Manfredi M, Polonelli L, Aguirre-Urizar JM, Carozzo M, McCullough MJ. Urban legends series: oral candidosis. Oral Dis. 2013; 19:245-261
Falagas ME, Roussos N, Vardakas KZ. Relative frequency of albicans and the various non-albicans Candida spp among candidemia isolates from patients in various parts of the world: a systematic review. Int J Infect Dis. 2010; 14:e945-e966
Williams D, Lewis M. Pathogenesis and treatment of oral candidosis. J Oral Microbiol. 2011; 28
Ellepola ANB, Samaranayake LP. Inhalational and topical steroids, and oral candidosis: a mini review. Oral Dis. 2001; 7:211-216
Knight L, Fletcher J. Growth of Candida albicans in saliva: stimulation by glucose associated with antibiotics, corticosteroids and diabetes mellitus. J Inf Dis. 1971; 123:371-377
Hibino K, Wong R, Hagg U, Samaranayake LP. The effects of orthodontic appliances on Candida in the human mouth. Int J Paed Dent. 2009; 19:301-308
Bessa CN, Santos PB, Aguiar MF, V do Carma MA. Prevalence of oral mucosal alterations in children from 0 to 12 years old. J Oral Pathol Med. 2004; 33:17-22
Darwazeh AG, Al-Bashir A. Oral candida flora in healthy infants. J Oral Pathol Med. 1995; 24:361-364
Sag C, Ozden FO, Acikgoz G, Anlar FY. The effects of combination treatment with a long-acting beta2-agonist and a corticosteroid on salivary flow rate, secretory immunoglobulin A and oral health in children and adolescents with moderate asthma: a 1-month, single blind clinical study. Clin Ther. 2007; 29:2236-2242
Epstein JB. Oral complications of cancer and cancer therapy: from cancer treatment to survivorship. CA Cancer J Clinic. 2012; 62:400-422
Leggot P. Oral complications in the pediatric population. NCI Monographs. 1990; 9:129-131
Iro H, Zenk J. Salivary gland diseases in children. Curr Topics Otolaryngol Head Neck Surg. 2014; 13:1-30
Soysa NS, Samaranayake LP, Ellepola AB. Diabetes mellitus as a contributory factor in oral candidosis. Diabet Med. 2005; 23:455-459
Kadir T, Pisiriciler R, Akyuz S, Yarat A, Emekli N, Ipbuker A. Mycological and cytological examination of oral candida carriage in diabetic patients and non-diabetic control subjects: thorough analysis of local aetiologic and systemic factors. J Oral Rehab. 2002; 29:452-457
Rozeli M, Esther G, Claudete R. Oral manifestations of diabetes mellitus in controlled and uncontrolled patients. Braz Dent J. 1995; 6:131-136
Brownlee M, Cerami A, Vlassara H. Advanced glycosylation end products in tissue and the biochemical basis of diabetic complications. N Engl J Med. 1988; 318:1315-1321
Cortes-Ramirez J, Cortes Ayala C Oral alterations in children with cancer. Literature review. J Oral Res. 2014; 3:262-268
Belfield PM, Dwyer AA. Oral complications of childhood cancer and its treatment: current best practice. Eur J Cancer. 2004; 40:1035-1041
Ramos-Gomez FJ, Flaitz C, Catapano P, Murray P, Milnes AR, Dorenbaum A. Classification, diagnostic criteria, and treatment recommendations for orofacial manifestations in HIV-infected pediatric patients. Collaborative Workgroup on Oral Manifestations of Pediatric HIV Infection. J Clin Pediatr Dent. 1999; 23:85-96
Pinheiro R, Franca T, Ribeiro C, Leao J, De Souza I, Castro G. Oral manifestations in human immunodeficiency virus infected children in highly active antiretroviral therapy era. J Oral Pathol Med. 2009; 38:613-622
Niimi M, Firth N, Cannon R. Antifungal drug resistance of oral fungi. Odontology. 2010; 98:15-25
Oral candidosis can present in childhood with recognizable mucosal changes. It may be associated with predisposing factors or suggest underlying systemic disease such as poorly controlled diabetes or an immunosuppressed state. Investigations are often required and management includes addressing predisposing factors in addition to prescribing topical or systemic antifungal therapy.
CPD/Clinical Relevance: It is important for general dental practitioners to recognize oral mucosal changes related to candidal infection and refer to secondary care for further assessment when appropriate.
Article
Candida albicans is the most common candida species isolated from the oral cavity in both healthy and diseased states.1 However, there has been an increase in the incidence of non-albicans species such as C. glabrata, C. tropicalis and C. krusei in recent years.2
It is important to differentiate between candida as a commensal and candida infection (candidosis). Commensal oral carriage of candida can occur in up to 80% of healthy individuals.3 Progression from harmless commensal to pathogenic organism is often due to predisposing host factors which often relate to a weakening of host immune defences.3 In the paediatric setting it is important to consider these predisposing factors as oral candidosis may reflect an undiagnosed systemic condition.
Predisposing factors
Factors that predispose to oral candidosis relate primarily to the host. The virulence factors unique to Candida albicans which allow it to colonize the oral mucosal surface so effectively are listed in Table 1.
Cell wall proteins (adhesins) that interact with mucosal epithelial cells and increase adherence;
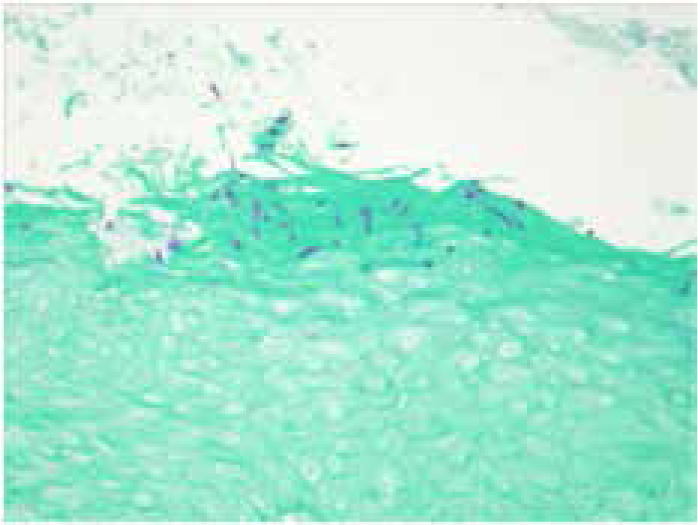
Ability to produce hyphae (Figure 1) which allows deeper invasion of the oral mucosa;
Phenotype switching which allows a change of morphology and evasion of host immune mechanisms;
Secretion of proteolytic and lipolytic enzymes which assist with mucosal invasion and destruction of secretory IgA.
Figure 1. Oral mucosa showing candidal hyphae.
The factors relevant in the paediatric setting include:
Local factors
Reduced salivary flow;
Use of inhaled steroids;
Dental appliances.
Systemic factors
Diabetes mellitus;
Immunosuppression;
Nutritional deficiencies.
Iatrogenic factors
Use of broad spectrum antibiotics;
Corticosteroid use;
Radiotherapy;
Chemotherapy.
Classification
Oral candidosis can be classified as primary, confined to the oral cavity alone, and secondary, where lesions affect both oral and extra-oral sites (Table 2).4
Primary Oral Candidosis
Secondary Oral Candidosis
The primary triadPseudomembranousErythematous (acute or chronic)Chronic hyperplasticCandida-associated lesionsDenture-related stomatitisAngular cheilitisMedian rhomboid glossitisLinear gingival erythema
This condition is often referred to as ‘oral thrush’ and is a common form of oral candidosis in newborns and the elderly. It presents as creamy white plaques, often said to resemble milk curds, which most commonly affect the soft palate, tongue and buccal mucosa (Figure 2). A feature of pseudomembranous candidosis is that these plaques can be removed with gauze, leaving an erythematous, and sometimes bleeding, mucosal surface.3 It affects up to 5% of newborns, at any time during the first few weeks of life, as a result of a newborn's immature immune system and vertical transmission during the passage through the birth canal.5
Figure 2. Pseudomembranous candidosis of palate.
Predisposing factors include the use of inhaled or topical corticosteroid or immunosuppression, most notably human immunodeficiency virus (HIV) infection. It normally presents acutely with minimal symptoms but, in cases of long-term immunosuppression, a chronic pseudomembranous candidosis can develop with an associated risk of oesophageal and respiratory involvement.6
Acute and chronic erythematous candidosis
Acute erythematous candidosis most commonly occurs acutely after the use of broad spectrum antibacterials when the normal bacterial flora of the mouth is altered allowing fungal overgrowth. Sites affected include the buccal mucosa, dorsal tongue and palate. It resolves spontaneously after the antibacterials are discontinued. Other causes include the use of inhaled corticosteroids. It is reported that erythematous candidosis is the only form of candidosis that is consistently painful.3
Chronic erythematous candidosis is most commonly seen in patients with removable appliances, such as dentures or orthodontic appliances (Figure 3). This presents as areas of erythema in relation to the fitting surfaces of the appliances, particularly if these are not removed regularly and/or if oral and appliance hygiene are poor.
Figure 3. Chronic erythematous candidosis affecting the hard palate.
Chronic hyperplastic candidosis
This does not typically occur in the paediatric setting. It presents as a persistent white lesion which may have associated erythema and which is not removable (Figure 4). It most commonly affects the commissures, though any site can be involved.
Figure 4. Chronic hyperplastic candidosis right commissure.
Angular cheilitis
Angular chelitis is classified as a candida-associated lesion, as other factors are involved in its occurrence. It presents with painful erythema at the corners of the mouth (Figure 5). Both candida and the bacterium Staphylococcus aureus have been implicated7 and there is usually a high candida load intra-orally.3
Figure 5. Bilateral angular cheilitis.
Angular cheilitis can also present as a result of iron deficiency anaemia. It is commonly seen in cases of orofacial granulomatosis or as an oral manifestation of Crohn's disease.8
Median rhomboid glossitis
Median rhomboid glossitis is a candida-associated lesion characterized by an area of papillary atrophy with either a rhomboid or elliptical shape present in the midline of the dorsal tongue posteriorly (Figure 6). Usually it is a flat smooth lesion, although it can be raised and lobulated. It may be seen in children who use corticosteroid inhalers or those who are immunosuppressed.
Figure 6. Median rhomboid glossitis.
Host factors in the paediatric setting
Asthma
It is evident that the use of corticosteroid inhalers in asthma promotes oral carriage of candida which may develop into clinical infection in susceptible individuals. This usually presents as areas of erythema or, less commonly, pseudomembranous candidosis (oral thrush). Only 10–20% of the corticosteroid from an inhaler reaches the lungs, while the remainder is left in the oropharynx.9 Lesions can often be found in areas where the aerosol is deposited.10 Despite this, the presence of oral thrush is an uncommon finding in children using inhaled corticosteroids.11 The generalized immunosuppressive and anti-inflammatory effects of steroids are thought to be a factor in the pathogenesis of candidosis.12 Other factors which have been considered include the possibility that patients using inhaled corticosteroids have higher salivary glucose levels, which can promote proliferation and adhesion of candida to oral mucosal cells.13
Removable appliances
There are limited publications on the association of wearing orthodontic appliances and oral candidosis. In a review of two studies of removable appliances and three studies of fixed appliances, no subjects developed clinical oral candidosis. However, in all of the long-term studies included in this review, there was evidence of an increase in candidal carriage with both removable, or fixed, appliance orthodontic treatment.14
Clinical lesions of oral candidosis are more likely to occur in children who had a pacifier habit.15 It is possible that microscopic breaches in the oral epithelium caused by trauma from persistent sucking may predispose to candidal colonization.16 Other factors involved include the reduction in the flushing effect of saliva on the oral mucosa and the provision of surfaces for biofilm formation in both fixed and removable appliances.14
Reduced salivary flow
Increased oral carriage of candida occurs in patients whose salivary flow rates are reduced. This is due to the reduced flushing action of saliva which contains lactoferrin, lysozyme, lactoperoxidase and IgA which act to minimize colonization of the oral mucosa by inhibiting candidal adhesion to epithelial cells and assisting in phagocytosis of candida.17
Causes of reduced salivary flow rate in children include the use of xerogenic medications and diabetes mellitus. In asthmatics, the use of B2 agonists and corticosteroid inhalers may also reduce salivary flow rate.18
Salivary flow rate may also be diminished in Sjögren's syndrome, following radiation therapy or during cytotoxic therapy. Radiotherapy to the head and neck will cause alterations to the oral mucosa after 10 Gy, with often permanent damage to the salivary glands after 30 Gy.19 The outcome is best in those patients whose radiation field does not involve the parotids. Dry mouth due to chemotherapy is usually temporary and tends to resolve within 48 hours.20
Sjögren's syndrome is a chronic autoimmune disease characterized by lymphocytic infiltration and destruction of exocrine glands. Involvement of the salivary and lacrimal glands leads to both dry eyes and dry mouth. It is more common in women than in men (9:1) with an onset usually between the ages of 40–50. It is a rare condition in children, and when diagnosed usually presents as recurrent swellings of the parotid glands.21 Dry mouth and dry eye symptoms were reported less frequently.
Congenital salivary gland disease in the form of hypoplasia or aplasia is rare. It can affect one, several or all of the salivary glands and may be associated with other congenital facial malformations such as Treacher Collins syndrome or hemifacial microsomy.21
Diabetes mellitus
A review of oral candidosis in diabetes mellitus22 notes varying rates of oral carriage of candida in diabetics from 18–80% reported in the literature. Salivary flow rate and pH of saliva of diabetic patients are generally lower than in non-diabetic controls,23 with hyposalivation more common in poorly controlled diabetics.24
Other factors involved in predisposing diabetics to oral candidosis include defective candicidal activity of neutrophils and potentially higher salivary glucose levels, which may alter the cell surface receptors involved in the adherence of candida.25
Nutritional deficiencies
Numerous nutritional factors have been considered with regards to oral candidosis, including iron and vitamin deficiencies and carbohydrate rich diets.
A number of mechanisms have been proposed for oral candidosis in iron deficiency:17
Epithelial abnormalities;
Depression of cell-mediated immunity;
Defective phagocytosis;
Inadequate antibody production.
Folate and B12 have been implicated in the pathogenesis of oral candida infections.26 It is proposed that such deficiencies could affect the integrity of the oral mucosa, making candida colonization more likely, which would also be compounded by a generalized deficiency state.
There is limited evidence to support higher rates of the candida carriage in malnourished children compared to otherwise healthy children, with conflicting results in some studies.26
Antimicrobial use
The use of broad-spectrum antimicrobials, in particular tetracyclines and, to a lesser degree, metronidazole and ampicillin, are associated with oral candidosis.27 In the paediatric setting tetracyclines can be used in the treatment of acne vulgaris which most commonly presents in puberty.28 Of note, tetracycline can cause permanent staining of the dentition if prescribed prior to the age of 8 years, when permanent teeth are still undergoing mineralization.29
The oral lesion typical of candida overgrowth related to antibiotic use is acute erythematous candidosis.
A possible mechanism for candidal overgrowth following broad-spectrum antimicrobial use involves a reduction in the normal oral bacteria which would otherwise inhibit the adherence of candida to the oral mucosa and also compete with candida for nutrients.27
Malignancy
The most common cancers in children are lymphoblastic and myeloid leukaemia, retinoblastoma, neuroblastoma and Ewing sarcoma. These are commonly treated with cytotoxic therapy alone or combined with radiotherapy.30
Oral candidosis in these patients is multifactorial in origin and often relates to treatment:
Mucositis as a result of cytotoxic and radiotherapy;
Use of broad spectrum antimicrobials and corticosteroids;
Reduced salivary flow caused by both cytotoxic and radiotherapy.
Oral candidal lesions in these patients typically presents as a chronic erythematous candidosis or as a pseudomembranous candidosis.31
The oral mucosa is also affected by complications that arise from chronic graft versus host disease, which can occur following haematopoietic cell transplantation (HCT) used in the treatment of haematologic malignancies.19 Inflammatory infiltration of the salivary gland leads to reduced salivary flow which can subsequently lead to increased carriage of oral candida.
Human immunodeficiency virus (HIV)
Candida lesions commonly associated with HIV infection in children include pseudomembranous candidosis, erythematous candidosis and angular cheilitis.32
Interestingly, oral candidosis may be the first manifestation of HIV and is the most commonly reported lesion in HIV-infected children.33
The use of anti-retroviral therapy (ART) has significantly reduced HIV-related oral manifestations. Lower rates of candida-related oral lesions have been reported in children on ART compared to those not on this treatment.33
Diagnosis and management
It is essential that a thorough medical and dental history is carried out with a focus on the numerous predisposing factors in oral candidosis. The clinical examination will often lead to a diagnosis due to the typical appearance of lesions resulting from oral candidosis. In both the diagnosis and management of oral candidosis in children, a multidisciplinary approach may be required, often necessitating liaison with the general medical practitioner and/or referral to an oral medicine unit.
Use of oral swabs and/or rinse can be helpful to confirm a diagnosis, as may a smear or imprint if available. However, as noted previously, isolation of candida from the oral mucosa does not equate to oral candidosis. Use of oral rinse allows a quantitative analysis of candida burden. Normal carriage in 50% of the population is less than 1,000 cfu/ml.8
Additionally, blood investigations include FBC, haematinic assessment and blood glucose assessment may be arranged and, in some cases of persistent oral candidosis in the absence of obvious predisposing causes, assessment of HIV status may be warranted.
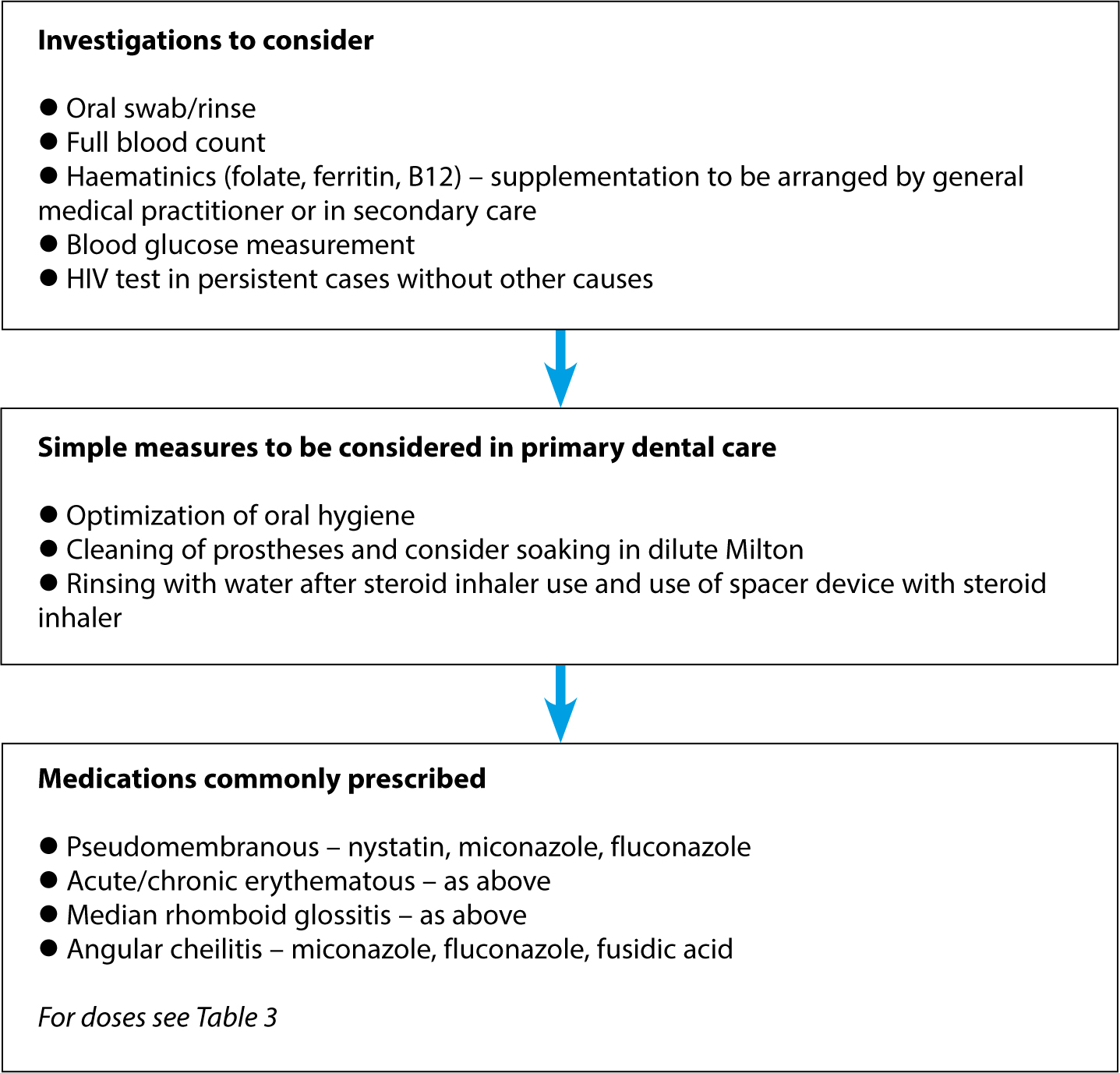
A synopsis of investigations which would be carried out in secondary care, or by the general medical practitioner and management, is summarized in the flowchart (Figure 7).
Figure 7. Investigation and management of oral candidosis in children.
The management of oral candidosis firstly involves rectifying any predisposing factors. In cases of corticosteroid inhaler use, advice on rinsing or toothbrushing, after use of the inhaler and the use of a spacer device with it may prove helpful.12
Where a diagnosis of diabetes is involved, optimization of blood sugar control is necessary to assist with resolution of oral candidosis. Any causes of anaemia will need to be further assessed and managed accordingly and, in some cases, iron and vitamin supplementation may be necessary.
Good oral hygiene will reduce the candida load intra-orally and the use of a chlorhexidine gluconate mouthwash has anti-candidal activity.3 It should be noted that chlorhexidine renders Nystatin ineffective and these should not be used together.
The two classes of antifungal medications which can be prescribed are the polyenes and the azoles. Polyenes have a fungicidal action and include nystatin and amphotericin (Table 3). Azole medications are fungistatic and the most commonly prescribed in this group include fluconazole and miconazole (Table 3.) Primary care practitioners may consider prescription of topical preparations in an otherwise healthy child. Systemic medications are best managed in secondary care.
Drug
Dose
Directions for Use
Notes
Nystatin oral suspension
100,000 units/ml
1ml four times daily for 7 days
To take after foodSuspension to be retained near lesion for 5 minutes before swallowing
Miconazole Gel
24 mg/ml
4 months–2 years:2.5 ml twice daily2–6 years:5 ml twice dailyOver 6 years:5 ml four times daily
Retain near lesions before swallowingContinue use for 2 days after lesion has resolvedTo take after food
Fluconazole/Fluconazole Oral Suspension
50 mg/50 mg/5 ml
6 months–12 years:3–6 mg/kg on first day and then 3 mg/kg (max 100 mg) daily12–18 years:50 mg daily
Administer for maximum of 14 days
Certain medications can prove helpful in specific candidal lesions. In cases of angular cheilitis, the use of miconazole gel or ointment or fusidic acid, either alone or in combination with hydrocortisone in cream or ointment form, can be used for a short period to reduce inflammation.
In cases of recalcitrant oral candidosis, the option of using antifungal treatment prophylactically can be considered. It should be noted that some oral candida species such as C. glabrata and C. krusei are innately less susceptible to azoles than other candida species and that C. albicans can develop resistance to azoles.34
Conclusion
Although oral candidosis in children is uncommon, when it does occur it often presents with pathognomic signs and symptoms. In these cases it is important to consider both local and host factors relevant in the paediatric setting which may predispose to onset. If a general dental practitioner identifies features typical of oral candidosis, referral to an oral medicine unit should be considered if simple measures do not lead to resolution.