McGurk M, Escudier MP, Thomas BL, Brown JE. A revolution in the management of obstructive salivary gland disease. Dent Update. 2006; 33:28-36
Cawson R, Odell EW. Cawson's Essential of Oral Pathology and Oral Medicine, 9th edn. : Elsevier; 2017
Leung A, Choi M, Wagner G. Multiple sialoliths and a sialolith of unusual size in the submandibular duct. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999; 87:331-333
McGurk M, Escudier M, Brown J. Modern management of salivary calculi. Br J Surg. 2005; 91:107-112
Goncalves M, Schapher M, Iro H Value of sonography in the diagnosis of sialolithiasis: comparison with the reference standard of direct stone identification. J Ultrasound Med. 2017; 36:2227-2235
Cordesmeyer R, Winterhoff J, Kauffmann P, Laskawi R. Sialoendoscopy as a diagnostic and therapeutic option for obstructive diseases of the large salivary glands—a retrospective analysis. Clin Oral Invest. 2016; 20:1065-1070
Dulguerov P, Marchai F, Lehmann W. Postparotidectomy facial nerve paralysis: possible etiologic factors and results with routine facial nerve monitoring. Laryngoscope. 1999; 109:754-762
Raad I, Sabbagh M, Caranasos G. Acute bacterial sialadenitis: a study of 29 cases and review. Clin Infect Dis. 1990; 12:591-601
Su S, Chang H, Chen K. Current status of mumps virus infection: epidemiology, pathogenesis, and vaccine. Int J Environ Res Public Health. 2020; 17
Aasheim ET, Inns T, Trindall A Outbreak of mumps in a school setting, United Kingdom, 2013. Hum Vaccin Immunother. 2014; 10:2446-2449
Hviid A, Rubin S, Mühlemann K. Mumps. Lancet. 2008; 371:932-944
Scully C, Bagán J, Eveson J Sialosis: 35 cases of persistent parotid swelling from two countries. Br J Oral Maxillofac Surg. 2008; 46:468-472
Scully C, Porter S. Orofacial disease: update for the clinical team: 9. Orofacial pain. Dent Update. 1999; 26:410-417
Voulgarelis M, Dafni U, Isenberg D, Moutsopoulos H. Malignant lymphoma in primary Sjogren's syndrome: a multicenter, retrospective, clinical study by the European concerted action on Sjogren's syndrome. Arthritis Rheum. 1999; 42:1765-1772
Felix D, Luker J, Scully C. Oral medicine: 4. Dry mouth and disorders of salivation. Dent Update. 2012; 39:738-743
Scully C. Drug effects on salivary glands: dry mouth. Oral Dis. 2003; 9:165-176
Lakraj A, Moghimi N, Jabbari B. Sialorrhea: anatomy, pathophysiology and treatment with emphasis on the role of botulinum toxins. Toxins. 2013; 5:1010-1031
Mozaffari H, Ramezani M, Janbakhsh A, Sadeghi M. Malignant salivary gland tumors and Epstein–Barr virus (EBV) infection: a systematic review and meta-analysis. Asian Pac J Cancer Prev. 2017; 18:1201-1206
Dong C, Hemminki K. Second primary neoplasms among 53,159 haematolymphoproliferative malignancy patients in Sweden, 1958–1996: a search for common mechanisms. Br J Cancer. 2001; 85:997-1005
Shebl F, Bhatia K, Engels E. Salivary gland and nasopharyngeal cancers in individuals with acquired immunodeficiency syndrome in United States. Int J Cancer. 2010; 126:2503-2508
Sood S, McGurk M, Vaz F. Management of salivary gland tumours: United Kingdom national multidisciplinary guidelines. J Laryngol Otol. 2016; 130:(S2)S142-S149
To V, Chan J, Tsang R, Wei W. Review of salivary gland neoplasms. ISRN Otolaryngol. 2012:1-6
Millsop JW, Wang EA, Fazel N. Etiology, evaluation, and management of xerostomia. Clin Dermatol. 2017; 35:468-476
An overview of the diagnosis and management of non-neoplastic salivary gland pathologies Neel Sethi Alessandra Joelle Booth Nikul Patel Graham Merrick Dental Update 2024 49:5, 707-709.
Salivary gland pathologies can be caused by obstruction, inflammation, bacterial or viral infections and neoplasia. Patients can present with acute or chronic presentations of salivary gland disease. Salivary gland disorders can have a significant impact on a patient's systemic health, oral health and quality of life. This article aims to increase awareness of salivary gland pathologies and how they may present in practice. It aims to offer general dental practitioners an understanding of how salivary gland disease can be managed in primary care and which conditions may warrant referral to secondary care, including suspected malignancy. The dental profession has a duty of care to recognize pathologies and treat or refer patients. This article provides an overview of non-neoplastic salivary gland disease, including diagnoses, management and when to refer to secondary care.
CPD/Clinical Relevance: It is important to understand the signs, symptoms and management of non-neoplastic salivary gland diseases, and when to refer patients to secondary care.
Article
Salivary glands are vital to the maintenance of good oral health. They are exocrine glands that produce saliva, which is essential to ensure lubrication of the oral cavity, aid in the digestion of food and act as a buffer to protect the teeth. Anatomically, there are three pairs of major salivary glands, the parotid, submandibular and sublingual glands. Minor salivary glands are numerous and can be found throughout the mucosa lining the oral cavity with the exception of the gingiva. Salivary gland disease can present as a range of pathologies from stones, obstructions and infections through to benign or malignant tumours. This article focuses on non-neoplastic salivary gland pathologies, their diagnosis, management and the role of the general dental practitioner (GDP) in managing patients with salivary gland disease.
Obstructive salivary disease
Obstructive salivary gland disease is the most common salivary gland pathology to present to general dental practitioners.1 Patients suffering from obstructive salivary disease may complain of intermittent pain and swelling. There are two patterns. The first is related to a stone that presents classically as an acute swelling at meal times. This is typically intermittent and generally resolves over a 30-minute period after eating, as saliva gently oozes past the stone. The second is obstruction by a mucous plug, which tends to happen at breakfast or after a patient has become dehydrated, that can lead to sluggish saliva flow and plug formation. Commonly known as ‘mealtime syndrome,’ saliva production stimulated by the process or thought of eating causes a build-up of saliva in the affected gland and consequential postprandial swelling. In addition to this, after a period, patients with stones may experience repeated episodes of bacterial infections causing suppuration from the gland duct opening and possible systemic symptoms of fever and malaise. Mucous plugs seldom cause infection.
The most common cause for obstruction is sialolithiasis. These are saliva stones consisting of calcium, magnesium, potassium and ammonium deposits. The majority of these cases occur unilaterally in one of the submandibular glands. Sialolithiasis is most commonly seen in males2 and is thought to affect 12 in 1000 adults,3 rarely affecting children.
Around 94.2% of sialoliths in the submandibular gland, and 43.3% in the parotid gland, are radiopaque,4 therefore standard radiographs (Figure 1) and computer tomography can be of diagnostic value. Ultrasound sonography has been shown to be beneficial in locating stones in the hands of experienced radiographers.5 Sialoendoscopy is being increasingly used both to diagnose and treat sialoliths.6
Figure 1. Radiograph of submandibular sialolith.
Management techniques for sialoliths vary depending on the size and location of the stone. In the past, there were very few treatment options available for the management of obstructive salivary gland disease, and the main surgical treatment involved the removal of the associated gland. However, using modern techniques, it has now been shown that over 70% of stones can be retrieved, and only a minority of glands require removal.4 Minimally invasive techniques include extra-corporeal shockwave lithotripsy, radiologically guided basket retrieval, balloon dilation and intra-oral stone removal.1 Surgical removal is a well-documented technique for removing larger stones. Interventional radiography such as fluoroscopy-guided basket removal can be used to locate and retrieve stones within a duct.
In some cases, a sialadenectomy (surgical excision of the affected salivary gland) may be required, but this is not without the risk of paralysis of the marginal mandibular nerve in the case of the submandibular gland or the facial nerve when treating the parotid gland. Cases that may warrant a sialadenectomy include multiple stones within the duct, stones that have adhered to the duct wall, recurrent sialoliths, large stones within the gland itself or previous failed attempts at retrieval of a stone.7
Sialadenitis
Infections within the salivary glands most commonly occur in the parotid. Acute bacterial ascending sialadenitis is predominantly caused by Staphylococcus aureus.8 Traditionally, it was related to patients with a decreased salivary flow rate, such as in older persons or those with chronic dehydration, but this is uncommon now, and it is normally associated with obstruction by a stone. Usually, sialadenitis presents as diffuse pain and swelling around the gland. Massaging of the gland may expel suppuration from the duct opening. Occasionally, the infections can be severe and patients may present with systemic signs of infection, such as pyrexia or malaise. Management of the condition involves antibiotics, surgical release of pus if present, and removal of the obstructing stone. Patient education to encourage hydration, self-massage of the gland and consumption of saliva-stimulating foods, such as citric acid, can be beneficial.
Mucoceles
Mucoceles present as rounded, localized blue-transparent swellings on the oral mucosa caused by an alteration in a minor salivary gland leading to the accumulation of mucous. While they can occur on any oral mucosa containing minor salivary glands, they are most commonly seen on the lower lip and can be linked to trauma, lip biting habits or iatrogenic causes (Figure 2). These are predominantly mucous extravasation cysts induced by trauma to a minor salivary duct, and the subsequent pumping of saliva into the loose surrounding connective tissue (hence why they do not occur on the hard palate). Minor salivary glands have the unique capacity to secrete against pressure.
Figure 2. Lower lip mucocele.
Ranulas describe extravasation cysts of the sublingual gland that predominantly present as a cystic swelling in the floor of the mouth. They have the potential to become plunging ranulas in instances where the saliva passes through the mylohyoid muscles and extend down into the neck.
Diagnosis of mucoceles is usually based on clinical presentation and excisional biopsy. Fine needle aspiration can be used. Aspirate of amylase and high-protein content would confirm the presence of saliva, and the diagnosis of a mucocele, but observing a thick sticky liquid is pathognomonic of this condition.
Mucoceles are occasionally self-limiting and may go through periods of relapse and recurrence, but normally persist and have to be removed. Correcting the aetiology if trauma is a contributing factor through removing sharp restorations or addressing lip biting habits will aid this process.
Simple incision of the mucocele often leads to recurrence because the excess mucous is drained, but the affected salivary gland remains. Surgical excision, along with the affected saliva gland, is the conventional treatment of choice. However, patients need to be warned of the risk of recurrence, or numbness from injury to small branches of the mental nerve.
Mumps
Mumps is an infectious viral disease that causes swelling of the parotid glands caused by a virus from the paramyxovirus family. Symptoms usually present as bilateral swelling of the parotids accompanied by systemic signs such as pyrexia, fatigue and malaise. Although the mumps, measles and rubella vaccine (MMR) has decreased the incidence of the virus,9 those who are vaccinated can still develop the disease and the UK has seen local outbreaks.10 While rare, complications include orchitis, encephalitis, pancreatitis and myocarditis.11
Diagnosis is usually determined clinically, however. Laboratory diagnosis can be made from a saliva sample using immunofluorescence staining or PCR to test for the presence of the virus, or serological testing to look for virus-specific antibodies.11
The management for mumps is predominantly supportive therapy through regular analgesics, promoting hydration and bed rest. Further medical intervention should be sought to confirm diagnosis and monitor for complications.
Systemic disease
Salivary gland pathology can present as a manifestation of systemic disease. Usually these present as diffuse, non-inflammatory swellings of the major salivary glands. The most common cause of sialosis is diabetes mellitus and alcoholism.12 Other possible causes to investigate include HIV, hepatis C and sarcoidosis.
Xerostomia
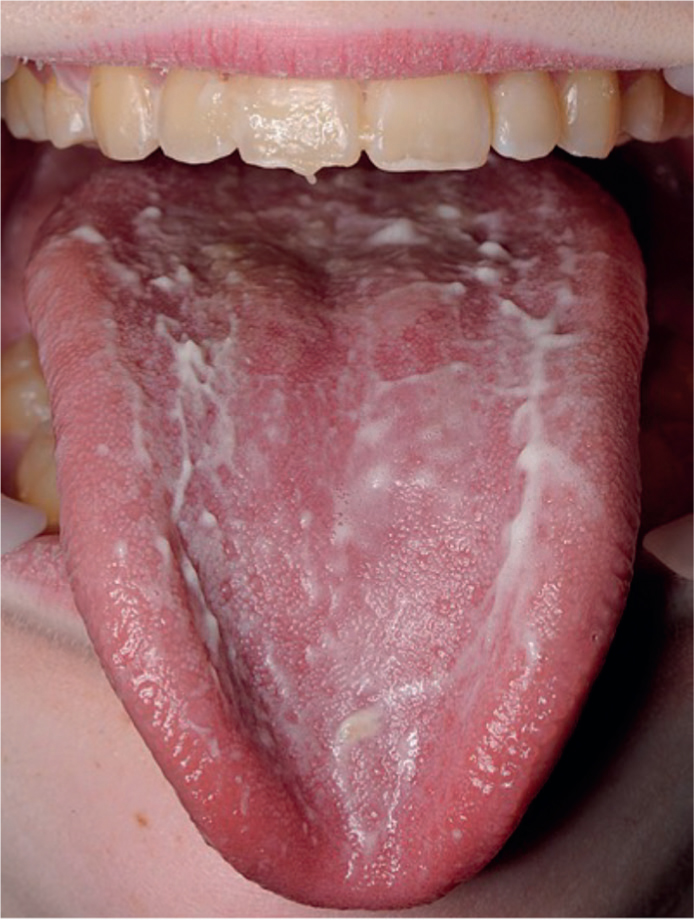
Xerostomia is the sensation of a dry mouth due to either a reduction in the quantity of saliva produced, or the composition of saliva (Figure 3). Dry mouth can impact a patient's speech, ability to chew, eat, swallow and wear dentures. Drugs are the most common cause of a reduction in salivary flow.13 This is becoming a growing problem among those who are older due to the high prevalence of polypharmacy. Some of the other causes of xerostomia are outlined in Table 1.
Figure 3. Frothy saliva resulting from xerostomia.
Table 1. A list of some of the causes of xerostomia. Based on a figure by Millsop et al.25
Sjogren's Syndrome
IgG4
Thyroid disease
Scleroderma
Sarcoidosis
Tuberculosis
Ectodermal dysplasia
Parkinson disease
Primary biliary cirrhosis
Graft vs host disease
Medication
Head and neck radiotherapy
Diabetes mellitus
HIV
Hepatitis C
Renal disease
Dehydration
Alcohol intake
Tobacco use
Several questionnaires have been developed that can indicate whether a patient is suffering from a dry mouth. This, alongside a thorough medical history assessing which medications a patient is taking, whether they have any systemic diseases and if they have had a history of radiation to the head and neck can determine potential causes for xerostomia. Additionally, a clinical examination, such as sialometry, can determine the severity of a patient's xerostomia.
Sjogren's syndrome (SS) is an autoimmune condition, which, when it develops in isolation of any rheumatic disease, is known as primary SS. Patients with primary SS are at a higher risk of developing non-Hodgkin's lymphoma and may require more frequent monitoring and regular recall intervals.14 However, secondary SS is more common and linked to other autoimmune diseases, such as rheumatoid arthritis or systemic lupus erythematosus. Diagnosis involves saliva flow rate, blood tests (specifically antinuclear antibodies Ro and La, rheumatoid factor and erythrocyte sedimentation rate), Schirmer test (a measure of tear production), ultrasound scans and labial salivary gland biopsy.15
The management for xerostomia involves advising patients to take frequent sips of water, sugar-free chewing gum, diabetic sweets, cholinergic drugs (eg pilocarpine), avoid dry, sharp, acidic or citrus foods and prescribing saliva replacements, which come in a range of modalities, such as sprays, gels and lozenges. Reduced saliva flow predisposes patients to an increased risk of dental decay. Due to this, GDPs should consider shorter recall intervals, fluoride varnish applications, high-fluoride toothpaste, diet education and oral hygiene advice.16 Patients should also be informed of common habits that may further exacerbate symptoms of a dry mouth, including alcohol, smoking and caffeinated beverages.17 Patients are also at a higher risk of developing oral candidiasis and sialadenitis, so should be educated about the symptoms of these and treated accordingly by the GDP.
Sialorrhea
While true hypersalivation is uncommon, sialorrhea can impact the quality of life of patients with neurodegenerative disorders such as Parkinson's disease. If left untreated, it can lead to reduced social functioning, skin breakdown, infection or aspiration. True sialorrhea is due to hypersalivation, usually linked to medication such as clozapine. Pseudo causes of sialorrhea result from the inability to clear saliva from the oral cavity, such as in conditions that impair a patient's ability to swallow, for example motor neurone disease. Management includes oral-motor exercises, anticholinergic medication, botulinum toxin injections or, in more severe cases, surgical intervention through gland excision, denervation of glands or redirection of saliva duct openings.18
Neoplasia
While infrequent, salivary gland tumours can occur in the minor or major salivary glands and be either benign or malignant. Malignant major salivary gland disease accounts for 6% of all head and neck cancers in the UK, and the incidence of major salivary gland malignancy is increasing.19 Most commonly, salivary gland tumours are found within the parotid gland, the majority of which are benign. In contrast to this, while less common, tumours in the minor salivary glands carry a much higher risk of malignancy.
While the aetiology remains unclear, although rare, certain factors have been shown to increase the risk of developing a salivary gland neoplasm, for example, previous head and neck radiation, Epstein–Barr virus,20 Hodgkin lymphoma,21 and immunosuppression (acquired immunodeficiency disease).22 Some benign salivary gland tumours, such as a pleomorphic adenoma (Figure 4), have a small malignant transformation risk.23 Carcinoma ex pleomorphic adenoma occurs from either a primary or recurrent benign pleomorphic adenoma.23
Figure 4. A parotid swelling, which in this instance was diagnosed as pleomorphic adenoma.
Features that should alert the clinician to suspected malignancy include: a rapid growing mass, any unexplained lump or swelling, fixation of the tumour to underlying tissues, increasing pain, unexplained ulceration and cervical lymphadenopathy. Salivary gland neoplasms affecting the parotid or submandibular glands may impinge on the facial nerve and cause ipsilateral facial nerve weakness or paralysis. If a patient presents with any of the above symptoms, it is imperative that they are referred appropriately via a suspected cancer 2-week wait pathway. The main treatment of choice for salivary gland tumours is excision with or without adjunctive radiotherapy.24,25
Summary
Salivary gland pathology is a common presentation to the GDP. In order for these patients to be appropriately managed, clinicians must have a good understanding of their presentation and treatment. It is imperative that thorough extra- and intra-oral clinical examinations are undertaken for all patients. If required, further investigations and management should be undertaken in primary care. Although the majority of salivary gland conditions are benign, it is essential that patients are referred to a secondary care or specialist service on a 2-week wait referral pathway when malignancy is suspected.