating factors, the patient's attention was drawn to the area following an appointment with his hygienist.
Of relevance in his medical history, the patient suffered with multiple myeloma (MM), Stage III IgG Lambda with anaemia, diagnosed 2 years previously. He had skeletal disease at presentation and had been treated with cyclophosphamide, thalidomide and dexamethasone (CTD) chemotherapy and 4 mg intravenous infusions of zoledronic acid, both on a monthly basis. He became intolerant to the CTD chemotherapy after six cycles and was changed to a Velcade-containing chemotherapy regimen (Cyclophosphamide, Velcade, Dexamethasone, CVD), of which he received 5 cycles. Five months later, he underwent an autologous stem cell transplant uneventfully. Since then, no further chemotherapy was given, but he continued with his once monthly zoledronic acid infusions. His bony pains resolved and his peripheral neuropathy was improving slowly.
The patient smoked up to a maximum of 10 cigarettes per day and consumed less than 14 units of alcohol on average per week. He was otherwise a regular dental attender with additional four-monthly hygienist visits. He reported no active dental complaints or recent history of invasive dental treatment (within the previous 2 years).
Clinical examination demonstrated no cervical lymphadenopathy or facial asymmetry. No ‘lesions’ were identified apart from a generalized mild pallor affecting the hard palate. He reported no mucositis and demonstrated good oral hygiene with no obvious hard or soft tissue abnormalities. The patient was reassured, no intervention was advised and a review was organized for two months time.
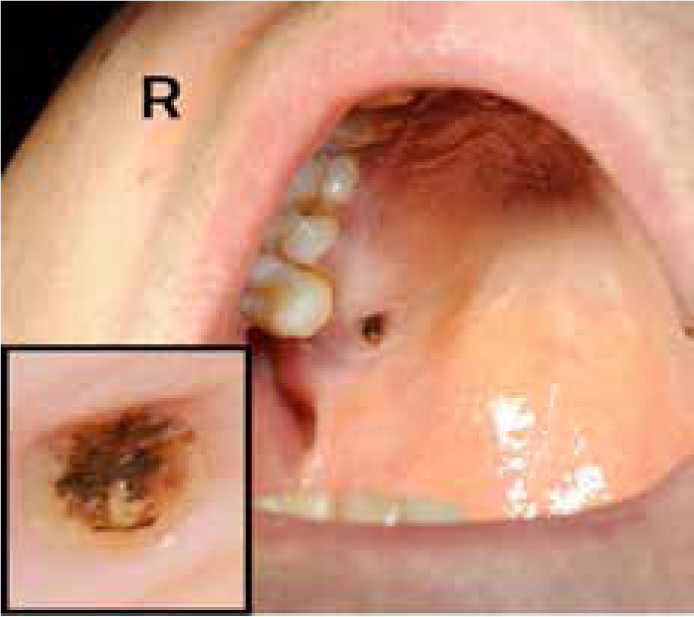
At two month review, a small (approximately 3 mm in diameter), faint, speckled, irregular, non-tender, light brown patch was identified over the right hard palate mucosa approximately 5 mm adjacent to UR6. Provisional diagnosis was that it was a melanocytic macule and an incisional biopsy under local anaesthetic was advised to confirm diagnosis and exclude malignancy.
Approximately 1 ml of 2% lidocaine hydrochloride with adrenaline (1:80 000) was infiltrated through palatal mucosa around the lesion and a 4 mm punch biopsy ring (Figure 2) was used to incise and remove the mucosal lesion. A 4 mm circular defect of exposed bone was left and haemostasis was achieved with a single 75% w/w silver nitrate stick (Figure 1) uneventfully. Standard minor oral surgery verbal and written postoperative instructions were provided with no additional prescription and a review was organized for 6 weeks.
Figure 2. Example of a disposable punch biopsy tool.
At 6 week review, the patient remained asymptomatic but complained of a visible ‘black spot and ridge of gum’, felt with his tongue in the area biopsied, present since biopsy and unchanged in nature. On examination, non-healing of the well-defined circular mucosal punch biopsy defect (approximately 4 mm in diameter) was noted, the margins of which were slightly raised though not tender or inflamed. No bleeding on probing or exudate was seen. The exposed area of bone demonstrated a central blackened area, hard to probe. A clinical diagnosis of BRONJ was suspected and the patient advised. Histopathological analysis of the biopsied mucosa showed squamous mucosa with marked hyperkeratosis and minimal chronic inflammation. He was prescribed a 2-week course of Doxycycline 100 mg twice daily and advised to use chlorhexidine 0.12% mouthwash twice daily. Review was arranged at 2 weeks.
At subsequent 2 week review, little had changed clinically and the patient remained asymptomatic. As 2 months of ‘non-healing’ had elapsed, the bone remaining exposed and ‘necrotic’ in appearance, a diagnosis of BRONJ (Stage 11) was made. Photographs were taken for records with the patient's consent (Figure 3) and his GP and haemato-oncologist informed. Review interval was extended to once monthly, given that he remained asymptomatic and his condition, though apparently non-resolving, was not deteriorating. He was advised to continue twice daily chlorhexidine digluconate 0.12% mouthwashes, ie conservative management.
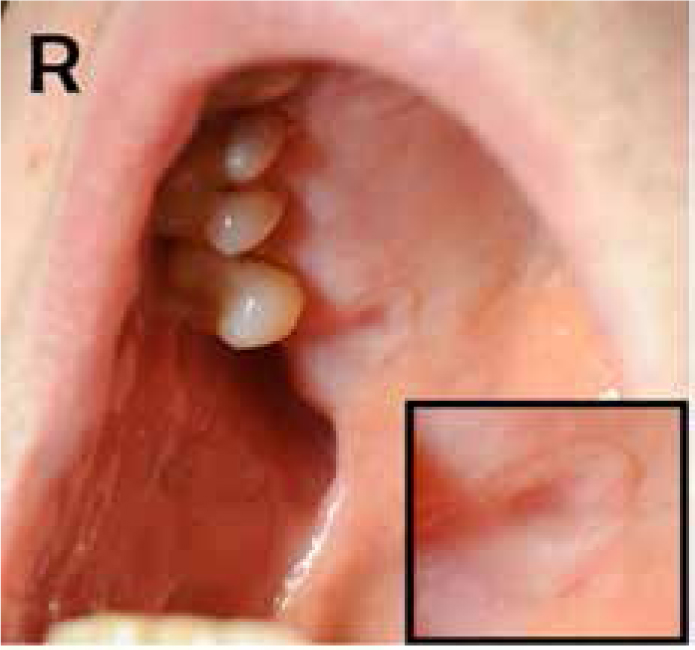
Three months later, 16 weeks post-biopsy, the patient continued to remain asymptomatic. On examination, complete mucosal closure over the bony defect had occurred with a small saucerized depression remaining (Figure 4). The area was non-tender to touch with no evidence of suppuration. Review interval was extended to three monthly and the patient advised to perform local cleaning of the area with chlorhexidine digluconate 0.12% mouthwash soaked cotton bud twice daily. His haemato-oncologist advised an increase in interval between zoledronic acid infusions to four-monthly given his multiple myeloma was in haematological remission (stable paraprotein levels at 2g/L since October 2011).
Figure 4. Evidence of healing at 16-week review post-biopsy.
At review, 36 weeks post-biopsy (February 2012), continued resolution of the area was noted with a reduction in the appearance of the saucerized depression centrally (Figure 5). The overlying mucosa remained healthy and non-tender to the touch. The patient described being aware of the ‘ridge of gum’ disappearing a month earlier.
Figure 5. Near complete healing at 36 weeks postbiopsy review.
Final review, three months later, demonstrated continued healing with further resolution of the saucerized mucosal depression. The patient remained asymptomatic, was reassured and discharged.
Discussion
The authors believe this case to be the first highlighting the risk of developing BRONJ following use of silver nitrate in the oral cavity for patients with a history of BST. Cases of osteonecrosis secondary to indirect and direct trauma from other chemicals, in the absence of a history of BST, have already been documented.6,7,8
Categorizing BRONJ risk
The patient described in this case was at particularly high risk of developing BRONJ given that he had been receiving monthly intravenous infusions of zoledronic acid (a potent nitrogen-containing bisphosphonate) for nearly 24 months at the time of presentation.1,9 A study by Filleul et al, over a six-year period, found that nearly 90% of 2400 BRONJ patients reviewed had received zoledronic acid infusions as part of treatment for their malignancy.10 Other compounding risk factors, specific to our patient, included his age (over 60 years old), underlying malignancy (MM), immunosuppression (from the chemotherapy) and concomitant long-term steroid therapy (daily dexamethasone).1,11,12 As a smoker, the nicotine in smoke is a vasoconstrictor11 and anti-angiogenic (as is zoledronic acid13 and the thalidomide in CTD therapy). It can also destroy soft tissues and impair bony healing.14
Minimizing BRONJ risk
Given this knowledge above, the authors pose two important questions relating to the management of this patient. First, did the benefit of conducting a biopsy (of a non-sinister lesion) outweigh the risk of developing BRONJ? Secondly, what if anything could have been done to prevent the development of BRONJ based on the available evidence base?
The authors stand by their decision to confirm diagnosis through biopsy as this remains the only true way of ascertaining histopathology. As regards preventive measures, no pre-/peri- or post-operative antibiotic therapy or mouthwash was provided at the time of biopsy. The patient was not undergoing chemotherapy at this time. No robust evidence currently exists to support the use of antibiotic prophylaxis for invasive dental procedures to prevent BRONJ.2 Opinion on this, however, is divided and variation in recommendations to use pre- and/or post-operative chlorhexidine digluconate 0.12% mouthwash and/or antibiotics exist.5,15,16 Furthermore, the choice of antibiotic may depend on results of culture, patient tolerance and duration of the problem. Tetracycline therapy (eg doxycycline) is well tolerated in the long term if required and demonstrates good bony uptake, hence its use in this case. Doxycycline (100 mg OD) or Penicillin V (500 mg QDS) would be appropriate antibiotic regimens, given that most pathogens isolated in BRONJ are actinomyces, eikenella and moraxella species.2
Analysis of clinical intervention
Knowing that dento-alveolar surgery is a well documented risk factor for BRONJ,1 the authors consider the method of biopsy technique. Did the BRONJ develop as a result of mechanical trauma from the punch biopsy itself or through chemical insult from the silver nitrate used to cauterize bleeding points?
The punch biopsy technique is frequently used in oral medicine/surgery and dermatology settings. It is easy, inexpensive, safe and quick to use. It comprises a cylindrical blade (like a pastry cutter), whose diameter comes in sizes between 2 and 10 millimetres attached to a plastic handle (Figure 2). A core of tissue is cut by applying the punch at a right angle to the mucosa, entering into the tissues by continuous rotation under medium pressure. The tissue specimen is removed and the base released using a scalpel or curved scissors. It is considered an atraumatic technique producing fewer artefacts under histopathological examination than standard incisional biopsy technique. The residual defect is small and can be left unsutured.17,18
Local release of bone-incorporated bisphosphonate, secondary to intra-oral trauma, has been proposed to inhibit epithelial cell proliferation, thereby delaying soft tissue healing and increasing exposure time of the underlying bone to micro-organisms of the oral cavity.2,19. Perhaps therefore, a shallower biopsy to avoid bony exposure may have been preferential, although this in turn may have compromised the sample and made it less representative. Primary closure of the soft tissues of the hard palate with sutures is ideal to help protect underlying bone and forming a blood clot.11,20 In reality this can be difficult to achieve owing to their lack of elasticity.
If primary closure and the haemostasis it creates are not possible, other methods of achieving haemostasis in the hard palate region must also be considered carefully in the BRONJ susceptible patient. MM patients may be at higher risk of intra-oral bleeding if they are thrombocytopenic as a consequence of plasma cell proliferation in the bone marrow. Therefore, the need for good haemostasis at the time of surgery is even more important.
In our case report, a junior grade clinician (senior house officer) performed the procedure and overzealous/incorrect use of the silver nitrate stick may have occurred. Silver nitrate applicator sticks should be applied carefully and directly in light and small rotational movements to dampened lesions. This allows dissolution of the chemical and adequate concentration to be reached. Topical silver nitrate of 95% concentration has shown double the penetration depth of its 75% concentration equivalent when used on tonsillar mucosal tissue in a nasal cautery study.21 Perhaps, therefore, use of the lowest concentration (65%) available in applicator stick form may have been prudent. However, this does not detract from the fact that, irrespective of concentration, silver nitrate is caustic and can increase the depth of injury in tissues to which it is applied.22 Even its minimal use could produce sufficient chemical trauma to trigger BRONJ. Marked spreading local necrosis of the tongue has been reported following single topical application of an aphthous ulcer with a toughened (25% potassium nitrate) 75% silver nitrate stick.23 Thus the authors propose the use of silver nitrate in the oral cavity to be absolutely contra-indicated for patients with a history of BST, irrespective of the experience level of the clinician handling the substance and concentration of silver nitrate used.
Alternatives for achieving haemostasis
These include electrocautery and the application of a temporary sterile dressing pack, with or without holding sutures or cover plate. For a small biopsy of the palate, the authors consider whether simple gauze pressure with a haemostatic agent, such as tranexamic acid, may be adequate if bleeding is minimal.
Electrocautery
Surgical diathermy or electrosurgery/cautery is often used in oral and maxillofacial surgery for the cutting (‘dry incision’) and coagulation (haemostasis) of soft tissues. An electric current excites tissue molecules to produce heat, causing cellular explosion followed by tissue division and cellular desiccation with blood protein coagulation, respectively. A study by Sudhindra et al found clinicians at all levels and across multiple specialties to have significant lack of knowledge regarding the use of surgical diathermy equipment.24 Of the two modes of diathermy, bipolar diathermy is safer and produces less tissue damage than monopolar diathermy. Use of monopolar diathermy in periodontal surgery has dropped significantly owing to reports of soft and hard tissue necrosis.25 The authors have found no literature to support or refute the safe use of bipolar diathermy for soft tissue bleeding points in the BRONJ susceptible patient.
Dressing/pack placement
The secure placement of a non eugenol-containing periodontal dressing paste (eg CoePak™) or sterile pre-soaked gauze pack (eg betadine-soaked gauze, bismuth iodoform paraffin paste BIPP-impregnated gauze) with sutures or a pre-fabricated custom-made cover plate for the larger palatal biopsy has its uses.26 Unfortunately, again, no literature exists to support its use in preventing BRONJ.
The authors feel that, although a number of patient and operator factors were at play in the development of BRONJ for this patient, the causticity of the silver nitrate coupled with the potential/actual bony exposure created in performing mucosal biopsy of the hard palate were significant triggers.
Management of quiescent BRONJ
The therapeutic aims of managing BRONJ are to eliminate pain, control infection and minimize further disease progression. Fortunately, our patient remained asymptomatic throughout with no clinical signs of infection or disease progression (eg pain, swelling, suppuration, etc) and so conservative management was followed. The effect of the patient's haemato-oncologist's decision to increase the interval between zoledronic acid infusions from 2–4 monthly from the point of BRONJ diagnosis on the rate of BRONJ resolution cannot be correlated. The effects of dose reduction, interval extension and/or a drug holiday altogether on an established BRONJ are unclear as data is lacking.27 It has been postulated that a drug holiday may help stabilize and reduce the appearance of established BRONJ;1 this is providing the patient's systemic condition allows for discontinuation of BST.
Conclusion
The use of topical silver nitrate in the oral cavity should be contra-indicated in BRONJ-susceptible patients and in the hands of inexperienced clinicians.
There is a need to consider the implications of all forms of potential soft and hard tissue trauma (mechanical, chemical, thermal, etc) when managing patients on BST.
The category of risk for development of BRONJ must be assessed for individual patients as this will influence approach to treatment.
All members of the clinical team (including junior grades) must ensure up to date awareness of the issues and developments surrounding the causes, prevention and management of BRONJ and identification of susceptible patients.
Liaison between specialties (eg oncologists and dentists) is essential to prevent BRONJ.